Explain mediastinum anatomy everything
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from Gray's Anatomy for Students. Let me compile the full, detailed answer.
Mediastinum - Complete Anatomy
Source: Gray's Anatomy for Students
Overview and Definition
The mediastinum is a thick midline partition within the thoracic cavity. It extends:
- Anteriorly: from the sternum
- Posteriorly: to the thoracic vertebrae
- Superiorly: from the superior thoracic aperture
- Inferiorly: to the inferior thoracic aperture (diaphragm)
The pleural cavities lie on either side of it, one on the right and one on the left.
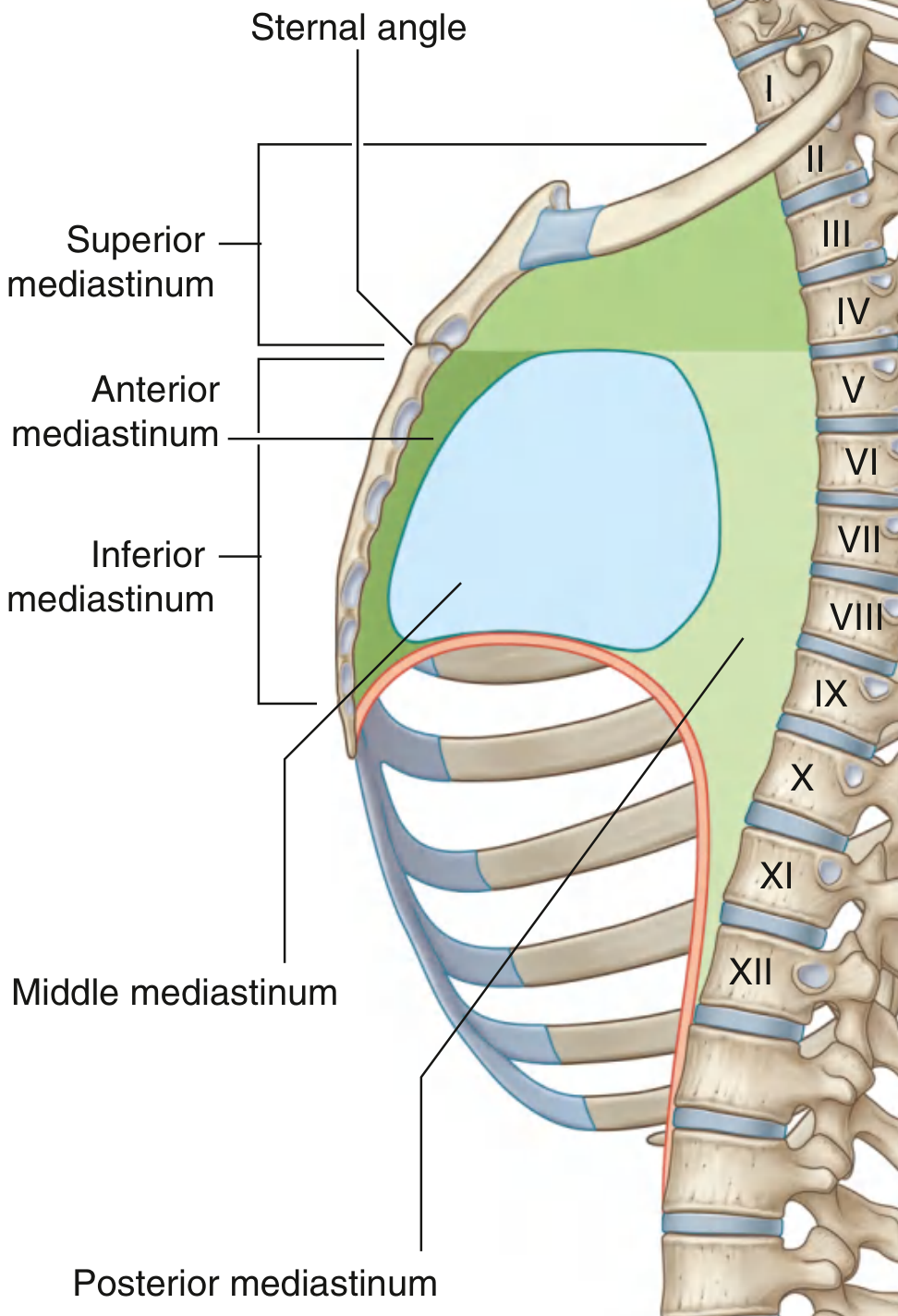
Fig. 3.59 - Subdivisions of the Mediastinum (Gray's Anatomy for Students)
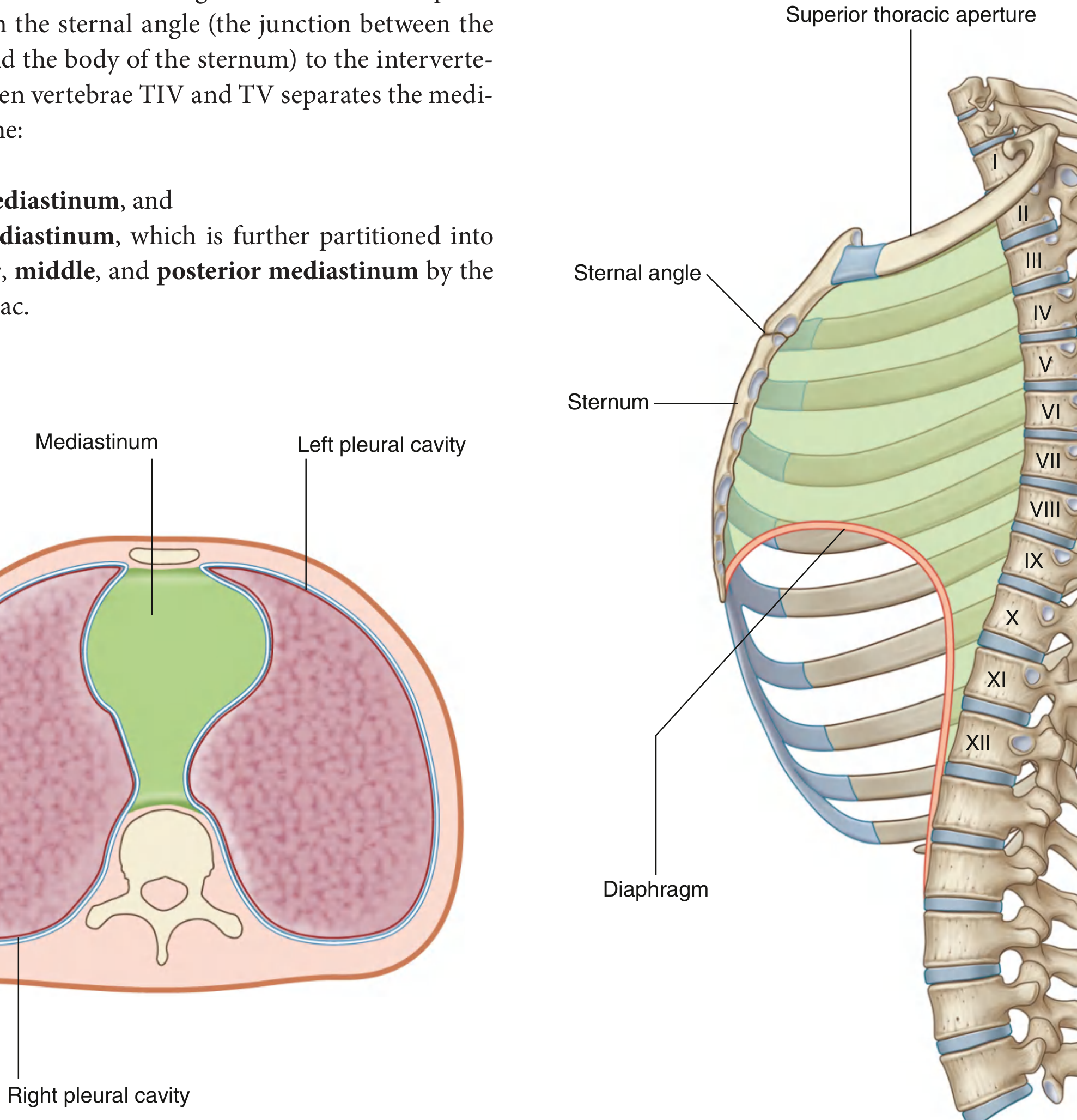
Fig. 3.57/3.58 - Cross-Section of the Thorax and lateral view
Subdivisions
A horizontal plane through the sternal angle (manubriosternal joint) and the intervertebral disc between TIV and TV divides the mediastinum into two major parts:
| Division | Location |
|---|---|
| Superior mediastinum | Above the sternal angle plane |
| Inferior mediastinum | Below the sternal angle plane |
The inferior mediastinum is further divided by the pericardial sac into:
| Subdivision | Position |
|---|---|
| Anterior mediastinum | Between sternum and pericardium (in front) |
| Middle mediastinum | The pericardium + heart themselves |
| Posterior mediastinum | Between pericardium and thoracic vertebrae (behind) |
1. Superior Mediastinum
Boundaries
- Anterior: manubrium of the sternum
- Posterior: bodies of T1-T4 vertebrae
- Superior: oblique plane from the jugular notch upward and posteriorly to the superior border of T1 (communicates with the neck)
- Inferior: horizontal plane at the sternal angle / TIV-TV disc
- Lateral: mediastinal parietal pleura on each side
Contents (in order from anterior to posterior)
1. Thymus
- Most anterior structure in the superior mediastinum
- Lies immediately posterior to the manubrium
- Bilobed, asymmetrical; may extend into the neck up to the thyroid gland, and inferiorly into the anterior mediastinum over the pericardial sac
- Vital in early immune development; involutes after puberty and is largely replaced by fat in adults
- Blood supply: small branches from internal thoracic arteries
- Venous drainage: mainly into the left brachiocephalic vein
- Lymphatics drain to parasternal nodes, tracheobronchial nodes, and neck nodes
2. Brachiocephalic Veins
- Posterior to the thymus
- Both form at the junction of the internal jugular and subclavian veins
- Right brachiocephalic vein: short, passes vertically downward
- Left brachiocephalic vein: longer, crosses the midline posterior to the manubrium (lies above the manubrium in children - clinically important for procedures)
- The two unite to form the superior vena cava (SVC) posterior to the right first costal cartilage
3. Superior Vena Cava (SVC)
- Formed by the union of the two brachiocephalic veins
- Descends on the right side to enter the right atrium
- The azygos vein arches over the root of the right lung to drain into the SVC
4. Arch of the Aorta
Three major branches arise from the aortic arch:
- Brachiocephalic trunk (right side) - divides into right common carotid + right subclavian arteries
- Left common carotid artery
- Left subclavian artery - major blood supply to the left upper limb
Ligamentum arteriosum: connects the pulmonary trunk to the arch of the aorta; remnant of the fetal ductus arteriosus (which shunted blood past the unexpanded lungs in fetal life)
5. Trachea
- Descends in the midline, slightly to the right of center
- Bifurcates at the level of the sternal angle (TIV/TV) into the right and left main bronchi - the carina is the internal ridge at bifurcation
- Right main bronchus is wider, shorter, and more vertical than the left (hence foreign bodies preferentially go right)
6. Esophagus
- Passes through the posterior part of the superior mediastinum
- Lies posterior to the trachea
- Continues into the posterior mediastinum
7. Nerves
- Phrenic nerves (C3, C4, C5): pass through the superior mediastinum and descend into the thorax
- Vagus nerves (CN X): descend through the superior mediastinum; the left recurrent laryngeal nerve loops around the arch of the aorta (at the ligamentum arteriosum) and ascends back to the larynx - this is why left-sided mediastinal masses can cause hoarseness
- Left superior intercostal vein also present
8. Thoracic Duct
- The main lymphatic channel of the body
- Runs through the superior mediastinum
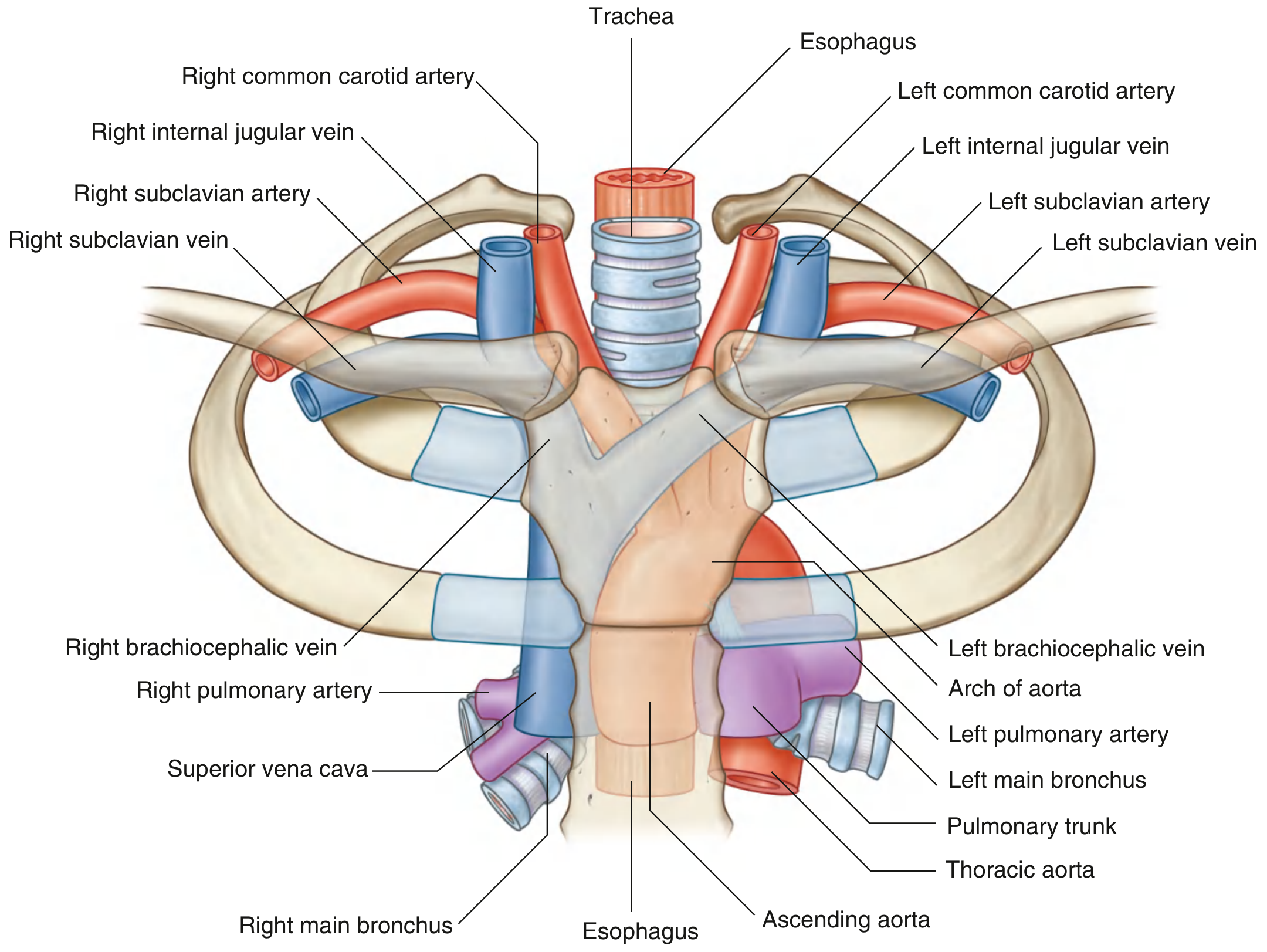
Fig. 3.89 - Structures in the Superior Mediastinum (Gray's Anatomy for Students)
2. Anterior Mediastinum
Boundaries
- Anterior: posterior surface of the body of the sternum
- Posterior: anterior surface of the pericardial sac
- Superior: the TIV/TV plane (the sternal angle level) - separates it from the superior mediastinum
- Inferior: diaphragm
- Lateral: mediastinal parietal pleura
Contents
- Inferior extension of the thymus gland (major structure)
- Fatty connective tissue
- Lymph nodes
- Mediastinal branches of the internal thoracic vessels
- Sternopericardial ligaments: pass from the posterior surface of the sternum to the fibrous pericardium, helping hold the heart in position
This is the smallest of the four compartments. Clinically, anterior mediastinal masses are classically recalled as the "4 T's": Thymoma, Teratoma (germ cell tumour), Terrible lymphoma, and Thyroid (retrosternal).
3. Middle Mediastinum
Contents
The middle mediastinum is the centrally located compartment. It contains:
Pericardium
The pericardium is a fibroserous sac enclosing the heart and roots of the great vessels. It has two layers:
- Fibrous pericardium (outer): tough connective tissue, defines the middle mediastinum boundaries; attached to the diaphragm inferiorly, and continuous with the adventitia of the great vessels superiorly
- Serous pericardium (inner): thin, two-layered:
- Parietal layer: lines the inner fibrous pericardium
- Visceral layer (epicardium): adheres to the heart surface
The pericardial cavity is the narrow potential space between parietal and visceral serous layers. It contains a small amount of serous fluid (15-50 mL) that lubricates cardiac movement.
Pericardial sinuses (clinically important):
- Transverse pericardial sinus: passage behind the ascending aorta and pulmonary trunk, and in front of the SVC and pulmonary veins. Surgeons can place a finger through it to control aortic and pulmonary trunk bleeding.
- Oblique pericardial sinus: a blind recess posterior to the left atrium, between the pulmonary veins. It is accessed from below. Fluid can accumulate here and not be detected by standard pericardiocentesis.
The Heart
The heart lies obliquely in the middle mediastinum. Its surfaces are:
- Anterior (sternocostal) surface: mainly the right ventricle
- Posterior (base): mainly the left atrium, receiving the four pulmonary veins
- Inferior (diaphragmatic) surface: right and left ventricles
- Right border: right atrium
- Left border: left ventricle and auricle
Great Vessels (roots)
- Ascending aorta (exits left ventricle)
- Pulmonary trunk (exits right ventricle)
- Superior vena cava (enters right atrium)
- Pulmonary veins (enter left atrium)
- Inferior vena cava (enters right atrium - short intrapericardial course)
Nerves in the Middle Mediastinum
- Phrenic nerves (from C3, C4, C5): descend between the pericardium and the mediastinal pleura, providing motor supply to the diaphragm and sensory supply to the pericardium, mediastinal pleura, and diaphragm
4. Posterior Mediastinum
Boundaries
- Anterior: pericardial sac and diaphragm
- Posterior: mid-to-lower thoracic vertebral bodies (T5-T12)
- Superior: TIV/TV disc level
- Inferior: diaphragm
- Lateral: mediastinal parietal pleura
Contents
1. Esophagus
- Muscular tube from pharynx (CVI) to stomach (TXI gastro-esophageal junction)
- Descends through the thorax in a midline position, then deviates anteriorly and to the left as it approaches the diaphragm
- Passes through the esophageal hiatus at vertebral level TX
- Relations in the posterior mediastinum:
- Right side: covered by mediastinal pleura
- Left side: related to the thoracic aorta
- Anterior: right pulmonary artery, left main bronchus, then the left atrium (important - atrial enlargement causes dysphagia)
- Posterior: thoracic duct (crosses from right to left), hemizygos veins, posterior intercostal vessels
- Surrounded by the esophageal nerve plexus (from vagus nerves); just above the diaphragm these converge into the anterior vagal trunk (mainly left vagus) and posterior vagal trunk (mainly right vagus)
2. Thoracic Aorta
- Begins at the lower border of TIV (continuation of the aortic arch)
- Ends at TXII, passing through the aortic hiatus (posterior to the diaphragm, between the crura) to become the abdominal aorta
- Initially lies to the left of the vertebral column, then moves to the midline inferiorly
Branches of the thoracic aorta:
| Branch | Description |
|---|---|
| Posterior intercostal arteries (×9 pairs) | Supply lower 9 intercostal spaces (first 2 from supreme intercostal artery) |
| Bronchial arteries | 2 left (from thoracic aorta), 1 right (usually from 3rd intercostal) |
| Esophageal arteries (4-5) | Form a continuous anastomotic chain on the esophagus |
| Pericardial branches | Small vessels to posterior pericardium |
| Mediastinal branches | Supply lymph nodes, nerves, areolar tissue |
| Superior phrenic arteries | Supply posterior superior diaphragm |
| Subcostal artery | Below rib XII |
3. Azygos System of Veins
- A series of longitudinal vessels on each side of the vertebral column that drain the body wall and thoracic viscera into the SVC
- Serves as an important collateral pathway if the inferior vena cava is obstructed (blood from lower limbs can drain via ascending lumbar veins into the azygos system and reach the SVC)
- Azygos vein (right side): ascends to arch over the root of the right lung at T4, draining into the SVC
- Hemi-azygos vein (left side): runs along the left side of lower thoracic vertebrae
- Accessory hemi-azygos vein: above the hemi-azygos, on the left
- Cross-connections exist between all three vessels
4. Thoracic Duct
- The main lymphatic vessel of the body; drains all lymph below the diaphragm and from the left side of the body above
- Begins in the abdomen as the cisterna chyli at the level of L1-L2
- Enters the thorax through the aortic hiatus
- Ascends on the right side of the vertebral column in the lower posterior mediastinum, posterior to the esophagus
- Crosses to the left at around T4-T5
- Exits the thorax by passing into the neck and empties into the junction of the left subclavian and left internal jugular veins
- Injury (e.g., during esophagectomy or chest trauma) causes a chylothorax
5. Sympathetic Trunks
- Two chains of ganglia lying lateral to the vertebral bodies
- Each thoracic sympathetic trunk has 10-12 ganglia
- Provide sympathetic innervation to the thoracic viscera and body wall
6. Thoracic Splanchnic Nerves
- Arise from the sympathetic trunks
- Greater splanchnic nerve (T5-T9): passes through the crura of the diaphragm to the celiac ganglion
- Lesser splanchnic nerve (T10-T11): to the aorticorenal ganglion
- Least splanchnic nerve (T12): to the renal plexus
- Convey pre-ganglionic sympathetic fibers to the abdominal viscera and visceral afferent (pain) fibers
Clinical Correlations
| Structure | Clinical Relevance |
|---|---|
| Left recurrent laryngeal nerve (loops around aortic arch) | Hoarseness from aortic aneurysm, left lung cancer, or lymph node enlargement |
| Left brachiocephalic vein (above manubrium in children) | Risk of injury during midline neck procedures in pediatric patients |
| Esophagus adjacent to left atrium | Left atrial enlargement (e.g., mitral stenosis) causes dysphagia |
| Esophageal hiatus at TX | Hiatus hernia - stomach herniates into chest |
| Phrenic nerve | Injury causes ipsilateral diaphragm paralysis (elevated hemidiaphragm on CXR) |
| SVC obstruction | SVC syndrome: facial oedema, arm swelling, dilated neck veins |
| Azygos vein | Collateral for IVC obstruction; azygos lobe (anatomical variant) |
| Aortic dissection | Fixed points (aortic valve ring, ligamentum arteriosum, median arcuate ligament) are sites of trauma |
| Coarctation of the aorta | Narrowing just distal to the left subclavian artery; rib notching on CXR from intercostal collaterals |
| Thoracic duct injury | Chylothorax (milky pleural fluid rich in chylomicrons) |
| Transverse pericardial sinus | Cardiac surgeons pass ligature here to clamp aorta/pulmonary trunk |
Summary Table: Four Compartments at a Glance
| Compartment | Key Boundary | Major Contents |
|---|---|---|
| Superior | Above sternal angle (TIV/TV) | Thymus, SVC, brachiocephalic veins, aortic arch + 3 branches, trachea, esophagus, thoracic duct, phrenic nerves, vagus nerves, left recurrent laryngeal nerve |
| Anterior | Behind sternum, in front of pericardium | Thymus (inferior extension), fat, lymph nodes, sternopericardial ligaments, internal thoracic vessels |
| Middle | The pericardial sac itself | Pericardium, heart, ascending aorta (root), pulmonary trunk (root), SVC, pulmonary veins, IVC (short segment), phrenic nerves |
| Posterior | Behind pericardium, in front of T5-T12 | Esophagus, thoracic aorta, azygos/hemiazygos veins, thoracic duct, sympathetic trunks, thoracic splanchnic nerves |
- Gray's Anatomy for Students, pp. 165-166, 220, 252-268
Genarte mcqs
Here are 25 high-yield MCQs on Mediastinum Anatomy — exam-style, with answers and explanations:
🧠 Mediastinum Anatomy - MCQs
Q1. The mediastinum is divided into superior and inferior parts by a plane passing through which of the following?
- A) Jugular notch and T1
- B) Sternal angle and TIV/TV intervertebral disc
- C) Xiphoid process and TVIII
- D) Manubriosternal joint and TIII
✅ Answer: B
The sternal angle (angle of Louis) corresponds to the TIV/TV disc level. This horizontal plane is the key landmark dividing the mediastinum into superior and inferior parts.
Q2. Which of the following structures is the MOST anterior in the superior mediastinum?
- A) Trachea
- B) Arch of aorta
- C) Thymus
- D) Esophagus
✅ Answer: C
The thymus is the most anterior structure, lying immediately posterior to the manubrium. The order front to back is: Thymus → Brachiocephalic veins → Aortic arch → Trachea → Esophagus.
Q3. A 65-year-old patient develops sudden hoarseness after being diagnosed with a left-sided lung mass. Which nerve is most likely compressed?
- A) Right recurrent laryngeal nerve
- B) Left phrenic nerve
- C) Left recurrent laryngeal nerve
- D) Left vagus nerve at the jugular foramen
✅ Answer: C
The left recurrent laryngeal nerve loops under the arch of the aorta at the ligamentum arteriosum, making it vulnerable to compression by left-sided mediastinal and lung masses. The right RLN loops around the subclavian artery in the neck and is not in the mediastinum.
Q4. Which structure passes through the esophageal hiatus of the diaphragm?
- A) Thoracic duct
- B) Azygos vein
- C) Thoracic aorta
- D) Esophagus, anterior and posterior vagal trunks
✅ Answer: D
The esophageal hiatus (at TX) transmits the esophagus plus the anterior and posterior vagal trunks. The aorta passes through the aortic hiatus (TXII), and the IVC through the caval opening (TVIII).
Q5. The left brachiocephalic vein is clinically important in children because it:
- A) Drains directly into the azygos vein
- B) Passes above the superior border of the manubrium
- C) Contains valves that can obstruct blood flow
- D) Receives the thoracic duct
✅ Answer: B
In infants and children, the left brachiocephalic vein rises above the manubrium and is therefore less protected by bone, making it vulnerable during midline neck procedures. In adults, it passes posterior to the manubrium.
Q6. Which of the following is NOT a content of the posterior mediastinum?
- A) Thoracic duct
- B) Azygos vein
- C) Phrenic nerve
- D) Thoracic aorta
✅ Answer: C
The phrenic nerves (C3, C4, C5) descend between the pericardium and the mediastinal pleura, making them contents of the middle mediastinum (and superior mediastinum). They are NOT in the posterior mediastinum.
Q7. A patient with mitral stenosis and marked left atrial enlargement presents with difficulty swallowing. Which structure is being compressed?
- A) Trachea
- B) Esophagus
- C) Superior vena cava
- D) Left main bronchus
✅ Answer: B
The esophagus lies immediately posterior to the left atrium in the posterior mediastinum, separated only by pericardium. Significant left atrial enlargement can compress the esophagus, causing dysphagia.
Q8. The thoracic duct crosses from the right side to the left side of the vertebral column at which vertebral level?
- A) T1-T2
- B) T4-T5
- C) T8-T9
- D) T12-L1
✅ Answer: B
The thoracic duct ascends on the right side in the lower posterior mediastinum, then crosses the midline to the left at approximately T4-T5. It then ascends on the left side and exits the thorax to drain into the left venous angle (junction of left subclavian and internal jugular veins).
Q9. Which compartment of the mediastinum contains the sternopericardial ligaments?
- A) Superior mediastinum
- B) Posterior mediastinum
- C) Anterior mediastinum
- D) Middle mediastinum
✅ Answer: C
Sternopericardial ligaments pass from the posterior surface of the sternum to the fibrous pericardium. They are contents of the anterior mediastinum along with the thymus extension, fat, lymph nodes, and internal thoracic vessel branches.
Q10. The transverse pericardial sinus lies between which structures?
- A) Posterior to the left atrium, between the pulmonary veins
- B) Behind the ascending aorta/pulmonary trunk and in front of the SVC/pulmonary veins
- C) Between the fibrous and serous layers of pericardium
- D) Between the right and left atria
✅ Answer: B
The transverse pericardial sinus is a passage posterior to the ascending aorta and pulmonary trunk, and anterior to the SVC and pulmonary veins. Cardiac surgeons use it to place clamps on these vessels. (The oblique sinus is posterior to the left atrium — option A.)
Q11. Which of the following correctly describes the aortic hiatus of the diaphragm?
- A) Located at TX, transmits esophagus
- B) Located at TVIII, transmits IVC
- C) Located at TXII, posterior to the diaphragm between the crura
- D) Located at TIX, transmits thoracic duct
✅ Answer: C
The aortic hiatus is at TXII and lies posterior to the diaphragm (between the two crura), so it is technically behind the diaphragm, not a true hole through it. It transmits the thoracic aorta and the thoracic duct. Mnemonic: I 8 (ate) 10 eggs at 12 — IVC T8, Esophagus T10, Aorta T12.
Q12. The azygos vein drains into which structure?
- A) Inferior vena cava
- B) Right atrium directly
- C) Superior vena cava
- D) Left brachiocephalic vein
✅ Answer: C
The azygos vein arches over the root of the right lung at approximately T4 to drain into the posterior aspect of the superior vena cava. It is an important collateral when the IVC is obstructed.
Q13. A foreign body is aspirated and lodges in a bronchus. In which bronchus is it most likely to go?
- A) Left main bronchus, because it is wider
- B) Right main bronchus, because it is wider, shorter, and more vertical
- C) Either side equally
- D) Left main bronchus, because it is longer
✅ Answer: B
The right main bronchus is wider, shorter, and more vertical than the left. Foreign bodies preferentially enter the right side. Within the right lung, objects most commonly lodge in the right lower lobe bronchus.
Q14. The ligamentum arteriosum connects which two structures?
- A) Ascending aorta to the SVC
- B) Pulmonary trunk to the arch of the aorta
- C) Ductus venosus to the portal vein
- D) Left subclavian artery to the left pulmonary artery
✅ Answer: B
The ligamentum arteriosum is the fibrous remnant of the fetal ductus arteriosus, connecting the pulmonary trunk to the arch of the aorta. It closes soon after birth. The left recurrent laryngeal nerve loops around it.
Q15. Which of the following is the vertebral level at which the trachea bifurcates?
- A) TII/TIII
- B) TIV/TV (sternal angle level)
- C) TVII
- D) CI/CII
✅ Answer: B
The trachea bifurcates at the carina at the level of the sternal angle, which corresponds to the TIV/TV intervertebral disc. This is the same landmark that separates the superior from the inferior mediastinum.
Q16. In which mediastinal compartment would you find the oblique pericardial sinus?
- A) Anterior mediastinum
- B) Superior mediastinum
- C) Middle mediastinum
- D) Posterior mediastinum
✅ Answer: C
Both pericardial sinuses (transverse and oblique) are within the pericardial sac, which is the middle mediastinum. The oblique sinus is a blind recess posterior to the left atrium between the pulmonary veins.
Q17. Injury to the thoracic duct (e.g., during esophagectomy) results in:
- A) Hemothorax
- B) Pneumothorax
- C) Chylothorax
- D) Empyema
✅ Answer: C
Thoracic duct injury causes a chylothorax — accumulation of milky, chylomicron-rich lymph in the pleural cavity. It typically appears on the left side because the thoracic duct runs on the left side of the upper posterior mediastinum.
Q18. The right brachiocephalic vein receives all of the following tributaries EXCEPT:
- A) Right internal thoracic vein
- B) Right vertebral vein
- C) Left superior intercostal vein
- D) First posterior intercostal vein (right)
✅ Answer: C
The left superior intercostal vein drains into the left brachiocephalic vein, not the right. All the other listed veins are tributaries of the right brachiocephalic vein.
Q19. In coarctation of the aorta, the narrowing typically occurs:
- A) Proximal to the origin of the left subclavian artery
- B) Just distal to the origin of the left subclavian artery
- C) At the aortic valve
- D) At the level of the ligamentum arteriosum proximally, before the left subclavian
✅ Answer: B
Coarctation of the aorta is a congenital narrowing just distal to the origin of the left subclavian artery, near the ligamentum arteriosum. Blood supply to the lower body is reduced and collaterals develop via the intercostal arteries, causing rib notching on chest X-ray.
Q20. Which nerve supplies motor fibers to the diaphragm AND provides sensory fibers to the pericardium?
- A) Vagus nerve
- B) Intercostal nerves (T7-T12)
- C) Phrenic nerve
- D) Greater splanchnic nerve
✅ Answer: C
The phrenic nerve (C3, C4, C5 - "C3, 4, 5 keeps the diaphragm alive") provides motor supply to the diaphragm and sensory fibers to the central diaphragm, pericardium, and mediastinal pleura. Referred pain from the diaphragm goes to the shoulder (C4 distribution).
Q21. Which of the following structures is anterior to the esophagus at the level below the tracheal bifurcation?
- A) Thoracic aorta
- B) Thoracic duct
- C) Left atrium
- D) Azygos vein
✅ Answer: C
Below the tracheal bifurcation, the esophagus is immediately posterior to the left atrium (separated only by pericardium). This is why atrial enlargement causes dysphagia and why transesophageal echocardiography gives excellent views of the left atrium.
Q22. The greater splanchnic nerve arises from which thoracic sympathetic ganglia?
- A) T1-T4
- B) T5-T9
- C) T10-T11
- D) T12
✅ Answer: B
The greater splanchnic nerve arises from T5-T9 ganglia and passes through the diaphragmatic crura to the celiac ganglion. The lesser splanchnic is T10-T11 (to aorticorenal ganglion), and the least splanchnic is T12 (to the renal plexus).
Q23. Which statement about the thymus is CORRECT?
- A) It is largest in the elderly adult
- B) Venous drainage is mainly into the right brachiocephalic vein
- C) It develops from the third pharyngeal pouch
- D) It is the most posterior structure in the superior mediastinum
✅ Answer: C
The thymus develops from the third pharyngeal pouch (same as the inferior parathyroid glands), making it a common site for ectopic parathyroid tissue. It is the most anterior structure (not posterior), venous drainage is into the left brachiocephalic vein, and it is largest in childhood.
Q24. A trauma patient sustains a deceleration injury in a road accident. Aortic trauma is most likely at which location?
- A) At the origin of the brachiocephalic trunk
- B) At the ligamentum arteriosum
- C) At the origin of the left subclavian artery
- D) At the root of the aorta in the aortic sinus
✅ Answer: B
The aorta has three fixed points: the aortic valve ring, the ligamentum arteriosum, and the point where it passes behind the median arcuate ligament. Deceleration injuries most commonly tear the aorta at the ligamentum arteriosum (the junction of the arch and descending thoracic aorta). This is seen in high-speed MVAs.
Q25. Which of the following correctly pairs the structure with the vertebral level at which it crosses the diaphragm?
- A) IVC - T10, Esophagus - T8, Aorta - T12
- B) IVC - T8, Esophagus - T10, Aorta - T12
- C) IVC - T12, Esophagus - T8, Aorta - T10
- D) IVC - T8, Esophagus - T12, Aorta - T10
✅ Answer: B
Classic mnemonic: "I 8 (ate) 10 eggs at 12"
- IVC = T8
- Esophagus = T10
- Aorta = T12
Score Yourself
| Score | Level |
|---|---|
| 23-25 | Excellent - exam ready |
| 18-22 | Good - review weak areas |
| 13-17 | Fair - re-read the anatomy |
| < 13 | Needs focused revision |
This is a shared conversation. Sign in to Orris to start your own chat.