Amlodipine 
Reading File
Finding Sources
Searching PubMed
amlodipine calcium channel blocker hypertension
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive textbook data from Goodman & Gilman, Lippincott Pharmacology, and Brenner & Rector's Kidney. Here is the full, detailed answer:
Amlodipine
Drug Class & Chemistry
Amlodipine is a dihydropyridine (DHP) calcium channel blocker (CCB). It is a third-generation, long-acting member of this class and is available as the besylate salt (amlodipine besylate). Unlike other DHPs, amlodipine appears to bind to both dihydropyridine and non-dihydropyridine sites on the L-type calcium channel, contributing to its unique pharmacokinetic profile.
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Brenner and Rector's The Kidney
Mechanism of Action
Amlodipine blocks L-type (slow) voltage-gated calcium channels on the alpha-1 subunit. This inhibits calcium influx into:
- Vascular smooth muscle - causes arterial vasodilation, reduces systemic vascular resistance (SVR), and lowers blood pressure
- Cardiac myocytes (minor effect at therapeutic doses) - minimal negative inotropy
Key selectivity point: Amlodipine acts primarily on peripheral vascular smooth muscle, producing arteriolar vasodilation. It has minimal effect on cardiac conduction (no significant effect on heart rate, AV node, or SA node at therapeutic doses). This distinguishes it sharply from non-DHP CCBs (verapamil, diltiazem), which have strong chronotropic and dromotropic effects.
The vasodilation it produces does not significantly activate the sympathetic nervous system (unlike short-acting nifedipine), which is related to its gradual onset and long half-life. - Brenner and Rector's The Kidney
Pharmacokinetics
| Parameter | Value |
|---|---|
| Absorption | Almost complete after oral dosing |
| Time to peak plasma concentration | 6-12 hours |
| Clinical response onset | ~24 hours |
| Steady-state plasma levels | Achieved after 7-10 days of once-daily dosing |
| Elimination half-life (t½) | 30-50 hours (prolonged in elderly) |
| Protein binding | ~95% |
| Metabolism | ~90% hepatic (CYP3A4) to inactive metabolites |
| Excretion | Metabolites primarily in urine; 10% unchanged |
| Dose adjustment in renal impairment | Not required |
| Dose adjustment in hepatic impairment | May be needed (start low) |
The plasma concentration profile is characteristically flat and stable - very modest peaks and troughs - compared to the abrupt spikes seen with immediate-release nifedipine. This allows once-daily dosing and avoids reflex tachycardia.
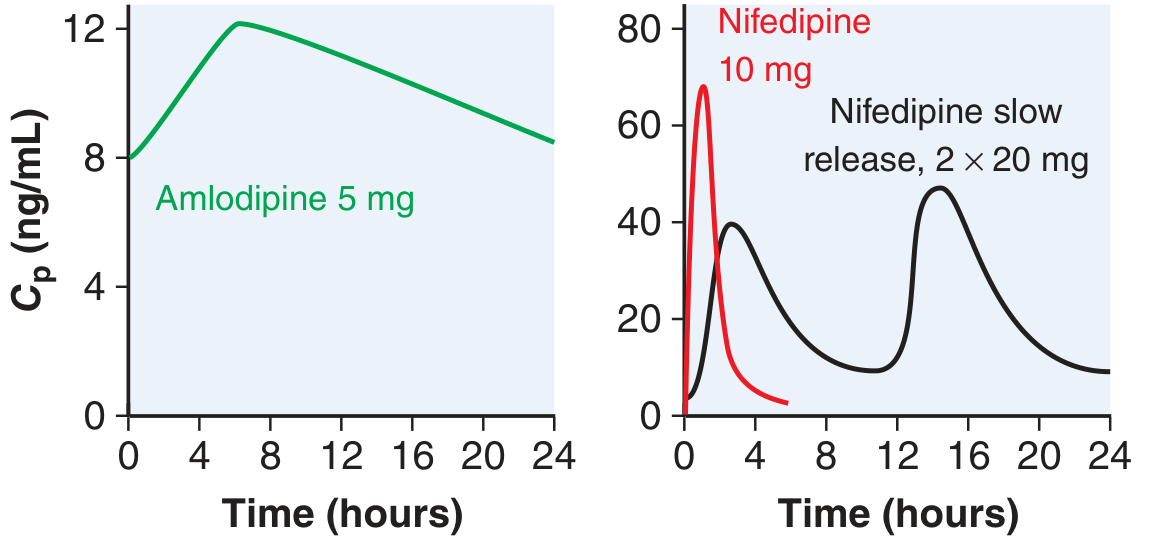
Plasma concentration (Cp) over 24 hours: Amlodipine 5 mg (left) shows a flat, stable profile; immediate-release nifedipine 10 mg (right, red) shows a sharp spike and rapid fall. - Goodman & Gilman's
Therapeutic Uses
1. Hypertension
Amlodipine is a first-line antihypertensive. It is the prototype DHP CCB for treating hypertension, and landmark trials (ALLHAT) showed it to be comparable to chlorthalidone for reducing most cardiovascular events. Importantly, its antihypertensive effect is independent of dietary sodium intake and does not require concurrent diuretic use.
2. Angina
- Variant (vasospastic / Prinzmetal's) angina: First-line treatment. CCBs are effective in ~90% of patients by relaxing coronary artery spasm.
- Stable exertional angina: Reduces myocardial O2 demand by decreasing afterload (reduces the double product: HR × systolic BP). Combining amlodipine with a beta-blocker is more effective than either alone - the beta-blocker suppresses the reflex tachycardia that amlodipine can cause.
3. Coronary artery disease (stable CAD)
Used for symptomatic relief when beta-blockers are insufficient or not tolerated. - Goodman & Gilman's, Lippincott Pharmacology
Dosing
| Indication | Dose |
|---|---|
| Hypertension | Start: 5 mg once daily; max: 10 mg/day |
| Elderly / hepatic impairment | Start: 2.5 mg once daily |
| Angina | 5-10 mg once daily |
Titrate at 7-14 day intervals due to long time to steady state (7-10 days).
Adverse Effects
| Effect | Notes |
|---|---|
| Peripheral edema | Most common; due to precapillary dilation + reflex postcapillary constriction (NOT fluid retention) |
| Headache, flushing, dizziness | Less common than short-acting DHPs due to gradual onset |
| Reflex tachycardia | Mild; much less than immediate-release nifedipine |
| Gingival hyperplasia | Rare |
| Gastroesophageal reflux | Can aggravate GERD via smooth muscle relaxation |
Unlike non-DHP CCBs (verapamil/diltiazem), amlodipine does NOT cause:
- Bradycardia or AV block
- Constipation
- Negative inotropy (clinically significant)
Contraindications / Special Situations
- Heart failure with reduced ejection fraction (HFrEF): Use with caution. Unlike verapamil/diltiazem, amlodipine does NOT have significant negative inotropy, so it is relatively safer in HFrEF than other CCBs (though not recommended for routine use in this setting).
- Severe aortic stenosis: Use cautiously (hypotension risk).
- Pregnancy: Generally avoided (limited data; non-DHP CCBs preferred for arrhythmias).
Drug Interactions
- Beta-blockers: Combination is safe and often beneficial (beta-blocker blunts reflex tachycardia from amlodipine); unlike verapamil/diltiazem, there is no additive AV block risk.
- CYP3A4 inhibitors (e.g., clarithromycin, ketoconazole, grapefruit juice): May increase amlodipine levels.
- CYP3A4 inducers (e.g., rifampicin): May decrease amlodipine levels.
- Simvastatin: Amlodipine inhibits CYP3A4-mediated metabolism of simvastatin; simvastatin dose should not exceed 20 mg/day when co-administered.
- Cyclosporine: Amlodipine may increase cyclosporine levels.
Key Distinguishing Features vs Other CCBs
| Feature | Amlodipine (DHP) | Verapamil (non-DHP) | Diltiazem (non-DHP) |
|---|---|---|---|
| Primary action | Vascular smooth muscle | Cardiac + vascular | Both (intermediate) |
| Negative inotropy | Minimal | Significant | Moderate |
| AV node effect | None | Strong (slows conduction) | Moderate |
| Reflex tachycardia | Mild | None | Minimal |
| Half-life | 30-50 h | 6-12 h | 4-9 h |
| Safe with beta-blocker | Yes | No (AV block risk) | Caution |
| Use in HFrEF | Safer | Contraindicated | Contraindicated |
Sources: - Lippincott Illustrated Reviews: Pharmacology - Goodman & Gilman's The Pharmacological Basis of Therapeutics - Brenner and Rector's The Kidney - Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.