One lung ventilation.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"one lung ventilation"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from three major anesthesia textbooks. Let me compile the full answer.
One-Lung Ventilation (OLV)
One-lung ventilation (OLV) is a technique used during thoracic surgery whereby ventilation is deliberately confined to one lung while the contralateral lung is allowed to collapse. It optimizes surgical access but creates significant physiological challenges - primarily hypoxemia and risk of lung injury.
Indications
Absolute Indications
(Lung separation is mandatory to prevent life-threatening complications)
| Category | Examples |
|---|---|
| Isolation to prevent contamination | Pulmonary abscess, infected cyst, massive hemoptysis, empyema |
| Control of ventilation distribution | Bronchopleural fistula, bronchopleural-cutaneous fistula, unilateral cyst/bullae, major bronchial disruption or trauma |
| Unilateral lung lavage | Whole-lung lavage for pulmonary alveolar proteinosis |
| Surgical exposure | Video-assisted thoracoscopic surgery (VATS) |
Relative Indications
(Facilitate surgery; OLV preferred but not mandatory)
- Thoracic aortic aneurysm repair
- Pneumonectomy, lobectomy, esophageal surgery
- Upper lobe thoracoscopic procedures
- Thoracoscopy, pleurodesis
(Barash Clinical Anesthesia 9e; Morgan & Mikhail 7e)
Physiology of OLV
The Core Problem: Obligatory Shunt
During OLV in the lateral decubitus position:
- Only the dependent (lower) lung is ventilated
- The nondependent (upper, operative) lung is collapsed but continues to receive blood flow
- This creates a right-to-left intrapulmonary shunt of 20-30%
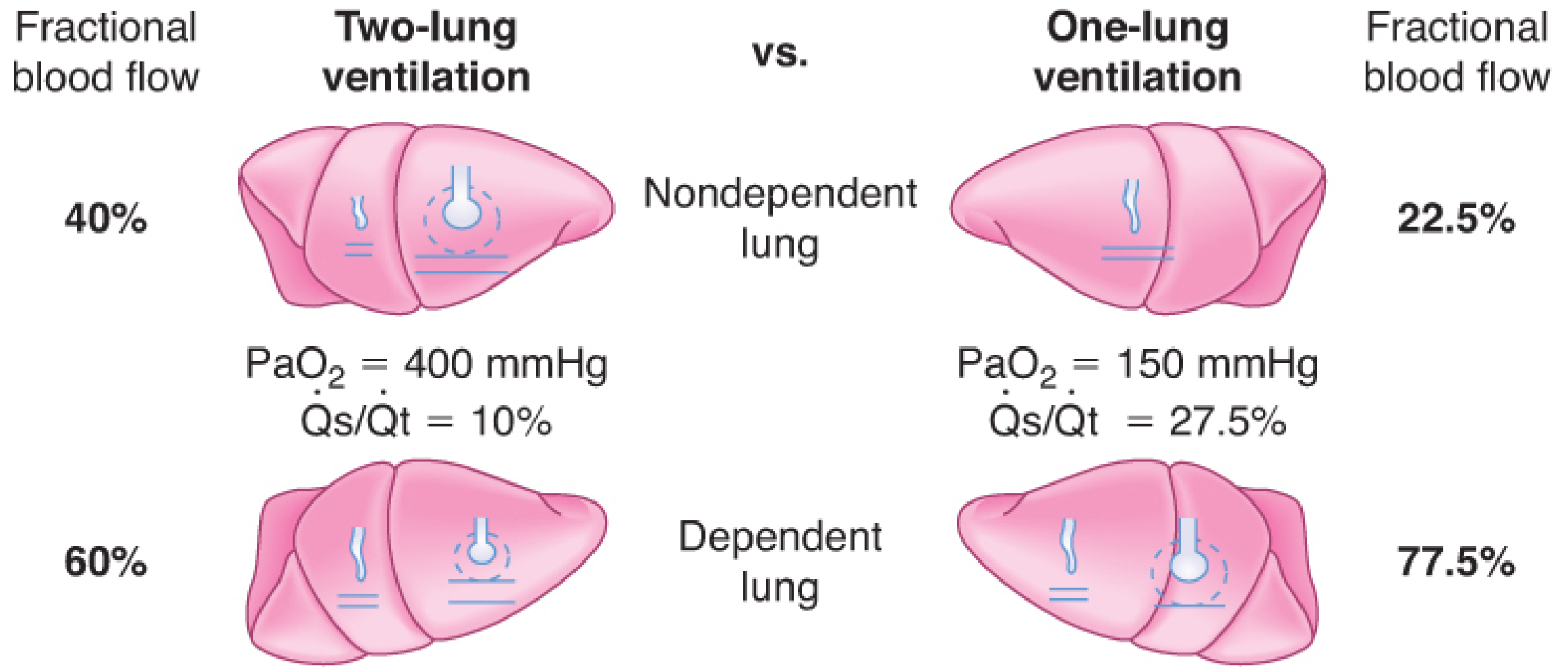
Typical values: PaO2 drops from ~400 mmHg (two-lung, FiO2 1.0) to ~150 mmHg during OLV. Qs/Qt rises from ~10% to ~27.5%. - Barash Clinical Anesthesia 9e, p. 3175
Two Main Contributors to Hypoxemia During OLV
- Persistent blood flow through the nonventilated nondependent lung - obligatory shunt
- Atelectasis in the dependent (ventilated) lung - caused by absorption atelectasis, compression, decreased FRC in lateral decubitus position
Hypoxic Pulmonary Vasoconstriction (HPV) - The Compensatory Mechanism
HPV is the critical physiological defense. When the nondependent lung collapses and becomes hypoxic, its pulmonary vasculature constricts, diverting blood flow away from the shunt lung toward the ventilated dependent lung. HPV can reduce blood flow to the collapsed lung by approximately 50%, thereby limiting the shunt.
- HPV has a biphasic response: rapid onset (minutes) and a slower phase peaking over hours
- HPV is the most important determinant of blood flow diversion away from the nonventilated lung (more so than mechanical vascular kinking)
(Miller's Anesthesia 10e, p. 7191; Barash 9e, p. 3175)
Factors That Inhibit HPV (Worsen Hypoxemia)
These increase venous admixture and shunt:
| Category | Factors |
|---|---|
| Drugs | Nitroglycerin, nitroprusside, nitric oxide (inhaled), phosphodiesterase inhibitors (milrinone), beta-agonists, calcium channel blockers |
| Inhalation agents | All volatile anesthetics (dose-dependent); halothane > enflurane > isoflurane; at 1 MAC, modern agents (isoflurane, sevoflurane, desflurane) cause only ~20% HPV inhibition |
| Physiologic | Pulmonary hypertension, hypocapnia/alkalosis, elevated mixed venous PO2, hypothermia, increased cardiac output |
| High airway pressures in ventilated lung | High PEEP, hyperventilation, high peak pressures - redirects flow to nonventilated lung |
| Low FiO2 in ventilated lung | Induces HPV in the ventilated lung, paradoxically worsening hypoxemia |
(Morgan & Mikhail 7e, p. 1024; Miller's 10e)
Techniques for Lung Isolation
Four methods are available:
1. Double-Lumen Endobronchial Tube (DLT) - Most Common
- Has one tracheal lumen and one bronchial lumen
- Allows independent ventilation, suctioning, and CPAP to each lung
- Left-sided DLT preferred in most cases - the left main bronchus is longer (5 cm vs. 2.5 cm on right), providing more margin of safety for cuff placement
- Right-sided DLT: more technically demanding; the bronchial cuff must align with the right upper lobe (RUL) ventilation slot, with only 1-8 mm margin - so right-sided DLTs are used when left bronchial intubation is contraindicated (e.g., left pneumonectomy)
- Position confirmation is mandatory with fiberoptic bronchoscopy
Common DLT Malposition Errors:
- Tube advanced too far into right or left bronchus - absent breath sounds contralaterally
- Tube not inserted far enough - bronchial cuff above carina
- Right upper lobe orifice occlusion with right-sided DLT
- Left upper lobe occlusion with deep left-sided DLT
- Bronchial cuff herniation over carina
2. Single-Lumen Tube + Bronchial Blocker
- A blocker (e.g., Arndt, Cohen, EZ-Blocker) is placed through or alongside a regular ETT
- Useful in difficult airways, tracheostomized patients, patients who need postoperative ventilation
- Allows conversion from two-lung to one-lung ventilation without tube exchange
3. Endobronchial Intubation with Single-Lumen Tube
- A standard ETT intentionally advanced into a mainstem bronchus
- Simplest but offers no ability to selectively manage the opposite lung
4. Tubeless / VATS Techniques
- Used for minimally invasive thoracoscopic procedures
- High-frequency ventilation or apneic oxygenation may be employed
(Morgan & Mikhail 7e, p. 1025)
Ventilation Strategy During OLV
Pre-OLV Preparation
- De-nitrogenate the operative (nondependent) lung by ventilating with 100% O2 before lung collapse - nitrogen's low blood solubility delays absorption atelectasis and slows collapse; pre-oxygenation speeds collapse
- Perform a recruitment maneuver of the dependent lung immediately after starting OLV (hold at ~20 cmH2O for 15-20 seconds) to reduce dependent atelectasis
Tidal Volume
- Use low tidal volumes: 4-6 mL/kg predicted body weight (not 10 mL/kg as used historically)
- Tidal volumes <3 mL/kg may cause derecruitment and worsen atelectasis
PEEP
- Apply sufficient PEEP to the ventilated dependent lung to prevent atelectasis
- Optimal PEEP is titrated to best compliance - excessive PEEP can redirect blood to the nonventilated lung and worsen oxygenation
Ventilatory Mode
- Pressure-controlled ventilation (PCV) may reduce barotrauma risk by limiting peak/plateau pressures and provides a more homogeneous tidal volume distribution
- Plateau pressure: <25 cmH2O; peak airway pressure: <35 cmH2O
FiO2
- Use FiO2 0.5-1.0; some evidence favors avoiding 100% O2 due to oxygen toxicity and absorption atelectasis concerns
- Use FiO2 of 1.0 during episodes of hypoxemia
CO2 Elimination
- Usually maintained adequately with unchanged minute ventilation
- End-tidal CO2 monitoring is useful as a trend but may underestimate PaCO2 (increased dead space)
- Permissive hypercapnia is acceptable when oxygenation is adequate
(Morgan & Mikhail 7e, p. 1024-1046; Miller's 10e, p. 7189)
Management of Hypoxemia During OLV
Acceptable SpO2 threshold: >90% (PaO2 >60 mmHg) is commonly accepted. Patients with coronary or cerebrovascular disease, anemia, or limited cardiopulmonary reserve require higher targets.
Step-wise approach:
| Step | Intervention |
|---|---|
| 1 | Confirm position of DLT or blocker by fiberoptic bronchoscopy - surgical manipulation can displace the tube |
| 2 | Suction both lumens to exclude mucus plugging |
| 3 | Increase FiO2 to 1.0 |
| 4 | Recruitment maneuver to dependent (ventilated) lung to eliminate atelectasis |
| 5 | Apply appropriate PEEP to ventilated lung |
| 6 | Apply CPAP (5-10 cmH2O) or blow-by O2 to the nonventilated (operative) lung - reduces shunt; use cautiously in VATS as it re-inflates the operative field |
| 7 | Return to two-lung ventilation for severe refractory hypoxemia |
| 8 | Surgical clamping of the pulmonary artery to the collapsed lung (last resort - eliminates shunt completely) |
Additional pharmacological options:
- Almitrine (IV pulmonary vasoconstrictor): potentiates HPV, reduces shunt - effective when combined with inhaled NO
- Inhaled NO: vasodilator to ventilated regions, increases Va/Q - alone has minimal effect but improves oxygenation when combined with almitrine
(Morgan & Mikhail 7e, p. 1047; Miller's 10e, p. 7191)
Choice of Anesthetic Agent
- At ≤1 MAC, modern volatile agents (isoflurane, sevoflurane, desflurane) are equipotent and weak HPV inhibitors - responsible for only ~4% net increase in shunt; acceptable for routine OLV
- TIVA (total IV anesthesia) may be preferred in special situations (e.g., bleomycin-treated patients requiring FiO2 limitation)
- Dexmedetomidine added to volatile anesthesia improves oxygenation during OLV
- Nitrous oxide should be avoided: raises pulmonary artery pressures, inhibits HPV, associated with increased postoperative atelectasis (51% vs. 24% with air/O2)
(Miller's Anesthesia 10e, p. 7200-7201)
Lung Injury During OLV
OLV can injure both lungs:
- Dependent (ventilated) lung: hyperperfusion + ventilator-induced trauma (volutrauma, barotrauma) from large tidal volumes
- Nondependent (collapsed) lung: surgical trauma + ischemia-reperfusion injury on re-expansion
Acute lung injury (ALI) after lung resection:
- Incidence: 2.5% overall; 7.9% after pneumonectomy
- Mortality/major morbidity: ~40% when it occurs
- Lung-protective ventilation (low VT, low FiO2, low pressures) reduces ALI risk
(Morgan & Mikhail 7e, p. 1046)
Lung Isolation in Special Situations
| Situation | Approach |
|---|---|
| Tracheostomy | Bronchial blocker through tracheostomy tube; specially sized DLT |
| Difficult airway | Bronchial blocker preferred; fiberoptic-assisted DLT placement |
| Bronchopleural fistula / large air leak | Lung isolation is absolute indication; OLV immediately separates affected side |
| Lung abscess / massive hemoptysis | Absolute isolation required to protect contralateral lung |
| Bilateral bullous disease | Avoid N2O; careful PEEP titration |
Postoperative Considerations
- Extubate early when possible to reduce barotrauma risk (especially risk of bronchial suture "blowout")
- When post-op ventilation is needed, replace the DLT with a standard single-lumen tube using a tube exchanger
- Common post-op complications: atelectasis, hypoxemia from splinting, reexpansion pulmonary edema of the collapsed lung, supraventricular arrhythmias (~common), hemorrhage (3% of thoracotomies)
- Adequate analgesia is essential - pain-related splinting leads to atelectasis and hypoxemia; thoracic epidural analgesia is the gold standard for open thoracotomy
(Morgan & Mikhail 7e, p. 1047-1048)
Recent evidence (2025): A meta-analysis (Wu et al., 2025) confirmed that double-lumen bronchial tubes and bronchial blockers have comparable efficacy and safety for OLV in thoracic surgery, supporting either device selection based on clinical context. A network meta-analysis (Li et al., 2025) further compared multiple OLV devices, finding nuanced differences in positioning ease and complication profiles.
Sources: Miller's Anesthesia 10e; Morgan & Mikhail's Clinical Anesthesiology 7e; Barash Clinical Anesthesia 9e
Oxygen dissociation curve for exam going DNB Anesthesiology trainee.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Excellent - I have comprehensive content from multiple authoritative textbooks and 3 key diagrams. Now let me compile the complete exam-focused answer for a DNB Anesthesiology trainee.
Oxygen-Hemoglobin Dissociation Curve (ODC)
DNB Anesthesiology Exam Notes
1. The Curve - Basic Description
The ODC describes the relationship between PaO2 (partial pressure of oxygen) and hemoglobin oxygen saturation (SpO2). It is measured at standard conditions: pH 7.40, temperature 37°C, PaCO2 40 mmHg.
Shape: Sigmoid (S-shaped) - NOT hyperbolic.
The sigmoid shape arises from cooperative binding (allosterism): binding of one O2 molecule to a heme group increases the oxygen affinity of the remaining three heme groups. This is due to conformational change in Hb from the T (tense, deoxy, low-affinity) state to the R (relaxed, oxy, high-affinity) state.
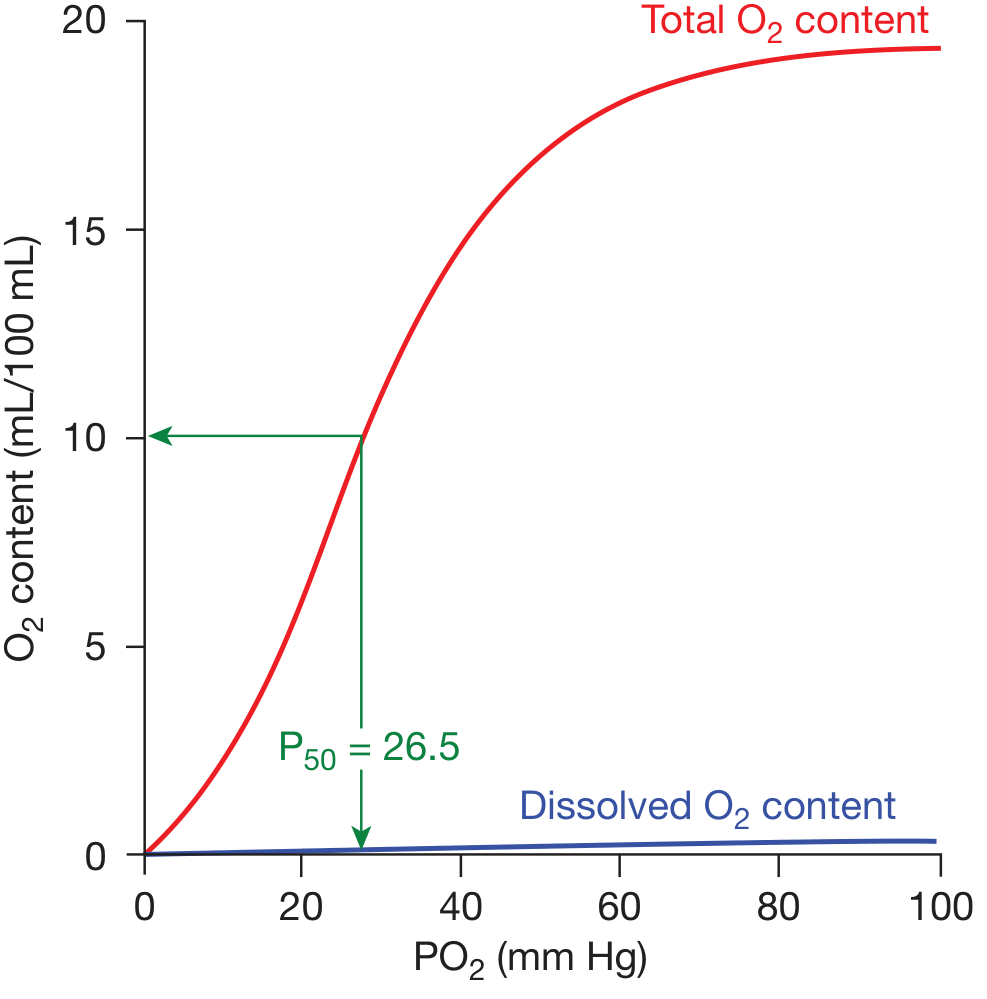
Oxygen dissociation curve showing total O2 content (red) and dissolved O2 (blue). P50 = 26.5 mmHg. - Fishman's Pulmonary Diseases & Disorders
2. Key Reference Points (Must Memorize for Exams)
| Point | PaO2 (mmHg) | SaO2 (%) | Clinical Significance |
|---|---|---|---|
| Arterial (a) | 95-100 | 97 | Normal arterial blood |
| Mixed venous (v̄) | 40 | 75 | At rest; 25% O2 extracted |
| P50 | 26.5 | 50 | Standard measure of Hb-O2 affinity |
| "Cliff edge" | 60 | ~90 | Below this: small PO2 drop → large SpO2 fall |
P50 is the PaO2 at which Hb is 50% saturated, measured at standard conditions. It is the single best number to express overall Hb-O2 affinity.
- Normal P50 = 26.5 mmHg
- Increased P50 = right shift = decreased affinity
- Decreased P50 = left shift = increased affinity
3. Why the Sigmoid Shape is Physiologically Perfect
The curve has two functional regions:
Upper Flat Portion (PaO2 60-100 mmHg) - "Loading Zone" (Lungs)
- Saturation stays high (~89-97%) despite large PaO2 swings
- Protective: even with lung disease causing PaO2 drop to 60 mmHg, Hb is still ~89% saturated
- O2 loading in the lungs is efficient and buffered
Steep Portion (PaO2 20-60 mmHg) - "Unloading Zone" (Tissues)
- Small drop in PO2 → large release of O2
- At rest PO2 falls from 95 → 40 mmHg in tissues, releasing ~25% of O2 (5 mL/100 mL blood)
- During exercise, active muscle can extract much more O2 with only modest PO2 reduction
- This is impossible with a hyperbolic curve (e.g., myoglobin has high affinity throughout this range and cannot unload O2 efficiently)
Exam pearl: Myoglobin has a hyperbolic curve and acts as an O2 store in muscle, not a transporter. It only releases O2 when intracellular PO2 falls very low.
Hb also acts as a tissue PO2 buffer - tissue PO2 is normally held between 15-40 mmHg regardless of whether alveolar PO2 varies from 60 to 500 mmHg. (Guyton & Hall)
4. Shifts of the ODC - The Most Exam-Tested Topic
RIGHT SHIFT = Increased P50 = Decreased Hb-O2 affinity = MORE O2 released to tissues
LEFT SHIFT = Decreased P50 = Increased Hb-O2 affinity = LESS O2 released to tissues
Causes of RIGHT SHIFT (CADET mnemonic):
| Factor | Mechanism |
|---|---|
| ↑ CO2 (hypercapnia) | Carbamino formation stabilizes T state |
| ↑ Acidity (↓ pH) | H+ binds Hb, stabilizes T state (Bohr effect) |
| ↑ DPG (2,3-bisphosphoglycerate) | Binds β-chain cleft, stabilizes T state |
| ↑ Exercise / Exercise metabolites | CO2, H+, temperature all rise together |
| ↑ Temperature | Disrupts Hb-O2 bonds |
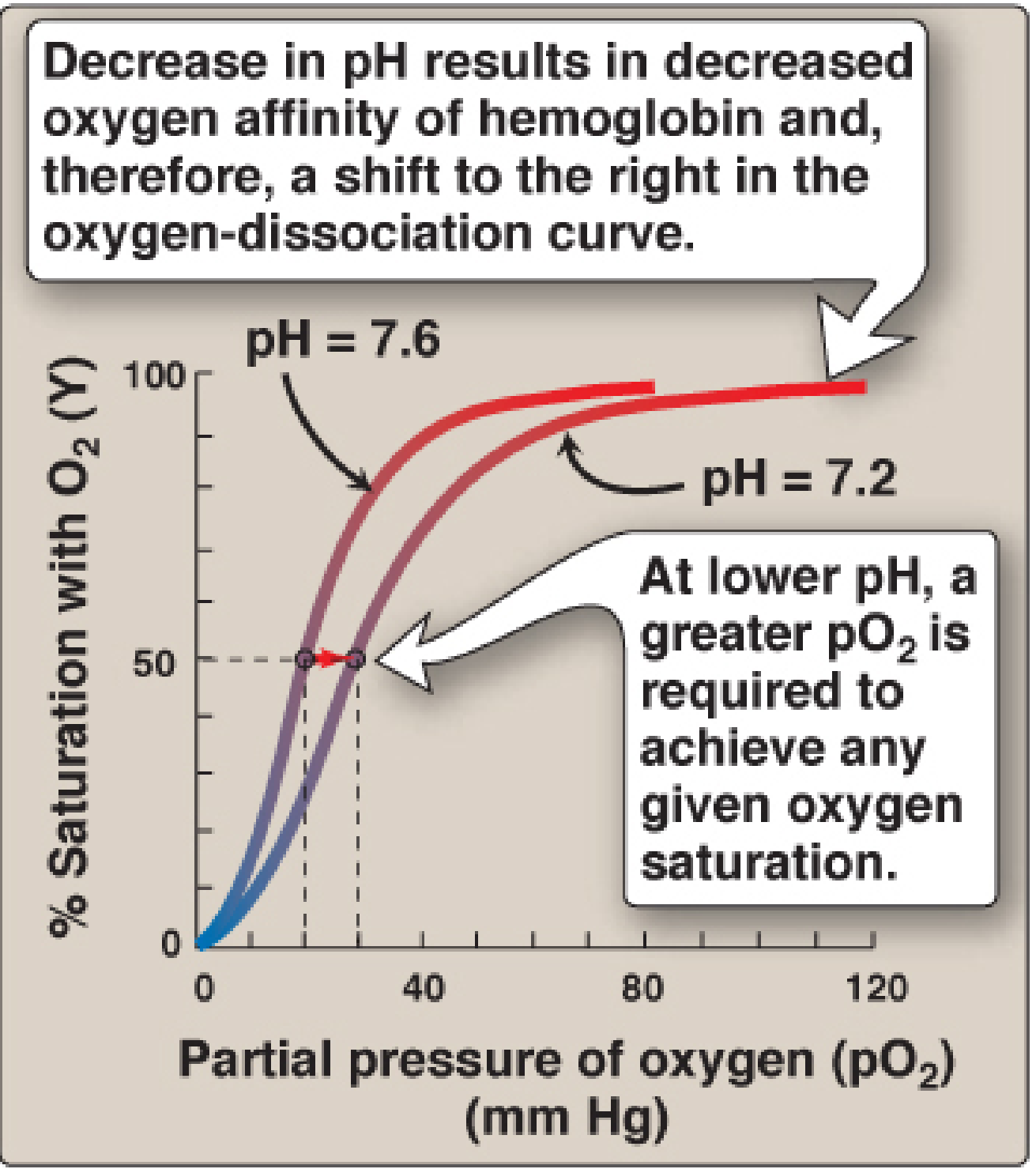
Bohr effect: pH 7.2 (acidosis) shifts curve right, requiring higher pO2 to achieve any given saturation. - Lippincott Biochemistry 8e
Causes of LEFT SHIFT (opposite of above):
| Factor | Examples |
|---|---|
| ↓ CO2 (hypocapnia) | Hyperventilation, alkalosis |
| ↓ Temperature | Hypothermia, stored blood |
| ↓ 2,3-DPG | Stored blood (DPG depletes in 24h), hexokinase deficiency |
| Fetal Hb (HbF) | γ chains bind 2,3-DPG less avidly than β chains |
| MetHb, COHb, HbS | Various mechanisms |
| Alkalosis |
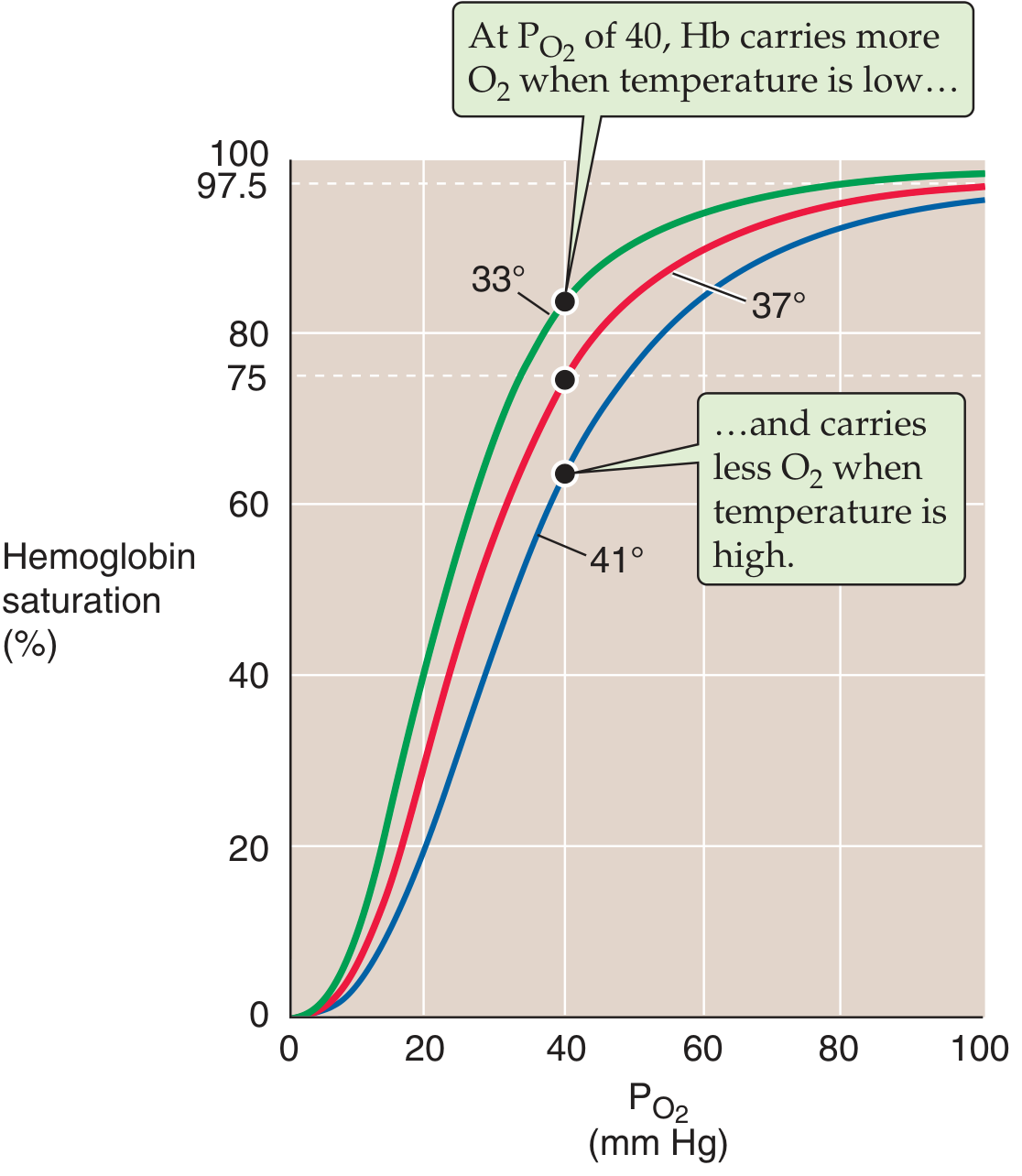
Temperature effect on ODC: 33°C (left shift) → more O2 held; 41°C (right shift) → more O2 released. - Medical Physiology (Boron & Boulpaep)
5. The Bohr Effect - Exam Favorite
Described by Christian Bohr (1904). Increased [H+] or increased PCO2 → right shift of ODC → promotes O2 unloading at tissues.
Mechanism at tissue level:
- Active tissues produce CO2
- Carbonic anhydrase: CO2 + H2O → H2CO3 → HCO3⁻ + H⁺
- H⁺ binds to specific histidine residues on Hb (β-chain His146)
- Salt bridges form → stabilizes T (deoxy) state
- Hb dumps O2
Mechanism at lung level (reverse):
- Low PCO2, high pH in alveolar capillaries → destabilizes T state → shifts Hb to R state → O2 loading enhanced
The CO2-specific Bohr effect also involves carbamino formation: CO2 + Hb-NH2 → Hb-NH-COO⁻ (carbamino-Hb), further stabilizing the deoxy T state.
6. 2,3-Bisphosphoglycerate (2,3-BPG / DPG)
- Produced in RBCs via Rapoport-Luebering shunt (glycolysis bypass)
- Binds to the central cavity formed by the β-chains of deoxy-Hb (T state); cannot bind in R (oxy) state
- Stabilizes T state → reduces O2 affinity → right shift
Why HbF has higher O2 affinity:
- HbF has γ-chains replacing β-chains
- γ-chains bind 2,3-DPG less avidly than β-chains
- Result: HbF stays more in R state → higher O2 affinity → LEFT-shifted ODC
- This allows fetal blood to extract O2 from maternal blood across the placenta (fetal PO2 is low, ~30-40 mmHg)
2,3-DPG in clinical practice:
| Condition | 2,3-DPG | ODC Shift | Effect |
|---|---|---|---|
| Stored blood (>24h) | ↓ | Left | Hb won't release O2 to tissues |
| Chronic hypoxia/anemia | ↑ | Right | Compensatory - delivers more O2 |
| Hyperthyroidism | ↑ | Right | |
| Hypothyroidism | ↓ | Left | |
| Pyruvate kinase deficiency | ↑ | Right | |
| Hexokinase deficiency | ↓ | Left |
7. Special Hemoglobins and ODC
| Hemoglobin | Shift | Clinical Notes |
|---|---|---|
| HbF (fetal, α2γ2) | LEFT (P50 ~18-20 mmHg) | Higher O2 affinity, placental O2 extraction |
| HbA2 (α2δ2) | Slightly left | Minor adult Hb (~2.5%) |
| COHb (carboxyhemoglobin) | LEFT | CO binds Hb 200-250x > O2; also converts remaining subunits to R state |
| MetHb | LEFT | Fe3+ cannot carry O2; remaining Fe2+ subunits have increased affinity; Bohr effect absent in α-chain MetHb |
| HbS (sickle) | Slightly RIGHT | Reduced O2 affinity; polymerizes when deoxygenated |
| High-affinity variants (e.g., Hb Chesapeake, Yakima) | LEFT | Erythrocytosis (erythropoietin-driven) |
| Low-affinity variants (e.g., Hb Kansas, Beth Israel) | RIGHT | Cyanosis + anemia; not distinguished on gel electrophoresis |
COHb - the "double insult":
- CO occupies heme sites (reducing O2-carrying capacity)
- Remaining oxy-Hb subunits shift LEFT (won't release O2 to tissues) Result: SpO2 reads falsely normal on pulse oximeter (COHb absorbs light like OxyHb at 660 nm)
8. Oxygen Content of Blood
Formula:
CaO2 = (Hb × 1.34 × SaO2) + (PaO2 × 0.003)
| Component | Value (normal) | Notes |
|---|---|---|
| Hb-bound O2 | ~19.7 mL/100 mL | Dominant component |
| Dissolved O2 | ~0.3 mL/100 mL | Linear with PaO2; 0.003 mL/mmHg/100 mL |
| Total CaO2 | ~20 mL/100 mL | |
| Mixed venous CvO2 | ~15 mL/100 mL | |
| O2 delivery (DO2) | = CaO2 × CO × 10 | Normal ~1000 mL/min |
| O2 consumption (VO2) | ~250 mL/min | At rest |
Hüfner's constant = 1.34 mL O2 per gram of Hb (theoretical max = 1.39, but ~1.34 in vivo due to MetHb and other forms)
9. Clinical Anesthesia Applications (High-Yield)
Hypothermia and ODC
- Hypothermia causes LEFT shift → Hb retains O2 → tissue hypoxia risk even if SpO2 appears normal
- Clinically relevant in cardiac bypass, deep hypothermic circulatory arrest
- At 20°C, P50 falls dramatically; blood gas analyzers measure PO2 at 37°C - must correct for patient temperature
Stored Blood
- 2,3-DPG depletes in 24-48h of storage → left shift
- However, regenerated within 24h after transfusion
- Clinical impact debated - large RCTs (INFORM trial) showed no survival difference with older vs. newer blood
One-Lung Ventilation (OLV) / Thoracic Anesthesia
- HPV depends partly on the ODC - hypoxia in the nonventilated lung promotes vasoconstriction (HPV)
- Alkalosis from hyperventilation → LEFT shift → impairs O2 delivery; also inhibits HPV
Carbon Monoxide Poisoning
- Standard pulse oximetry unreliable (falsely high SpO2 reading)
- Measure COHb directly by co-oximetry
- 100% O2 displaces CO; half-life of COHb falls from 5h (room air) → 90 min (100% O2) → 23 min (hyperbaric O2)
Neonates
- At birth HbF predominates (left-shifted curve); transitions to HbA over first 6 months
- Fetal "normal" PaO2 values are lower (25-35 mmHg) but Hb saturation still ~70% due to HbF
10. Quick Summary Table - Shifts of ODC
| Causes RIGHT Shift (↑ P50) | Causes LEFT Shift (↓ P50) |
|---|---|
| ↑ Temperature | ↓ Temperature (hypothermia) |
| ↑ PCO2 | ↓ PCO2 (hyperventilation) |
| ↓ pH (acidosis) | ↑ pH (alkalosis) |
| ↑ 2,3-DPG | ↓ 2,3-DPG (stored blood) |
| Exercise | HbF (fetal Hb) |
| Chronic anemia / hypoxia | COHb, MetHb |
| Hyperthyroidism | Hypothyroidism |
| Sickle Hb (HbS) | High-affinity Hb variants |
RIGHT shift = R for Release of O2 (good for tissues)
LEFT shift = L for Loading O2 (good for lungs; bad for tissue delivery)
DNB Exam Buzzwords to Remember
- P50 = 26.5 mmHg (normal)
- Bohr effect = H⁺/CO2 → right shift
- Haldane effect = O2 binding → CO2 release (reciprocal)
- HbF left-shifted because γ-chains bind 2,3-DPG less
- Sigmoid shape = cooperative binding (not hyperbolic like myoglobin)
- "Cliff edge" at PaO2 60 mmHg = SpO2 90%; below this, further desaturation is rapid
- Hüfner's constant = 1.34 mL O2/g Hb
- Pulse oximetry blind to COHb and MetHb - use co-oximetry
Sources: Fishman's Pulmonary Diseases 2e; Lippincott Biochemistry 8e; Guyton & Hall Medical Physiology; Medical Physiology (Boron & Boulpaep); Barash Clinical Anesthesia 9e; Miller's Anesthesia 10e
Small -1 page recent advances in OLV.
Searching PubMed
"one lung ventilation" AND "lung protective"
Searching PubMed
"one lung ventilation" AND "driving pressure"
Searching PubMed
"one lung ventilation" AND bronchial blocker
Searching PubMed
"one lung ventilation" AND "acute lung injury" AND thoracic
Reading Article
PMID: 38065200
Reading Article
PMID: 42245953
Reading Article
PMID: 39825438
Reading Article
PMID: 40876391
Reading Article
PMID: 40637441
I now have excellent, high-quality recent evidence. Here is the concise 1-page recent advances summary:
Recent Advances in One-Lung Ventilation
DNB Anesthesiology - Concise Update (2023-2026)
1. Individualised Open-Lung Approach (iOLA) - iPROVE-OLV Trial (Lancet Respir Med, 2024)
The most important recent landmark trial in OLV.
- Design: Multicentre RCT, 1308 patients, 25 hospitals across 5 countries
- Intervention: iOLA = recruitment manoeuvre (RM) to 40 cmH2O end-inspiratory pressure + PEEP titrated to best respiratory compliance + postoperative high-flow nasal oxygen (HFNO)
- Control: Fixed PEEP 4 cmH2O + conventional O2 therapy
- Result: Severe postoperative pulmonary complications (PPCs) at 7 days:
- iOLA group: 6% vs control: 15% (RR 0.39; 95% CI 0.28-0.56)
- Absolute risk reduction: 9.2%
- Key message: Individualising PEEP to best compliance (rather than a fixed value) and adding postoperative HFNO significantly reduces PPCs after lung resection.
2. Individualised PEEP Titration by Compliance - Meta-Analysis (Crit Care, 2025)
- Design: Meta-analysis of 10 RCTs, 3426 patients
- Finding: Individualised PEEP by lung compliance vs. fixed PEEP:
- PPCs: RR 0.55 (95% CI 0.38-0.78) - 45% relative reduction
- Pneumonia: RR 0.71; Atelectasis: RR 0.63
- Better PaO2/FiO2 and lower driving pressure
- No difference in ARDS, mortality, or haemodynamics
- Best method: Titration by dynamic compliance using a stepwise decremental strategy outperformed incremental or driving-pressure based titration
- Key message: PEEP should be titrated to optimal compliance for each patient during OLV - a fixed 5 cmH2O is insufficient.
3. Driving Pressure (DP) as the New Ventilatory Target
What is Driving Pressure?
DP = Plateau Pressure - PEEP (reflects stress per unit of ventilatable lung)
- Emerged from ARDS literature (Amato, NEJM 2015) - applied now to OLV
- During OLV, only one lung is ventilated - DP captures the actual strain on available lung units better than tidal volume alone
2026 Systematic Review (Front Med, 2026 - PMID 42245953)
- Pooled 4 RCTs (654 patients): DP-guided ventilation trended toward reduced PPCs (RR 0.60) but not statistically significant (p = 0.14); evidence graded as low certainty (GRADE)
- Conclusion: DP-guided OLV is hypothesis-generating - larger multicentre trials needed
Large Observational Study (J Clin Anesth, 2025 - PMID 40876391)
- Retrospective cohort, ~4951 patients with OLV surgery
- DP independently associated with PPCs (OR 1.04 per cmH2O increase)
- Proposed thresholds: DP (plateau-based) ≤15 cmH2O; DP (peak-based) ≤18 cmH2O
- Mechanical power was NOT independently associated with PPCs in this cohort
4. Volatile vs. TIVA - Anti-inflammatory Advantage of Volatiles
Systematic Review + Meta-Analysis (Crit Care Explor, 2025 - PMID 40637441)
- 28 studies, 4175 patients undergoing lung resection
- Inhaled anaesthesia (vs TIVA) → lower alveolar TNF-α and IL-6 at 1-2 hours post-resection
- Suggests volatile agents (sevoflurane, desflurane) reduce the inflammatory cascade triggered by OLV ischaemia-reperfusion injury
- Limitation: Clinical outcome differences (mortality, ICU stay) not consistently reported
- Practical implication: Volatile anaesthesia may be preferred over TIVA specifically to attenuate OLV-associated lung inflammation, particularly in pneumonectomy or high-risk cases
5. Bronchial Blockers (BB) vs. Double-Lumen Tubes (DLT) - Updated Evidence
Meta-Analysis (BMC Anesthesiol, 2025 - PMID 40450255)
- DLT and BB have comparable efficacy and safety for OLV
- BB advantages: preferred in tracheostomy, difficult airway, patients requiring postoperative ventilation
- DLT advantages: faster lung collapse, easier suctioning, better CPAP delivery to operative lung
New Placement Technique (J Clin Anesth, 2025 - PMID 40367865)
- Multicentre RCT: Placing the BB in the lateral decubitus position (rather than supine before positioning) improved first-attempt success rate and reduced displacement
- 2026 RCT (BMC Anesthesiol): Right lateral decubitus position improved left BB placement success
Video-DLT / Video-Imaging Bronchial Blockers
- Emerging: video-imaging DLTs and video-guided blockers allow real-time visualisation of cuff position without fibreoptic bronchoscope
- 2025 RCT showed comparable outcomes between video-DLT and video-blocker + single-lumen tube for left lung isolation in minimally invasive cardiac surgery
6. Permissive Hypercarbia During OLV (EJA RCT, 2023 - PMID 37455644)
- Prospective RCT, thoracic surgery patients
- Permissive hypercapnia (allowing PaCO2 rise) during OLV:
- Improved PaO2 during OLV (vasoconstricts pulmonary vessels → potentiates HPV)
- Reduced postoperative pulmonary complications
- Mechanism: Hypercapnia enhances HPV in the collapsed lung, reducing shunt
- Corroborates allowing moderate CO2 rise rather than aggressive ventilation to normalise PaCO2
7. Cerebral Oximetry Monitoring During OLV (J Int Med Res, 2024 - PMID 39275973)
- RCT in elderly patients undergoing OLV thoracoscopic surgery
- Optimising cerebral O2 saturation (rSO2) by targeted interventions during OLV reduced postoperative delirium incidence
- Adds neurocognitive monitoring as a new dimension of OLV management in the elderly
Summary: What Has Changed in OLV Practice
| Old Approach | Current Evidence-Based Approach |
|---|---|
| Fixed PEEP 5 cmH2O | Individualised PEEP titrated to best compliance (decremental method) |
| Tidal volume <6 mL/kg | Tidal volume <6 mL/kg + driving pressure ≤15 cmH2O |
| Recruitment as salvage | Recruitment manoeuvre routinely before PEEP titration (iPROVE-OLV) |
| 100% FiO2 routinely | Lowest effective FiO2; postoperative HFNO reduces PPCs |
| TIVA vs volatile - equivalent | Volatile preferred for anti-inflammatory lung protection |
| DLT always first choice | BB equally safe; BB preferred in difficult airway/tracheostomy |
| Normalise PaCO2 | Permissive hypercarbia acceptable and may improve oxygenation |
Key references: iPROVE-OLV (Lancet Respir Med 2024, PMID 38065200); individualised PEEP meta-analysis (Crit Care 2025, PMID 39825438); driving pressure systematic review (Front Med 2026, PMID 42245953); volatile vs TIVA meta-analysis (Crit Care Explor 2025, PMID 40637441)
This is a shared conversation. Sign in to Orris to start your own chat.