History taking in ent
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Here is a structured, comprehensive guide to ENT history taking, drawn from K.J. Lee's Essential Otolaryngology and Cummings Otolaryngology Head and Neck Surgery.
History Taking in ENT
ENT history taking follows the same general framework as any clinical history but must systematically cover each of the four main subsystems: the ear, nose and sinuses, throat/larynx, and head and neck. The questions asked under each system help narrow the differential diagnosis before physical examination.
1. General Framework
Begin with the standard structure:
| Component | Content |
|---|---|
| Presenting complaint (PC) | Chief symptom in the patient's own words |
| History of presenting complaint (HPC) | SOCRATES for each symptom |
| Past medical/surgical history | Especially prior ENT operations (tonsillectomy, myringotomy, septoplasty, etc.) |
| Drug history | Ototoxic drugs (aminoglycosides, loop diuretics, cisplatin), antihypertensives, decongestants, anticoagulants |
| Allergies | Drug allergies + atopic history (rhinitis, asthma, eczema) |
| Family history | Hearing loss, neurofibromatosis type 2, autoimmune disorders, head and neck neoplasms |
| Social history | Smoking, alcohol, occupation (noise exposure, chemical exposure), travel history, sexual history |
| Systems review | Weight loss, fatigue, fever, neurological symptoms |
For symptoms, use the SOCRATES mnemonic:
- Site, Onset, Character, Radiation, Associations, Timing/course, Exacerbating/relieving factors, Severity
2. Ear (Otological History)
Common presenting symptoms
A. Hearing Loss (Hypoacusis)
- Onset: sudden vs. gradual
- Unilateral or bilateral
- Fluctuating or progressive
- Associated tinnitus, vertigo, aural fullness
- History of noise exposure, ototoxic medications, head trauma, ear infections or surgery
- Family history of deafness
B. Otalgia (Ear Pain)
- Site: inside the ear or periauricular
- Primary vs. referred otalgia (common referral sources: dental disease, TMJ, tonsils, larynx, cervical spine - via CN V, IX, X, and C2-C3)
- Associated discharge, hearing loss, fever
C. Otorrhoea (Ear Discharge)
- Character: watery, mucoid, mucopurulent, bloody, cheesy/foul (suggests cholesteatoma)
- Duration and frequency
- Relation to upper respiratory infection
- Painless chronic discharge - consider chronic suppurative otitis media
D. Tinnitus
- Subjective (most common) or objective (pulsatile - vascular cause)
- Unilateral or bilateral
- Pitch and character (ringing, buzzing, roaring)
- Associated hearing loss or vertigo
- Effect on sleep and quality of life
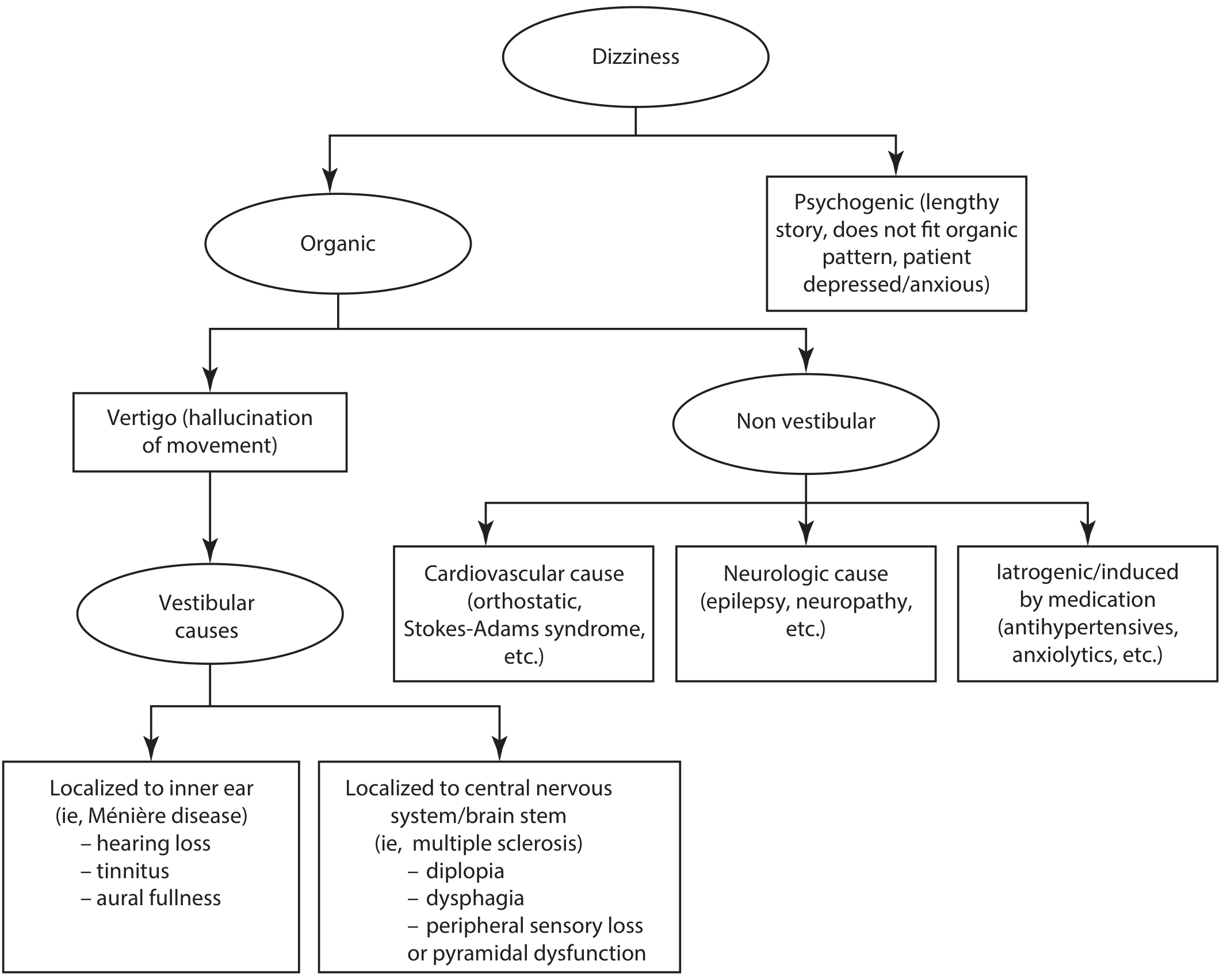
E. Vertigo and Dizziness
This is particularly important. A minimum vertigo history should address (K.J. Lee):
| Question | Significance |
|---|---|
| Duration of each attack (seconds/minutes/hours/days) | BPPV = seconds; Meniere's = 20 min - 12 hrs; vestibular neuritis = days |
| Frequency (daily/weekly/monthly) | Pattern recognition |
| Effect of head movements | Positional = BPPV |
| Inducing position/posture | Rolling to one side points to specific semicircular canal |
| Associated hearing loss, tinnitus, aural pressure | Points to inner ear (Meniere's disease) |
| Prior ear disease or ear surgery | Labyrinthine fistula, cholesteatoma |
| Family history, diabetes, neurofibromatosis | Genetic/systemic cause |
| Head trauma, medications, comorbidities | Ototoxicity, post-traumatic |
3. Nose and Sinuses (Rhinological History)
Common presenting symptoms
A. Nasal Obstruction
- Unilateral or bilateral; constant or intermittent
- Worse at certain times (day/night, season) - suggests allergy or structural cause
- Associated mouth breathing, snoring, sleep apnoea
B. Rhinorrhoea (Nasal Discharge)
- Character: clear/watery (allergy, CSF leak), mucoid, mucopurulent, bloody
- Unilateral bloodstained discharge in an adult - consider malignancy
C. Epistaxis (Nosebleed)
- Site: anterior (Little's area, most common) vs. posterior
- Frequency, duration, volume
- Precipitating factors (trauma, nose-picking, anticoagulants, hypertension)
- Family history (hereditary haemorrhagic telangiectasia)
D. Anosmia / Hyposmia (Smell Disturbance)
- Sudden onset (post-URI, post-traumatic) vs. gradual/fluctuating (sinusitis, allergic rhinitis, neurodegenerative disease)
- Congenital anosmia (Kallmann syndrome)
- Clarify the taste-smell distinction: flavor complaints are largely smell-dependent, while basic taste perception (sweet, sour, salty, bitter, umami) is separate
E. Facial Pain / Pressure
- Location: forehead (frontal), cheeks (maxillary), between eyes (ethmoidal), top of head (sphenoidal)
- Relation to posture (worse bending forward - sinusitis)
- Associated with nasal discharge or blockage
F. Sneezing, Itching, Postnasal Drip
- Suggests allergic rhinitis; ask about allergen exposure (dust, pollen, animals, occupational allergens)
4. Throat and Larynx (Laryngopharyngeal History)
Common presenting symptoms
A. Dysphagia (Difficulty Swallowing)
- Level: oral, pharyngeal (nasal regurgitation, coughing on swallowing), oesophageal
- Solids only (mechanical obstruction - stricture, carcinoma) vs. solids and liquids (motility disorder)
- Progressive (sinister - carcinoma) or intermittent (web, dysmotility)
- Associated odynophagia (painful swallowing), weight loss, hoarseness, regurgitation
B. Dysphonia / Hoarseness
- Duration: >3 weeks is a red flag requiring laryngoscopy to exclude malignancy
- Character: breathy (vocal cord palsy), rough/harsh (nodules, laryngitis), strained (spasmodic dysphonia)
- Associated with voice use (singers, teachers - vocal abuse), reflux, smoking
C. Sore Throat
- Acute vs. chronic
- Associated fever, trismus (peritonsillar abscess), difficulty breathing (epiglottitis - emergency)
- Recurrent tonsillitis: number of episodes per year, school/work days lost
D. Stridor
- Inspiratory (supraglottic/glottic), expiratory (subglottic/tracheal), or biphasic
- Onset: acute (foreign body, epiglottitis, angioedema) or chronic (subglottic stenosis, papillomatosis)
- This is always a potential airway emergency
E. Neck Lump
- Location, onset, duration, growth rate
- Associated symptoms: dysphagia, voice change, pain, constitutional symptoms (fever, night sweats, weight loss - lymphoma)
- Skin changes, fixation to underlying structures
- Exposure history: TB contact, cat scratch, EBV
5. Sleep-Related History (OSA)
In any patient with snoring or suspected obstructive sleep apnoea (OSA), the history should cover (K.J. Lee):
- Sleep habits, hygiene, typical sleep/wake times, shift work
- Daytime sleepiness (Epworth Sleepiness Scale - score >10 is significant)
- Observed apnoeic episodes (history from bed partner is invaluable)
- Morning headaches, nocturia, poor concentration
- Comorbidities: hypertension, obesity, metabolic syndrome, cardiovascular disease
- Occupational risk: drivers or heavy machinery operators have legal reporting implications in some jurisdictions
6. Head and Neck / Salivary Gland History
When a salivary gland is involved (K.J. Lee), specifically ask:
- Which gland(s) are affected: onset, duration, progression
- Pain: character, intensity, duration
- Cranial nerve deficit (facial nerve - parotid; trigeminal)
- Salivary discharge, dry mouth/eyes (Sjogren's)
- Otalgia (referred from parotid)
- Fever, weight loss, neck swelling
- Social history: smoking, alcohol, travel, infections, sexual history
- Family history: autoimmune disorders, head and neck neoplasms, lymphoma, genetic syndromes
7. Red Flag Symptoms in ENT
Always actively screen for these - they require urgent investigation:
| Red Flag | Possible Cause |
|---|---|
| Hoarseness > 3 weeks | Laryngeal carcinoma |
| Unilateral bloodstained nasal discharge | Nasal/sinus malignancy |
| Unilateral serous otitis media in adult | Nasopharyngeal carcinoma |
| Progressive unilateral sensorineural hearing loss | Acoustic neuroma (vestibular schwannoma) |
| Trismus + peritonsillar swelling | Peritonsillar abscess |
| Stridor | Airway compromise |
| Neck lump + constitutional symptoms | Lymphoma, metastatic carcinoma |
| Progressive dysphagia + weight loss | Hypopharyngeal/oesophageal carcinoma |
| Facial nerve palsy + parotid lump | Parotid malignancy |
A thorough ENT history, structured this way, will guide targeted examination and appropriate investigation before reaching a diagnosis. - K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology Head and Neck Surgery
1
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I'll assume you meant Section 1 - the General Framework and want it expanded in detail. Here it is:
Section 1: General Framework of ENT History Taking - Expanded
Every ENT history, regardless of the presenting complaint, follows a structured sequence. Think of it as building a clinical story layer by layer.
Step 1 - Introduce and Establish Rapport
- Greet the patient, confirm their name and age
- Open with an open-ended question: "What has brought you in today?" or "Tell me what's been bothering you."
- Let the patient speak for 1-2 minutes without interruption - studies show most patients finish their opening statement in under 90 seconds if allowed to continue
Step 2 - Presenting Complaint (PC)
Record the complaint in the patient's own words, not medical terminology. One or two words is ideal (e.g., "blocked ear," "lump in neck," "can't hear").
Step 3 - History of Presenting Complaint (HPC)
Use SOCRATES for every symptom:
| Letter | Stands for | Example questions in ENT |
|---|---|---|
| S | Site | "Which ear?" / "Which side of the nose?" |
| O | Onset | "When did it start? Was it sudden or gradual?" |
| C | Character | "Is the pain sharp, dull, throbbing? Is the discharge watery or thick?" |
| R | Radiation | "Does the pain spread anywhere - jaw, neck?" |
| A | Associations | "Any hearing loss with the pain? Any fever?" |
| T | Timing | "Is it constant or does it come and go? Any pattern?" |
| E | Exacerbating/Relieving | "What makes it worse or better?" |
| S | Severity | "On a scale of 1-10, how bad is it? How is it affecting your daily life?" |
For hearing loss specifically, Cummings recommends also asking about:
- Onset: abrupt vs. gradual; progressive, intermittent, or continuous
- Associated symptoms: tinnitus, vertigo, aural fullness, pain, allergy symptoms, distorted auditory perception
- Whether symptoms worsen with pregnancy or oral contraceptive use (relevant for otosclerosis)
Step 4 - Past Medical History (PMH)
Ask about:
- General medical conditions: diabetes (wax buildup, malignant otitis externa), hypertension (epistaxis, pulsatile tinnitus), autoimmune disease (sudden SNHL, Wegener's, Sjogren's), hypothyroidism (hoarseness, goitre)
- Previous ENT conditions: recurrent tonsillitis, otitis media, sinusitis, nasal polyps, previous hearing loss
- Previous ENT surgery: myringotomy and grommets, tonsillectomy, adenoidectomy, septoplasty, FESS, mastoidectomy - ask about outcome and any complications
- Other surgical history that may be relevant (e.g., neck dissection, thyroid surgery affecting the recurrent laryngeal nerve causing hoarseness)
- Significant infections: meningitis (causes SNHL), syphilis (causes SNHL and vestibular problems), mumps (unilateral SNHL)
Step 5 - Drug History
This is particularly important in ENT. Always ask about:
| Drug Category | ENT Relevance |
|---|---|
| Aminoglycoside antibiotics (gentamicin, streptomycin, neomycin) | Ototoxicity - cochlear and vestibular damage |
| Loop diuretics (furosemide) | Ototoxicity, especially combined with aminoglycosides |
| Cytotoxic drugs (cisplatin, carboplatin) | Ototoxicity |
| Quinine / antimalarials | Tinnitus, hearing loss |
| Aspirin and NSAIDs (high dose) | Reversible tinnitus |
| Antihypertensives / beta-blockers | Nasal stuffiness; relevant in OSA workup |
| Anticoagulants (warfarin, DOACs) | Epistaxis |
| Nasal decongestants (oxymetazoline) | Rhinitis medicamentosa with prolonged use |
| ACE inhibitors | Chronic cough (can be mistaken for throat/laryngeal problem) |
| Bisphosphonates | Osteonecrosis of the jaw - relevant in head and neck surgery |
Ask specifically about over-the-counter drugs and supplements - patients often omit these.
Step 6 - Allergy History
- Drug allergies: ask about the specific reaction (true anaphylaxis vs. intolerance)
- Atopic triad: allergic rhinitis, asthma, eczema - often co-exist; critical for rhinology workup
- Seasonal vs. perennial pattern (perennial suggests house dust mite or pet allergy; seasonal suggests pollen)
- Food allergies (relevant in eosinophilic oesophagitis causing dysphagia; oral allergy syndrome)
- Latex allergy (relevant pre-operatively)
Step 7 - Family History (FH)
| Condition | Reason to ask |
|---|---|
| Hearing loss | Genetic SNHL (connexin 26/GJB2 mutation, Pendred syndrome, Usher syndrome) |
| Neurofibromatosis type 2 | Bilateral acoustic neuromas - autosomal dominant |
| Otosclerosis | Autosomal dominant with variable penetrance |
| Hereditary haemorrhagic telangiectasia (Osler-Weber-Rendu) | Recurrent severe epistaxis |
| Head and neck malignancy | Increased risk |
| Autoimmune disorders | Sjogren's, SLE, rheumatoid arthritis - can affect ENT |
| Allergic disease | Atopy runs in families |
| Cleft palate / craniofacial abnormalities | Associated middle ear disease |
Step 8 - Social History (SH)
| Factor | ENT Relevance |
|---|---|
| Smoking | Laryngeal/pharyngeal/oral cancer, chronic rhinitis, worsens OSA |
| Alcohol | Head and neck cancer risk (synergistic with smoking), parotid enlargement |
| Occupation | Noise-induced hearing loss (factory workers, musicians, military); voice overuse (teachers, singers, call centre workers); chemical exposures (woodworkers - adenocarcinoma of ethmoid); farming (fungal sinusitis) |
| Recreational activities | Loud music/concerts (noise-induced hearing loss); swimming (otitis externa, otitis media); diving (barotrauma - perilymph fistula) |
| Air travel | Ear barotrauma, sinus pain |
| International travel | Tuberculosis (scrofula - cervical lymphadenopathy), rhinoscleroma, leishmaniasis |
| Sexual history | HPV (oropharyngeal cancer - base of tongue, tonsil); syphilis; HIV |
| Pets | Allergen exposure (cat dander, dog hair) |
| Marital/living situation | Bed partner history in OSA; passive smoking in children with recurrent otitis media |
Step 9 - Systems Review
Always screen actively for:
- Constitutional: fever, night sweats, unintentional weight loss (lymphoma, malignancy)
- Neurological: diplopia, facial weakness/numbness, dysphagia, hoarseness (cranial nerve involvement)
- Respiratory: cough, wheeze, breathlessness (asthma linked to nasal polyps; laryngeal cause of cough)
- Gastrointestinal: heartburn, regurgitation (laryngopharyngeal reflux causing hoarseness, globus, chronic cough)
- Rheumatological: joint pains, dry eyes/mouth (Sjogren's affecting salivary glands)
This framework ensures nothing clinically important is missed before you move on to the focused ENT-specific examination. - Cummings Otolaryngology Head and Neck Surgery; K.J. Lee's Essential Otolaryngology
Printable fornat
Reading File
Running Command
ls -la /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace && ls -la /home/daytona/workspace/
Running Command
mkdir -p /home/daytona/workspace/ent-history && echo "done"
Writing File
~/ent-history/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
OUTPUT = "/home/daytona/workspace/ent-history/ENT_History_Taking.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=2*cm,
rightMargin=2*cm,
topMargin=2*cm,
bottomMargin=2*cm,
title="ENT History Taking",
author="Orris Medical"
)
styles = getSampleStyleSheet()
# Custom styles
TEAL = colors.HexColor("#006B6B")
LIGHT_TEAL = colors.HexColor("#E6F4F4")
DARK = colors.HexColor("#1A1A2E")
ACCENT = colors.HexColor("#D97706")
LIGHT_GREY = colors.HexColor("#F5F5F5")
MID_GREY = colors.HexColor("#CCCCCC")
title_style = ParagraphStyle(
"Title", parent=styles["Title"],
fontSize=20, textColor=TEAL,
spaceAfter=4, alignment=TA_CENTER,
fontName="Helvetica-Bold"
)
subtitle_style = ParagraphStyle(
"Subtitle", parent=styles["Normal"],
fontSize=10, textColor=colors.grey,
spaceAfter=12, alignment=TA_CENTER,
fontName="Helvetica-Oblique"
)
section_style = ParagraphStyle(
"Section", parent=styles["Heading1"],
fontSize=12, textColor=colors.white,
spaceBefore=10, spaceAfter=4,
fontName="Helvetica-Bold",
backColor=TEAL,
leftIndent=-6, rightIndent=-6,
borderPad=4
)
subsection_style = ParagraphStyle(
"Subsection", parent=styles["Heading2"],
fontSize=10, textColor=TEAL,
spaceBefore=6, spaceAfter=2,
fontName="Helvetica-Bold"
)
body_style = ParagraphStyle(
"Body", parent=styles["Normal"],
fontSize=9, leading=13,
textColor=DARK,
fontName="Helvetica"
)
bullet_style = ParagraphStyle(
"Bullet", parent=styles["Normal"],
fontSize=9, leading=12,
leftIndent=14, firstLineIndent=-10,
textColor=DARK,
fontName="Helvetica",
bulletIndent=4
)
bullet2_style = ParagraphStyle(
"Bullet2", parent=styles["Normal"],
fontSize=8.5, leading=11,
leftIndent=26, firstLineIndent=-10,
textColor=DARK,
fontName="Helvetica"
)
redflag_style = ParagraphStyle(
"RedFlag", parent=styles["Normal"],
fontSize=9, leading=12,
textColor=colors.HexColor("#7B0000"),
fontName="Helvetica-Bold"
)
note_style = ParagraphStyle(
"Note", parent=styles["Normal"],
fontSize=8, leading=11,
textColor=colors.grey,
fontName="Helvetica-Oblique",
alignment=TA_CENTER
)
def section_header(text):
return [
Spacer(1, 6),
Paragraph(f" {text}", section_style),
Spacer(1, 4),
]
def subsection(text):
return Paragraph(text, subsection_style)
def body(text):
return Paragraph(text, body_style)
def bullet(text, level=1):
style = bullet_style if level == 1 else bullet2_style
return Paragraph(f"\u2022 {text}", style)
def spacer(h=4):
return Spacer(1, h)
# Table helper
def make_table(data, col_widths, row_colors=None):
t = Table(data, colWidths=col_widths, repeatRows=1)
style_cmds = [
("BACKGROUND", (0, 0), (-1, 0), TEAL),
("TEXTCOLOR", (0, 0), (-1, 0), colors.white),
("FONTNAME", (0, 0), (-1, 0), "Helvetica-Bold"),
("FONTSIZE", (0, 0), (-1, 0), 8.5),
("FONTNAME", (0, 1), (-1, -1), "Helvetica"),
("FONTSIZE", (0, 1), (-1, -1), 8.5),
("ROWBACKGROUNDS", (0, 1), (-1, -1), [colors.white, LIGHT_GREY]),
("GRID", (0, 0), (-1, -1), 0.4, MID_GREY),
("VALIGN", (0, 0), (-1, -1), "TOP"),
("LEFTPADDING", (0, 0), (-1, -1), 5),
("RIGHTPADDING", (0, 0), (-1, -1), 5),
("TOPPADDING", (0, 0), (-1, -1), 4),
("BOTTOMPADDING", (0, 0), (-1, -1), 4),
("WORDWRAP", (0, 0), (-1, -1), True),
]
t.setStyle(TableStyle(style_cmds))
return t
# ─── Build story ────────────────────────────────────────────────────────────────
story = []
# Title block
story.append(Spacer(1, 8))
story.append(Paragraph("ENT History Taking", title_style))
story.append(Paragraph("Ear • Nose & Sinuses • Throat & Larynx • Head & Neck", subtitle_style))
story.append(HRFlowable(width="100%", thickness=2, color=TEAL, spaceAfter=6))
# ── SECTION 1: GENERAL FRAMEWORK ────────────────────────────────────────────────
story += section_header("1. GENERAL FRAMEWORK")
story.append(subsection("Opening the Consultation"))
for b in [
"Greet the patient; confirm name and age",
"Open with an open-ended question: \"What has brought you in today?\"",
"Allow the patient to speak uninterrupted for the first 1–2 minutes",
"Record the <b>Presenting Complaint (PC)</b> in the patient's own words",
]:
story.append(bullet(b))
story.append(spacer())
story.append(subsection("SOCRATES — History of Presenting Complaint (HPC)"))
socrates_data = [
["Letter", "Stands for", "Example in ENT"],
["S", "Site", "Which ear? Which side of the nose?"],
["O", "Onset", "When did it start? Sudden or gradual?"],
["C", "Character", "Sharp/dull pain? Watery/thick discharge?"],
["R", "Radiation", "Does pain spread to jaw or neck?"],
["A", "Associations", "Any hearing loss with the pain? Fever?"],
["T", "Timing", "Constant or comes and goes? Any pattern?"],
["E", "Exacerbating/Relieving", "What makes it worse or better?"],
["S", "Severity", "1–10 scale. Effect on daily life?"],
]
story.append(make_table(socrates_data, [0.6*cm, 3*cm, 4*cm, 9.3*cm]))
story.append(spacer())
# ── SECTION 2: EAR ──────────────────────────────────────────────────────────────
story += section_header("2. EAR (Otological History)")
story.append(subsection("A. Hearing Loss"))
for b in [
"Onset: sudden vs. gradual; progressive, intermittent, or continuous",
"Unilateral or bilateral",
"Fluctuating (Ménière's) or steadily worsening",
"Associated tinnitus, vertigo, aural fullness",
"History of noise exposure, ototoxic medications, head trauma, ear infections or surgery",
"Worsening with pregnancy or oral contraceptive use (otosclerosis)",
"Family history of deafness (connexin 26/GJB2, Usher syndrome, Pendred syndrome)",
]:
story.append(bullet(b))
story.append(spacer(4))
story.append(subsection("B. Otalgia (Ear Pain)"))
for b in [
"Primary otalgia: pain originates in the ear",
"Referred otalgia — common sources via cranial nerves:",
]:
story.append(bullet(b))
referred = [
["CN V (trigeminal)", "Dental disease, TMJ dysfunction"],
["CN IX (glossopharyngeal)", "Tonsil, oropharynx, base of tongue"],
["CN X (vagus)", "Larynx, hypopharynx, oesophagus"],
["C2–C3 cervical", "Cervical spine, posterior fossa"],
]
ref_table = Table(referred, colWidths=[5.5*cm, 11.5*cm])
ref_table.setStyle(TableStyle([
("FONTNAME", (0, 0), (-1, -1), "Helvetica"),
("FONTSIZE", (0, 0), (-1, -1), 8.5),
("ROWBACKGROUNDS", (0, 0), (-1, -1), [colors.white, LIGHT_GREY]),
("GRID", (0, 0), (-1, -1), 0.4, MID_GREY),
("LEFTPADDING", (0, 0), (-1, -1), 5),
("TOPPADDING", (0, 0), (-1, -1), 3),
("BOTTOMPADDING", (0, 0), (-1, -1), 3),
]))
story.append(ref_table)
story.append(spacer(4))
story.append(subsection("C. Otorrhoea (Ear Discharge)"))
for b in [
"Character: watery / mucoid / mucopurulent / bloody / foul cheesy (→ cholesteatoma)",
"Duration and frequency; relation to upper respiratory infection",
"Painless chronic discharge → consider chronic suppurative otitis media (CSOM)",
]:
story.append(bullet(b))
story.append(spacer(4))
story.append(subsection("D. Tinnitus"))
for b in [
"Subjective (most common) or objective/pulsatile (→ vascular cause)",
"Unilateral or bilateral; pitch and character (ringing, buzzing, roaring)",
"Associated hearing loss or vertigo",
"Effect on sleep and quality of life",
]:
story.append(bullet(b))
story.append(spacer(4))
story.append(subsection("E. Vertigo / Dizziness — Minimum History (K.J. Lee)"))
vertigo_data = [
["Question", "Significance"],
["Duration of each attack", "Seconds = BPPV; 20 min–12 h = Ménière's; Days = vestibular neuritis"],
["Frequency", "Daily / weekly / monthly — pattern recognition"],
["Effect of head movements", "Positional → BPPV"],
["Inducing position/posture", "Rolling onto one side → specific canal involved"],
["Associated hearing loss, tinnitus, aural fullness", "→ Inner ear (Ménière's disease)"],
["Prior ear disease or surgery", "Labyrinthine fistula, cholesteatoma"],
["Family history, diabetes, neurofibromatosis", "Genetic / systemic cause"],
["Head trauma, medications, comorbidities", "Ototoxicity, post-traumatic"],
]
story.append(make_table(vertigo_data, [5.5*cm, 11.5*cm]))
story.append(spacer())
# ── SECTION 3: NOSE ─────────────────────────────────────────────────────────────
story += section_header("3. NOSE & SINUSES (Rhinological History)")
nose_items = {
"A. Nasal Obstruction": [
"Unilateral or bilateral; constant or intermittent",
"Worse at certain times (day/night, seasonal) → allergy vs. structural",
"Associated mouth breathing, snoring, sleep apnoea symptoms",
],
"B. Rhinorrhoea (Discharge)": [
"Clear/watery → allergy, CSF leak (unilateral, salty taste, halo sign)",
"Mucoid → sinusitis; mucopurulent → bacterial infection",
"Unilateral bloodstained discharge in adult → exclude malignancy (red flag)",
],
"C. Epistaxis": [
"Site: anterior (Little's area, most common) vs. posterior",
"Frequency, duration, estimated volume",
"Precipitating factors: trauma, nose-picking, anticoagulants, hypertension",
"Family history → hereditary haemorrhagic telangiectasia (Osler-Weber-Rendu)",
],
"D. Anosmia / Hyposmia": [
"Sudden onset: post-URI or post-traumatic",
"Gradual/fluctuating: sinusitis, allergies, neurodegenerative disease",
"Congenital anosmia → Kallmann syndrome (hypogonadism)",
"Distinguish: flavour complaints (smell) vs. basic taste (sweet/sour/salty/bitter — taste)",
],
"E. Facial Pain / Pressure": [
"Forehead → frontal sinus; cheeks → maxillary; between eyes → ethmoid; top of head → sphenoid",
"Worse on bending forward → sinusitis",
"Associated nasal discharge or blockage",
],
"F. Sneezing, Itching, Postnasal Drip": [
"Suggests allergic rhinitis; identify allergens (dust, pollen, animals, occupational)",
"Seasonal vs. perennial pattern",
],
}
for heading, bullets in nose_items.items():
story.append(subsection(heading))
for b in bullets:
story.append(bullet(b))
story.append(spacer(3))
# ── SECTION 4: THROAT ───────────────────────────────────────────────────────────
story += section_header("4. THROAT & LARYNX (Laryngopharyngeal History)")
throat_items = {
"A. Dysphagia (Difficulty Swallowing)": [
"Level: oral / pharyngeal (nasal regurgitation, coughing) / oesophageal",
"Solids only → mechanical obstruction (stricture, carcinoma)",
"Solids and liquids → motility disorder",
"Progressive (→ carcinoma) or intermittent (web, dysmotility)",
"Associated odynophagia, weight loss, hoarseness, regurgitation",
],
"B. Dysphonia / Hoarseness": [
"Duration > 3 weeks → RED FLAG: laryngoscopy mandatory to exclude malignancy",
"Breathy voice → vocal cord palsy; rough/harsh → nodules, laryngitis",
"Strained / effortful voice → spasmodic dysphonia",
"Voice use history: singers, teachers, call-centre workers (vocal abuse)",
"Reflux, smoking history",
],
"C. Sore Throat": [
"Acute vs. chronic; fever",
"Trismus + peritonsillar swelling → peritonsillar abscess",
"Difficulty breathing / muffled voice / drooling → epiglottitis (EMERGENCY)",
"Recurrent tonsillitis: number of episodes per year, days off school/work",
],
"D. Stridor": [
"Inspiratory → supraglottic/glottic; expiratory → subglottic/tracheal; biphasic → fixed obstruction",
"Acute: foreign body, epiglottitis, angioedema",
"Chronic: subglottic stenosis, laryngeal papillomatosis",
"Always a potential airway emergency — act accordingly",
],
"E. Neck Lump": [
"Location, onset, duration, growth rate",
"Constitutional symptoms: fever, night sweats, weight loss → lymphoma",
"Skin changes, fixation to underlying structures",
"Exposure history: TB contact, cat scratch disease, EBV",
"Associated dysphagia, hoarseness, voice change",
],
}
for heading, bullets in throat_items.items():
story.append(subsection(heading))
for b in bullets:
story.append(bullet(b))
story.append(spacer(3))
# ── SECTION 5: DRUG HISTORY ─────────────────────────────────────────────────────
story += section_header("5. DRUG HISTORY — ENT-Relevant Medications")
drug_data = [
["Drug / Class", "ENT Relevance"],
["Aminoglycosides (gentamicin, streptomycin, neomycin)", "Ototoxicity — cochlear and vestibular damage"],
["Loop diuretics (furosemide)", "Ototoxicity, especially combined with aminoglycosides"],
["Cytotoxics (cisplatin, carboplatin)", "Ototoxicity — high-frequency SNHL"],
["Quinine / antimalarials", "Tinnitus, reversible hearing loss"],
["Aspirin / NSAIDs (high dose)", "Reversible tinnitus"],
["ACE inhibitors", "Chronic dry cough (mistaken for laryngeal/throat problem)"],
["Anticoagulants (warfarin, DOACs)", "Epistaxis"],
["Nasal decongestants (oxymetazoline)", "Rhinitis medicamentosa with prolonged use (>5 days)"],
["Bisphosphonates", "Osteonecrosis of the jaw — relevant pre-operatively"],
]
story.append(make_table(drug_data, [7*cm, 10*cm]))
story.append(spacer())
# ── SECTION 6: FAMILY / SOCIAL HISTORY ─────────────────────────────────────────
story += section_header("6. FAMILY & SOCIAL HISTORY")
story.append(subsection("Family History — Key Conditions"))
fh_data = [
["Condition", "Reason"],
["Hearing loss", "Genetic SNHL (connexin 26/GJB2, Pendred, Usher syndromes)"],
["Neurofibromatosis type 2", "Bilateral acoustic neuromas — autosomal dominant"],
["Otosclerosis", "Autosomal dominant, variable penetrance"],
["Hereditary haemorrhagic telangiectasia", "Recurrent severe epistaxis"],
["Head and neck malignancy", "Increased personal risk"],
["Autoimmune disorders", "Sjogren's, SLE — salivary glands, sudden SNHL"],
["Cleft palate / craniofacial abnormalities", "Associated middle ear disease"],
]
story.append(make_table(fh_data, [6*cm, 11*cm]))
story.append(spacer(6))
story.append(subsection("Social History"))
sh_data = [
["Factor", "ENT Relevance"],
["Smoking", "Laryngeal/pharyngeal/oral cancer; chronic rhinitis; worsens OSA"],
["Alcohol", "Head and neck cancer (synergistic with smoking); parotid enlargement"],
["Occupation", "Noise exposure (factory, military, musicians); voice overuse (teachers, singers); woodworking (ethmoid adenocarcinoma)"],
["Recreational activities", "Loud music (NIHL); swimming (otitis externa); diving (barotrauma)"],
["Air travel", "Ear barotrauma, sinus pressure"],
["International travel", "TB (scrofula), rhinoscleroma, leishmaniasis"],
["Sexual history", "HPV (oropharyngeal cancer — base of tongue, tonsil); syphilis; HIV"],
["Pets", "Allergen exposure (cat dander, dog hair)"],
["Bed partner history", "Essential in OSA assessment — corroborates apnoeic episodes"],
]
story.append(make_table(sh_data, [4.5*cm, 12.5*cm]))
story.append(spacer())
# ── SECTION 7: OSA ──────────────────────────────────────────────────────────────
story += section_header("7. SLEEP / OSA HISTORY")
for b in [
"Sleep habits, hygiene, typical sleep/wake times, shift work",
"Daytime sleepiness — Epworth Sleepiness Scale (score > 10 is significant)",
"Observed apnoeic episodes, choking, gasping (bed partner history is invaluable)",
"Morning headaches, nocturia, poor concentration and memory",
"Comorbidities: hypertension, obesity, metabolic syndrome, cardiovascular disease",
"Occupational risk: drivers / heavy machinery operators may have legal reporting implications",
]:
story.append(bullet(b))
story.append(spacer())
# ── SECTION 8: RED FLAGS ────────────────────────────────────────────────────────
story += section_header("8. RED FLAG SYMPTOMS — Always Screen Actively")
rf_data = [
["Red Flag", "Possible Cause — Action"],
["Hoarseness > 3 weeks", "Laryngeal carcinoma → urgent laryngoscopy"],
["Unilateral bloodstained nasal discharge", "Sinonasal malignancy → urgent ENT referral"],
["Unilateral serous otitis media in adult", "Nasopharyngeal carcinoma → nasopharyngoscopy"],
["Progressive unilateral SNHL", "Acoustic neuroma (vestibular schwannoma) → MRI IAMs"],
["Trismus + peritonsillar swelling", "Peritonsillar abscess → urgent drainage"],
["Stridor", "Airway compromise → treat as emergency"],
["Neck lump + constitutional symptoms", "Lymphoma / metastatic carcinoma → urgent biopsy"],
["Progressive dysphagia + weight loss", "Hypopharyngeal / oesophageal carcinoma"],
["Facial nerve palsy + parotid lump", "Parotid malignancy → urgent imaging and biopsy"],
["Unilateral nasal polyp", "Inverted papilloma, malignancy — not simple polyp"],
]
style_rf = TableStyle([
("BACKGROUND", (0, 0), (-1, 0), colors.HexColor("#7B0000")),
("TEXTCOLOR", (0, 0), (-1, 0), colors.white),
("FONTNAME", (0, 0), (-1, 0), "Helvetica-Bold"),
("FONTSIZE", (0, 0), (-1, 0), 8.5),
("FONTNAME", (0, 1), (-1, -1), "Helvetica"),
("FONTSIZE", (0, 1), (-1, -1), 8.5),
("ROWBACKGROUNDS", (0, 1), (-1, -1), [colors.white, colors.HexColor("#FFF5F5")]),
("GRID", (0, 0), (-1, -1), 0.4, MID_GREY),
("VALIGN", (0, 0), (-1, -1), "TOP"),
("LEFTPADDING", (0, 0), (-1, -1), 5),
("RIGHTPADDING", (0, 0), (-1, -1), 5),
("TOPPADDING", (0, 0), (-1, -1), 4),
("BOTTOMPADDING", (0, 0), (-1, -1), 4),
])
rf_table = Table(rf_data, colWidths=[6.5*cm, 10.5*cm], repeatRows=1)
rf_table.setStyle(style_rf)
story.append(rf_table)
story.append(spacer(10))
# Footer note
story.append(HRFlowable(width="100%", thickness=1, color=TEAL, spaceBefore=4, spaceAfter=4))
story.append(Paragraph(
"Sources: K.J. Lee's Essential Otolaryngology (9th ed.) • Cummings Otolaryngology Head and Neck Surgery (7th ed.)",
note_style
))
# Build
doc.build(story)
print(f"PDF saved to: {OUTPUT}")
Running Command
cd /home/daytona/workspace/ent-history && python generate_pdf.py 2>&1
Your printable PDF is ready:
ENT History Taking
PDF Document · PDF
What's included in the PDF:
- General Framework - Opening the consultation + SOCRATES table
- Ear (Otological) - Hearing loss, otalgia, otorrhoea, tinnitus, vertigo (with the K.J. Lee vertigo history table)
- Nose & Sinuses - Obstruction, rhinorrhoea, epistaxis, anosmia, facial pain
- Throat & Larynx - Dysphagia, hoarseness, sore throat, stridor, neck lump
- Drug History - ENT-relevant medications table (ototoxics, anticoagulants, etc.)
- Family & Social History - Genetic conditions + occupational/lifestyle factors
- OSA History - Sleep-specific questions
- Red Flags - Highlighted in red for quick reference
It's formatted A4 with colour-coded section headers and clean tables - suitable for printing or digital use.
This is a shared conversation. Sign in to Orris to start your own chat.