Diabetes mellitus type 2
Reading File
Finding Sources
Searching PubMed
"type 2 diabetes mellitus"[MeSH Terms] AND management
Searching the Web
type 2 diabetes mellitus 2025 guidelines management overview
Reading File
Reading File
Searching PubMed
"type 2 diabetes"[MeSH Terms] AND "drug therapy"[MeSH Terms]
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Searching PubMed
"type 2 diabetes"[MeSH Terms] AND "GLP-1"[tiab]
I now have rich, high-quality content from Harrison's Principles of Internal Medicine 22E (2025). Here is a comprehensive overview:
Diabetes Mellitus Type 2 (T2DM)
1. Definition and Epidemiology
Type 2 diabetes mellitus is a heterogeneous disorder characterized by relative (rather than absolute) insulin deficiency and insulin resistance. It accounts for ~90-95% of all diabetes cases worldwide and is strongly linked to obesity, physical inactivity, aging, and genetic susceptibility. The number of cases continues to rise globally, paralleling the obesity epidemic.
2. Pathogenesis
T2DM develops when the pancreatic beta cells can no longer compensate for insulin resistance. The progression is illustrated by the figure below from Harrison's 22e:
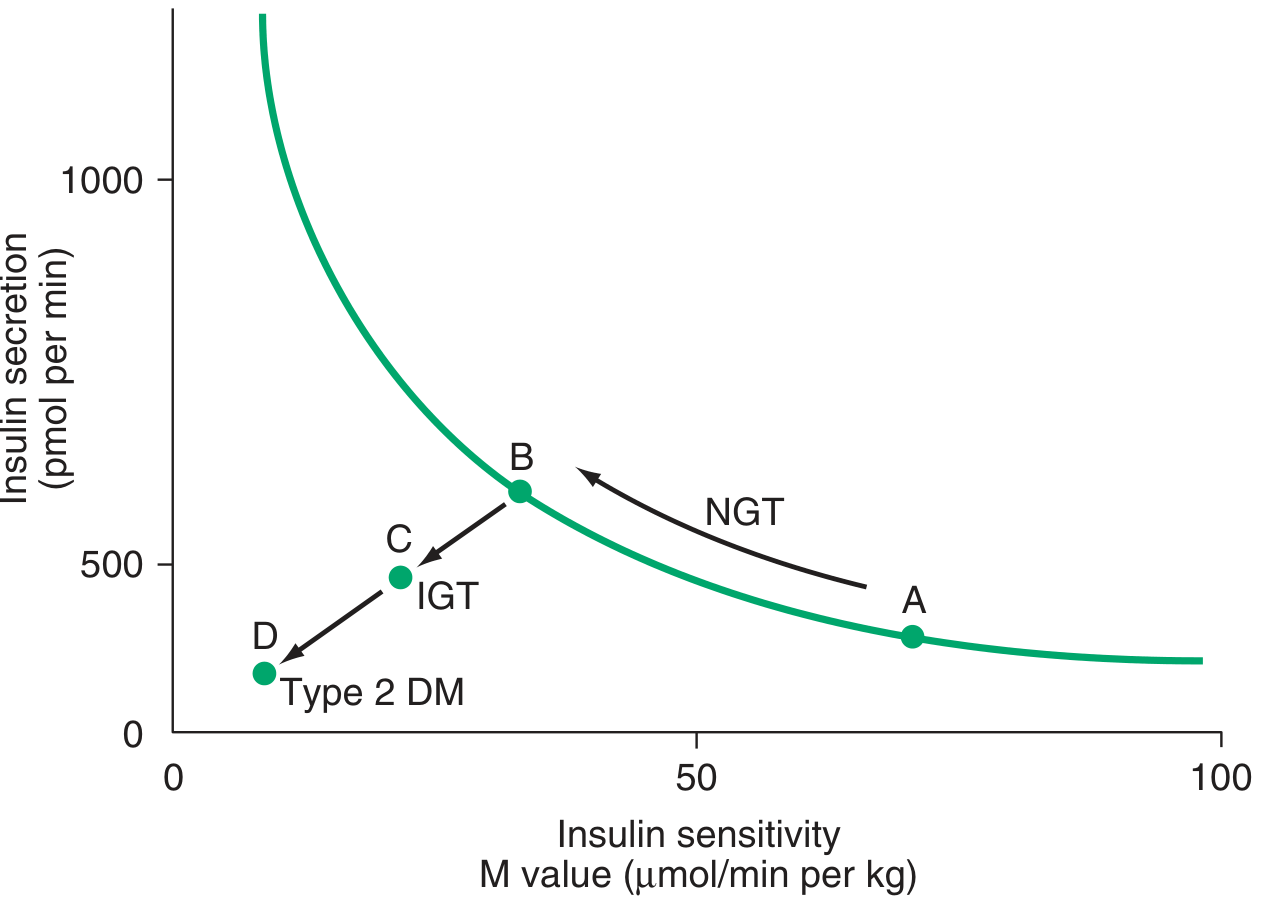
Harrison's Principles of Internal Medicine 22E, Figure 415-6
Key mechanisms:
Insulin Resistance
- Glucose utilization in T2DM is 30-60% lower than in non-diabetic individuals.
- Skeletal muscle is the primary site of impaired insulin-stimulated glucose uptake.
- Molecular defects are largely "post-receptor," involving impaired insulin-regulated phosphorylation cascades.
- Lipid intermediates accumulate within skeletal myocytes, impairing mitochondrial oxidative phosphorylation and reducing insulin-stimulated ATP production.
- Impaired fatty acid oxidation generates reactive oxygen species, producing chronic low-grade metabolic inflammation that further worsens insulin resistance.
Visceral Obesity
- Increased adipocyte mass leads to elevated circulating free fatty acids and adipokines (TNF-alpha, IL-6, resistin, leptin, retinol-binding protein 4).
- Adipose-resident macrophages are an important source of metabolic inflammation.
- Visceral fat drains into the portal circulation, delivering high concentrations of free fatty acids directly to the liver, impairing hepatic insulin signaling.
Beta Cell Failure
- Initially, beta cells compensate by hypersecretion (point B on the graph above).
- Failure to sustain this compensation results first in impaired glucose tolerance (IGT, point C), then frank T2DM (point D).
- Increased glucagon secretion from alpha cells raises hepatic glucose output, accounting predominantly for fasting hyperglycemia, while reduced peripheral uptake causes postprandial hyperglycemia.
3. Diagnosis
Diabetes is diagnosed by any one of the following criteria (confirmed on a repeat test unless clearly symptomatic):
| Test | Diabetes | Prediabetes |
|---|---|---|
| Fasting plasma glucose | ≥ 126 mg/dL (7.0 mmol/L) | 100-125 mg/dL (IFG) |
| 2-h plasma glucose (75g OGTT) | ≥ 200 mg/dL (11.1 mmol/L) | 140-199 mg/dL (IGT) |
| HbA1c | ≥ 6.5% (48 mmol/mol) | 5.7-6.4% |
| Random plasma glucose (with symptoms) | ≥ 200 mg/dL | -- |
HbA1c caveats: Does not capture glycemic variability. Conditions altering red cell lifespan (hemoglobinopathies, anemias, uremia, hemodialysis) can falsify results. African Americans show slightly higher HbA1c (~0.3%) than non-Hispanic whites at the same mean glucose.
4. Glycemic Goals
Goals should be individualized. The general HbA1c target is <7.0% for most adults, with stricter targets (6.0-6.5%) in younger patients with short disease duration and no significant comorbidities, and more lenient targets (7.5-8.5%) in elderly patients, those with frequent hypoglycemia, limited life expectancy, or extensive comorbidities.
Beyond HbA1c, continuous glucose monitoring (CGM) targets:
- Time-in-range (70-180 mg/dL): >70%
- Time below range (<70 mg/dL): <4%
- Time above range (>180 mg/dL): <25%
5. Non-Pharmacologic Management
Medical Nutrition Therapy (MNT)
- Focus on weight loss, high-quality nutrient-dense foods, carbohydrate limits, and cardiovascular risk factor management.
- Mediterranean-style diets rich in monounsaturated and polyunsaturated fats are preferred.
- Avoid fructose- and sucrose-containing beverages.
- Very-low-carbohydrate diets can produce rapid and dramatic glucose lowering in new-onset T2DM.
- Sodium <2300 mg/day. Minimize sleep disruption and shift work.
Exercise
- Increases insulin sensitivity.
- Promotes weight loss.
- Should be a cornerstone alongside MNT before or concurrent with pharmacotherapy.
6. Pharmacologic Management
T2DM is a progressive disorder that ultimately requires multiple agents. Therapy targets the different pathophysiologic defects:
Drug Classes and Mechanisms
| Class | Mechanism | Key Examples | Notes |
|---|---|---|---|
| Biguanides | Reduces hepatic glucose production; modest improvement in peripheral utilization | Metformin | First-line; weight-neutral; cheap; lactic acidosis risk (very rare); hold if GFR <30 mL/min, acidosis, unstable CHF, liver disease; monitor B12 |
| Sulfonylureas | Stimulate insulin secretion via ATP-sensitive K+ channel on beta cells | Glimepiride, Glipizide, Glyburide | Risk of hypoglycemia and weight gain; glimepiride/glipizide preferred (especially in elderly) over glyburide |
| Glinides | Short-acting ATP-K+ channel stimulators | Repaglinide, Nateglinide | Taken before each meal; reduce postprandial glucose |
| Thiazolidinediones (TZDs) | PPAR-gamma agonists; improve insulin sensitivity in muscle and fat | Pioglitazone, Rosiglitazone | Weight gain, fluid retention, bone fractures; contraindicated in heart failure |
| Alpha-glucosidase inhibitors | Delay intestinal carbohydrate absorption | Acarbose, Miglitol | Modest HbA1c reduction; GI side effects |
| DPP-4 inhibitors | Block DPP-4 enzyme, increasing incretin (GLP-1, GIP) levels; glucose-dependent insulin secretion | Sitagliptin, Saxagliptin, Linagliptin | Weight-neutral; low hypoglycemia risk; well-tolerated |
| GLP-1 Receptor Agonists | Mimic GLP-1: glucose-dependent insulin secretion, suppress glucagon, slow gastric emptying, reduce appetite | Semaglutide, Liraglutide, Dulaglutide, Exenatide | Significant weight loss; CV and renal benefits shown in trials; preferred in patients with established CVD or CKD; injectable (some oral formulations now available) |
| SGLT-2 Inhibitors | Block renal glucose reabsorption in proximal tubule; promote glucosuria | Empagliflozin, Canagliflozin, Dapagliflozin | Weight loss; BP lowering; heart failure and renal protective benefits; risk of genital mycotic infections, DKA (including euglycemic); UTI risk |
| Insulin | Exogenous insulin replacement | Multiple formulations (basal, prandial, premix) | Used when severe hyperglycemia, catabolism, or oral agents fail; can be added to any regimen |
Approach to Therapy (Harrison's 22e, ADA 2025 Standards)
- Begin with MNT + exercise in all patients.
- Add metformin as first-line pharmacotherapy unless contraindicated.
- In patients with established ASCVD, heart failure, or CKD: prioritize a GLP-1 RA (with proven CV benefit) or SGLT-2 inhibitor (with heart failure/renal benefits) regardless of HbA1c.
- Escalate or combine agents as T2DM progresses.
- Any therapy that improves glycemic control reduces "glucose toxicity" to beta cells and may transiently improve endogenous insulin secretion.
Weight considerations: Weight gain occurs with insulin, sulfonylureas, and TZDs. Weight-neutral or weight-reducing agents include metformin, GLP-1 RAs, SGLT-2 inhibitors, DPP-4 inhibitors, and alpha-glucosidase inhibitors. The 2025 ADA guidelines specifically add a recommendation to treat T2DM with MASLD/MASH with a GLP-1 RA or dual GIP/GLP-1 RA (tirzepatide).
7. Acute Complications
Diabetic Ketoacidosis (DKA)
- More common in T1DM but can occur in T2DM (especially with SGLT-2 inhibitor use - "euglycemic DKA").
- Features: hyperglycemia (usually >250 mg/dL), elevated ketones (beta-hydroxybutyrate preferred test), metabolic acidosis, Kussmaul respirations, fruity breath, nausea/vomiting.
- Euglycemic DKA with SGLT-2 inhibitors: blood glucose may be normal or mildly elevated due to glucosuria - a diagnostic trap.
Hyperglycemic Hyperosmolar State (HHS)
- Occurs mostly in T2DM.
- Greater hyperglycemia than DKA, leading to hyperosmolality and marked dehydration.
- Without significant ketosis or acidosis.
- High mortality if untreated.
DKA and HHS exist on a continuum; up to one-third of patients have features of both.
8. Chronic Complications
Chronic complications result from both microvascular and macrovascular damage driven by sustained hyperglycemia:
Microvascular:
- Diabetic retinopathy - leading cause of blindness in working-age adults
- Diabetic nephropathy - leading cause of end-stage renal disease
- Diabetic neuropathy - peripheral sensorimotor and autonomic; most common complication
Macrovascular (ASCVD):
- Atherosclerotic cardiovascular disease (coronary artery disease, stroke, peripheral arterial disease) is the leading cause of mortality in T2DM.
- Reduction in cardiovascular risk is paramount.
- All patients with diabetes aged 40-75 with LDL ≥70 mg/dL should be offered statin therapy (AHA/ACC guidelines).
Other:
- Metabolic-associated steatotic liver disease (MASLD/MASH)
- Increased susceptibility to infections
- Periodontal disease
9. Comprehensive Care Beyond Glucose Control
Management must address all cardiovascular risk factors:
| Target | Goal |
|---|---|
| HbA1c | <7.0% (individualized) |
| Blood pressure | <130/80 mmHg |
| LDL cholesterol | <70 mg/dL (high risk); statin therapy |
| Smoking cessation | Mandatory |
| Weight | 5-10% loss improves glycemia significantly |
| Antiplatelet therapy | Aspirin in those with established CVD |
| Annual screenings | Retinopathy, nephropathy (urine albumin/GFR), neuropathy (monofilament), foot exam |
The 2025 ADA Standards of Care emphasize:
- Expanded use of continuous glucose monitoring (CGM)
- Personalized pharmacological approaches (cardiorenal risk-based drug selection)
- Technology integration (automated insulin delivery systems)
- Addressing health disparities and equity in diabetes care
Sources: Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill) | Textbook of Family Medicine 9e | ADA Standards of Care in Diabetes 2025 | ADA 2025 press release
This is a shared conversation. Sign in to Orris to start your own chat.