Pericarditis
Reading File
Finding Sources
Searching PubMed
"pericarditis" AND "management"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
pericarditis ECG electrocardiogram diffuse ST elevation
Now I have comprehensive information. Let me compile a thorough response.
Pericarditis
Definition & Epidemiology
Pericarditis is inflammation of the pericardium — the fibroserous sac surrounding the heart — caused by granulocytic and lymphocytic infiltration. It is the most common pericardial disease encountered clinically, accounting for approximately 5% of all non-ischemic chest pain presentations. Incidence is roughly 27.7 cases/100,000 population/year, with men aged 16–65 at higher risk (RR ~2.0 vs. women).
Etiology
| Category | Examples |
|---|---|
| Idiopathic/Viral (most common in developed world, 80–90%) | Coxsackievirus B, echovirus, EBV, CMV, HIV, influenza |
| Bacterial | TB (most common cause in developing countries), Staphylococcus, Streptococcus |
| Autoimmune/Connective tissue disease | SLE, RA, systemic sclerosis |
| Post-cardiac injury | Dressler syndrome (post-MI, weeks later), post-pericardiotomy |
| Early post-MI pericarditis | 2–4 days after transmural MI (~20%) |
| Uremia | Most common systemic disorder associated |
| Malignancy | Metastatic (lung, breast, lymphoma), primary |
| Radiation | Mediastinal irradiation |
| Drugs | Hydralazine, procainamide, isoniazid, clozapine |
| Other | Sarcoidosis, amyloidosis, aortic dissection |
In SLE, pericarditis associates with disease flare and polyserositis; clinically significant pericarditis develops in <30% overall, but necropsy studies show involvement in 40–80% of SLE patients. — Braunwald's Heart Disease
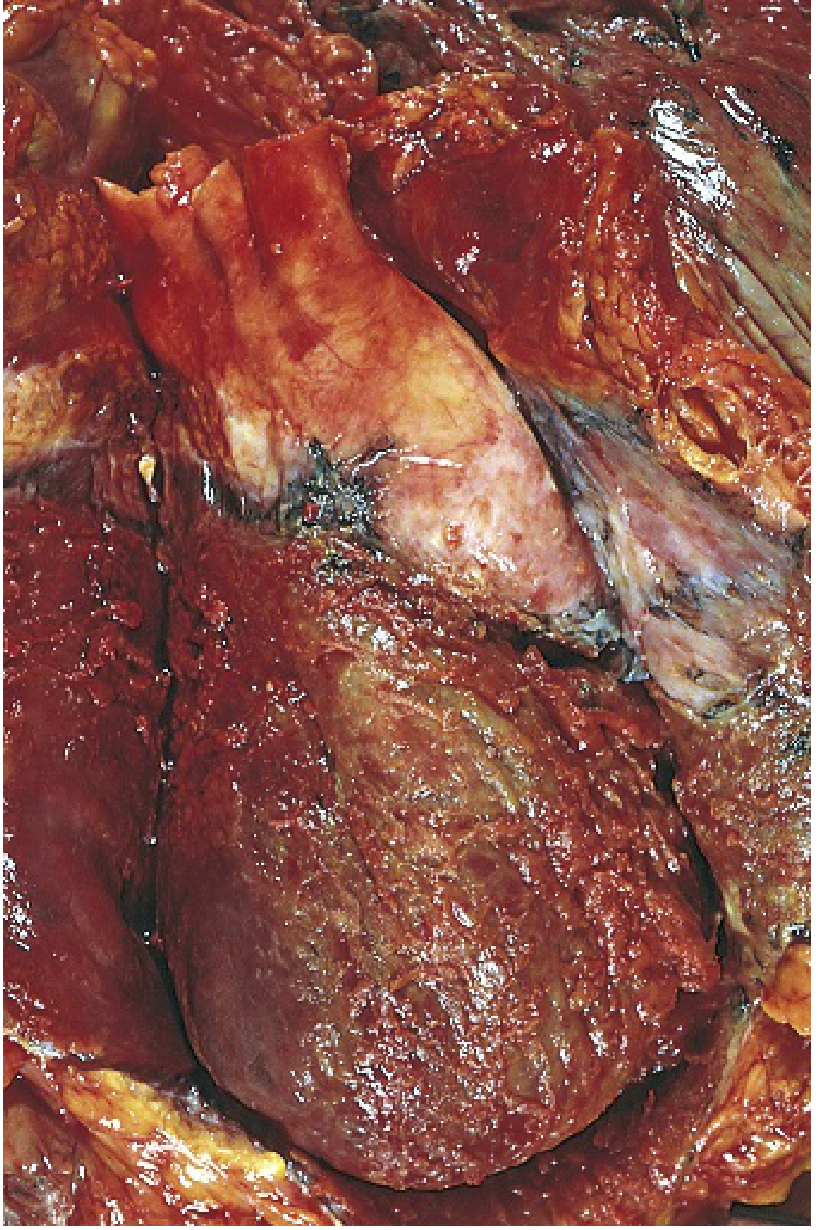
Pathology
Acute: Fibrinous exudate gives the pericardial surface a characteristic shaggy, "bread-and-butter" appearance. Bacterial infection produces fibrinopurulent (suppurative) exudate; TB may show caseation; malignancy produces hemorrhagic effusion.
Chronic/Constrictive: Healing with fibrosis and scar formation can obliterate the pericardial space. In extreme cases, dense encasement prevents normal diastolic expansion — constrictive pericarditis.
Clinical Features
Symptoms
- Chest pain: Sharp, pleuritic; relieved by sitting forward, worsened by lying supine, deep inspiration, or swallowing. Radiates to trapezius ridge or shoulder (pathognomonic of diaphragmatic pleural involvement via phrenic nerve).
- Fever (usually low-grade <38°C), myalgias, malaise
- Dyspnea if effusion is present
Signs
- Pericardial friction rub — pathognomonic; heard in ~1/3 of cases. Best heard at the lower left sternal border with the patient leaning forward in full expiration. Classic rub has 3 components: ventricular systole, early diastole, and atrial contraction. Evanescent and migratory — requires repeated auscultation.
- Sinus tachycardia
- Atrial fibrillation in ~5% of cases
ECG Changes (4 Stages)
| Stage | Findings |
|---|---|
| Stage I | Diffuse concave ("saddle-shaped") ST elevation in most leads; PR depression (except aVR, which shows PR elevation); Spodick's sign (downsloping TP segment) |
| Stage II | ST returns to baseline; T waves flatten |
| Stage III | T-wave inversions |
| Stage IV | ECG normalizes |
Key differentiator from STEMI: diffuse ST elevation across multiple vascular territories (not localized), concave morphology, PR depression, no reciprocal changes (except aVR).

Diagnosis
Diagnostic criteria — at least 2 of 4 required:
- Pericarditic chest pain
- Pericardial friction rub
- New widespread ST elevation or PR depression on ECG
- New or worsening pericardial effusion
Investigations
| Test | Findings |
|---|---|
| ECG | Diffuse ST elevation, PR depression (Stage I) |
| CRP/ESR/WBC | Elevated (CRP used to monitor treatment response and guide tapering) |
| Troponin | Elevated in ~30% (myopericarditis) |
| Echocardiography | Pericardial effusion; rule out tamponade; baseline recommended |
| CXR | Enlarged cardiac silhouette if effusion >250 mL ("water-bottle" heart) |
| CT/CMR | Pericardial thickening, enhancement; CMR best for myocardial involvement |
High-Risk Features (Warrant Hospitalization)
- Fever >38°C
- Subacute onset
- Large effusion
- Cardiac tamponade
- Failure of initial NSAID treatment
- Immunosuppressed state
- Trauma
- Anticoagulant therapy
Treatment
First-Line (Acute Idiopathic/Viral)
| Drug | Dose | Duration | Taper |
|---|---|---|---|
| Aspirin | 750–1000 mg q8h | 1–2 weeks | Decrease every 1–2 weeks over 2–3 weeks |
| Ibuprofen | 600–800 mg q8h | 1–2 weeks | Decrease every week for 2–3 weeks |
| Colchicine (adjunct — reduces recurrences by ~50%) | 0.5 mg once daily (<70 kg) or 0.5 mg bid (≥70 kg) | 3 months | Taper not usually required |
| Gastroprotection (PPI) | With all NSAID regimens | — | — |
- CRP-guided duration: taper once patient is asymptomatic and CRP normalized
- Corticosteroids: reserved for cases refractory to NSAIDs + colchicine, or when NSAIDs are contraindicated (e.g., pregnancy); avoid as first-line — associated with higher recurrence rates
Recurrent Pericarditis
- Repeat NSAIDs + colchicine
- Corticosteroids if refractory (low-dose prednisone, slow taper)
- Anakinra (IL-1β receptor antagonist): promising for colchicine-refractory cases
- Pericardiectomy: last resort
A 2024 meta-analysis confirmed efficacy and safety of IL-1 inhibitors (including anakinra and rilonacept) in recurrent pericarditis management [PMID: 38809412].
Specific Etiologies
- Uremia: Intensive dialysis + NSAIDs (indomethacin 25 mg TID); pericardial window if refractory
- Bacterial/TB: Pathogen-specific antibiotics; TB requires full anti-tuberculous therapy
- Post-MI (Dressler): NSAIDs or aspirin; avoid NSAIDs in early post-MI (impair healing)
- Autoimmune: Treat underlying disease; hydroxychloroquine for SLE
Complications
| Complication | Features |
|---|---|
| Pericardial effusion | Variable size; assess hemodynamic significance |
| Cardiac tamponade | Beck's triad: hypotension, JVD, muffled heart sounds; pulsus paradoxus >10 mmHg; requires urgent pericardiocentesis |
| Constrictive pericarditis | Late sequela; right-sided venous congestion + low CO; similar to restrictive cardiomyopathy; definitive Rx = pericardiectomy |
| Recurrence | Up to 30% of patients; risk factors: fever, large effusion, subacute course, initial NSAID failure |
Prognosis & Disposition
- 60% full recovery within 1 week; ~80% within 3 weeks
- Up to 30% recurrence rate
- Nonviral/non-idiopathic cases have higher rates of progression to constrictive pericarditis
- Athletes should avoid competitive sports until asymptomatic (expert consensus)
- Outpatient management is appropriate for low-risk, uncomplicated cases; hospitalization for high-risk features
Sources: Braunwald's Heart Disease (11e), Rosen's Emergency Medicine, Robbins & Kumar Basic Pathology
Recent evidence note: A 2024 systematic review/meta-analysis [PMID: 38809412] supports IL-1 inhibitors (anakinra, rilonacept) as effective and safe in recurrent pericarditis refractory to conventional therapy. A 2026 systematic review [PMID: 41276190] catalogued drug-induced pericarditis cases — clozapine, hydralazine, and procainamide among the most frequently implicated agents.
This is a shared conversation. Sign in to Orris to start your own chat.