Antiepileptic drug
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have a comprehensive set of information including the mechanism diagram. Let me compile the complete answer.
Antiepileptic Drugs (AEDs)
Overview
Antiepileptic drugs (AEDs), also called antiseizure medications (ASMs) or anticonvulsants, are used to suppress or prevent seizures by modulating neuronal excitability. The goal of therapy is a seizure-free state with minimal side effects. About 70% of epilepsy patients achieve complete or near-complete seizure control with medications; roughly half respond to the first agent tried. The remaining cases are considered treatment-resistant.
- Adams and Victor's Principles of Neurology, 12th Ed.
Mechanisms of Action
AEDs act via five main mechanisms, mapped to excitatory and inhibitory synapses:
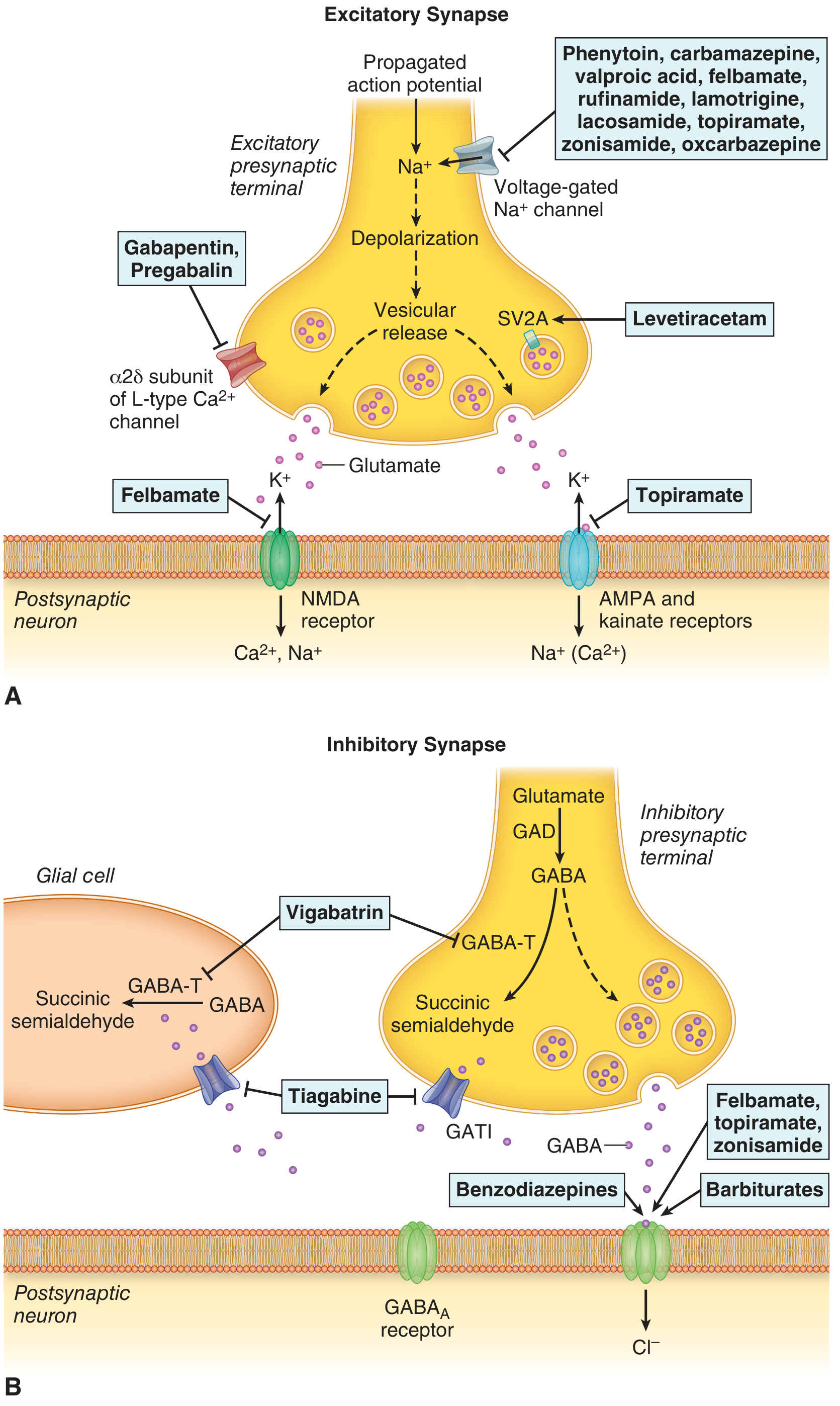
Figure: Schematic of AED sites of action at the excitatory synapse (top) and inhibitory synapse (bottom) - Katzung's Basic and Clinical Pharmacology, 16th Ed.
1. Voltage-Gated Sodium Channel Blockade
Block the fast Na+ channel, preventing abnormal high-frequency neuronal firing. Most act on the inactivated state of the channel (use-dependent/frequency-dependent block).
- Drugs: Phenytoin, carbamazepine, oxcarbazepine, eslicarbazepine, lamotrigine, lacosamide (also enhances slow inactivation), rufinamide, zonisamide, valproate (partial)
2. T-Type Calcium Channel Blockade
Reduces the low-threshold Ca2+ current responsible for thalamic pacemaker activity - the mechanism underlying absence seizures.
- Drugs: Ethosuximide (primary mechanism), valproate (partial)
3. GABA Enhancement
Potentiation of inhibitory GABAergic neurotransmission. This includes:
- GABA-A receptor potentiation (increase Cl- influx): Benzodiazepines (increase frequency of Cl- channel opening), Barbiturates/phenobarbital (increase duration), Topiramate, felbamate, zonisamide
- Block GABA reuptake (GAT-1): Tiagabine
- Inhibit GABA-transaminase (irreversible): Vigabatrin
- Drugs: Benzodiazepines, phenobarbital, primidone, vigabatrin, tiagabine, topiramate, valproate (increases GABA synthesis/levels)
4. Glutamate (Excitatory) Receptor Blockade
Reduce excitatory neurotransmission at NMDA and AMPA receptors.
- AMPA/kainate receptor blockade: Topiramate, perampanel (selective non-competitive AMPA antagonist)
- NMDA receptor antagonism: Felbamate, valproate
5. Synaptic Vesicle Protein SV2A Modulation
Bind to the SV2A protein on synaptic vesicles, reducing vesicular neurotransmitter release.
- Drugs: Levetiracetam, brivaracetam
6. α2δ Subunit of Voltage-Gated Ca2+ Channels
Reduce Ca2+ influx at the presynaptic terminal, decreasing neurotransmitter release.
- Drugs: Gabapentin, pregabalin
Classification and Drug Summary
Table: Major AEDs - Mechanism, Indications, and Limitations
(From Adams and Victor's Principles of Neurology, 12th Ed. - Table 15-5)
| Drug | Mechanism | Principal Indications | Major Limitations |
|---|---|---|---|
| Valproic acid | Multiple: GABA potentiation, NMDA inhibition, Na+ channel, T-type Ca2+ inhibition | Focal + generalized seizures, absence | Hepatic enzyme inhibitor, teratogenicity, weight gain |
| Phenytoin | Na+ channel inhibitor | Focal + generalized seizures | Enzyme inducer, nonlinear kinetics, skin hypersensitivity |
| Carbamazepine | Na+ channel inhibitor | Focal + generalized seizures | Enzyme inducer, skin hypersensitivity, hyponatremia |
| Oxcarbazepine | Na+ channel inhibitor | Focal seizures | Enzyme inducer, hyponatremia |
| Eslicarbazepine | Na+ channel inhibitor | Focal seizures (adjunctive) | Enzyme inducer, hyponatremia |
| Phenobarbital | GABA potentiation | Focal + generalized | Enzyme inducer, sedation, skin sensitivity |
| Lamotrigine | Na+ channel inhibitor | Focal + generalized | Enzyme inducer (mild), skin hypersensitivity (SJS) |
| Levetiracetam | SV2A modulation | Focal + generalized | Mood disturbance, psychosis |
| Brivaracetam | SV2A modulation | Focal + generalized | Less mood/psychosis vs. levetiracetam |
| Topiramate | Multiple: GABA, AMPA blockade, Na+/Ca2+ channels | Focal + generalized | Nephrolithiasis, cognitive impairment, weight loss |
| Lacosamide | Na+ channel inhibition (slow inactivation) | Focal + generalized | - |
| Zonisamide | Na+ channel inhibition | Focal + generalized | Nephrolithiasis, cognitive impairment, weight loss |
| Ethosuximide | T-type Ca2+ channel inhibition | Absence seizures only | Insomnia |
| Gabapentin | α2δ Ca2+ channel inhibition | Focal + generalized (adjunctive) | - |
| Pregabalin | α2δ Ca2+ channel inhibition | Focal + generalized (adjunctive) | Weight gain |
| Perampanel | AMPA inhibition (glutamate) | Focal + generalized (adjunctive) | - |
| Vigabatrin | GABA potentiation (GABA-T inhibitor) | Infantile spasms, focal seizures | Retinal toxicity (permanent visual field defects) |
| Clonazepam | GABA potentiation | Adjunctive only | Tolerance, sedation |
| Diazepam | GABA potentiation | Status epilepticus, adjunctive | Tolerance, sedation |
| Lorazepam | GABA potentiation | Status epilepticus | Tolerance, sedation |
Seizure-Type Specificity
| Seizure Type | First-line Drug(s) |
|---|---|
| Focal (partial) seizures | Carbamazepine, levetiracetam, lamotrigine, lacosamide |
| Generalized tonic-clonic | Valproate, levetiracetam, lamotrigine, topiramate |
| Absence seizures | Ethosuximide (drug of choice), valproate |
| Myoclonic seizures | Valproate, levetiracetam, clonazepam |
| Juvenile myoclonic epilepsy | Valproate (first-line in non-pregnant adults), levetiracetam |
| Lennox-Gastaut syndrome | Valproate, topiramate, rufinamide, clobazam |
| Infantile spasms (West syndrome) | Vigabatrin, ACTH |
| Status epilepticus | Lorazepam/diazepam (first), then phenytoin/fosphenytoin or levetiracetam |
Pharmacokinetics Highlights
- Phenytoin: Dose-dependent (saturable) elimination - small dose increases at high therapeutic levels cause disproportionate rise in serum levels (nonlinear kinetics). Highly protein-bound (~90%).
- Carbamazepine: Autoinduction of its own metabolism (CYP3A4) - doses effective initially may become subtherapeutic weeks later.
- Valproate: Highly protein-bound (90%), t½ 5-16 h, extensively hepatically metabolized.
- Levetiracetam: Minimal protein binding, minimal metabolism, excreted unchanged in urine - important in patients on multiple drugs or with liver disease. Requires dose adjustment in renal failure.
- Gabapentin/Pregabalin: Renally excreted unchanged - dose adjust in renal impairment.
- Lamotrigine: Glucuronidation; valproate markedly inhibits its clearance (double the lamotrigine half-life), requiring slower titration.
- Long half-lives (once-daily dosing): Phenytoin, phenobarbital, ethosuximide.
- Short half-lives (multiple daily doses): Valproate, carbamazepine.
Drug Interactions
| Interaction | Clinical Effect |
|---|---|
| Valproate + phenytoin | Valproate displaces phenytoin from proteins → toxicity |
| Valproate + phenobarbital | Accumulation of phenobarbital |
| Valproate + lamotrigine | Valproate inhibits lamotrigine metabolism → lamotrigine toxicity |
| Phenytoin/carbamazepine + OCP | Enzyme induction → oral contraceptive failure |
| Carbamazepine + erythromycin | Carbamazepine accumulation (toxicity) |
| Phenytoin/phenobarbital + warfarin | Enzyme induction → reduced warfarin levels |
| Valproate + carbamazepine-epoxide | Inhibits epoxide hydrolase → carbamazepine epoxide toxicity |
Levetiracetam is notable for having virtually no pharmacokinetic drug interactions, making it preferred in patients on chemotherapy or anticoagulants.
Special Populations
Pregnancy
- Most teratogenic: Valproate (neural tube defects, cognitive impairment in offspring - highest risk, 6-11% major malformations)
- Safest options: Lamotrigine, levetiracetam (relatively lower teratogenic risk; however, no AED is entirely safe)
- Enzyme-inducing AEDs reduce folic acid levels - folic acid supplementation (4-5 mg/day) is recommended
- Carbamazepine: 1% risk of neural tube defects
Renal Impairment
Dose reduction needed for: levetiracetam, gabapentin, pregabalin, topiramate (partial)
Elderly
All AEDs increase risk of bone loss/osteoporosis via CYP450 induction → vitamin D degradation; supplement with calcium + vitamin D.
Common Adverse Effects by Drug
| Drug | Key Adverse Effects |
|---|---|
| Phenytoin | Gingival hyperplasia, hirsutism, coarsening of facial features, nystagmus, ataxia, diplopia, peripheral neuropathy, osteoporosis |
| Carbamazepine | SIADH/hyponatremia, aplastic anemia (rare), SJS/TEN (especially in HLA-B*1502 carriers), diplopia, ataxia |
| Valproate | Weight gain, tremor, hair loss, hepatotoxicity, pancreatitis, thrombocytopenia, teratogenicity |
| Phenobarbital | Sedation, cognitive dulling, paradoxical hyperactivity in children, dependence |
| Lamotrigine | SJS/TEN (especially with rapid titration or valproate co-administration), headache |
| Levetiracetam | Irritability, mood disturbance, depression, psychosis |
| Topiramate | Word-finding difficulty ("topiramate stupor"), weight loss, metabolic acidosis, kidney stones |
| Vigabatrin | Irreversible concentric visual field constriction (retinal toxicity) |
| Gabapentin/Pregabalin | Sedation, dizziness, weight gain, peripheral edema |
| Benzodiazepines | Tolerance, physical dependence, sedation |
Key Points for Prescribing
- Start with monotherapy at a low dose and titrate upward.
- Approximately 70% are controlled with medication; about 50% respond to the first agent.
- A third or subsequent agent adds very little benefit; polypharmacy is generally avoided.
- Twice-daily or once-daily dosing is preferred for adherence.
- Bone density monitoring is advisable long-term (especially in women on enzyme-inducing AEDs).
- Class-wide, AEDs carry an FDA black-box warning for increased suicidality risk.
- Levetiracetam and carbamazepine are often preferred as first-line due to tolerability and fewer interactions.
- In adolescent/juvenile myoclonic epilepsy, valproate is traditionally first-line (but avoid in women of childbearing potential if possible due to teratogenicity).
Sources: Adams and Victor's Principles of Neurology, 12th Ed. | Katzung's Basic and Clinical Pharmacology, 16th Ed. | Goodman & Gilman's The Pharmacological Basis of Therapeutics
Easy way to revise antiepileptic drugs
Asking for Preferences
Here is a complete mnemonic-based revision guide for all major AEDs:
Antiepileptic Drugs - Mnemonics & Memory Tricks
1. GROUPING BY MECHANISM
Sodium Channel Blockers
"Please Call Lola - Very Lazy, Often Eats Zucchini, Ruining Felbamate's Reputation"
Phenytoin - Carbamazepine - Lamotrigine - Valproate (partial) - Lacosamide - Oxcarbazepine - Eslicarbazepine - Zonisamide - Rufinamide - Felbamate (partial)
GABA Enhancers
"Big Pandas Vigorously Tickle Baby Toads"
Benzodiazepines - Phenobarbital - Vigabatrin - Tiagabine - Barbiturates - Topiramate (partial)
- Vigabatrin = irreversibly inhibits GABA-T (destroys the enzyme that breaks down GABA)
- Tiagabine = blocks GABA reuptake (like an SSRI but for GABA)
- Benzodiazepines = increase frequency of Cl- channel opening
- Barbiturates = increase duration of Cl- channel opening
Memory trick: "Benzo = Frequency, Barb = Duration" (B comes before D alphabetically, like Benzo before Barb)
T-type Calcium Channel Blockers (Absence seizures)
"Every Void Treats Absence"
Ethosuximide - Valproate - Topiramate (partial)
Ethosuximide = ONLY absence seizures. Pure T-type blocker. Nothing else.
Mnemonic: "Ethosux... absence only, other seizures suck for it"
SV2A Modulators
"LEV it up with BRIVaderm"
LEVetiracetam - BRIVaracetam
Both end in -racetam → SV2A
Memory trick: "racetam = race to the vesicle (SV2A)"
α2δ Calcium Channel Blockers
"GABApentin and PREgabalin = GabaA Blockers? No - Alpha-2-Delta!"
Gabapentin, Pregabalin
Both have GABA in the name but do NOT act on GABA receptors - they act on the α2δ subunit of voltage-gated Ca2+ channels.
Trick: "GABApen has GABA in name but that's a LIE - it's Ca2+ channel"
AMPA/Glutamate Blockers
"PERAmpanel = PERA = Pure AMPA blocker"
Perampanel - Topiramate (partial)
2. DRUG OF CHOICE - Quick Recall
"Absence = Ethosux, JME = Val, Status = Loraza→Phenytoin, Infantile = Vigabatrin"
| Seizure | DOC | Mnemonic |
|---|---|---|
| Absence | Ethosuximide | "Ethosux"cess in absence |
| Juvenile Myoclonic Epilepsy (JME) | Valproate | "Val"iant for JME |
| Status Epilepticus | Lorazepam → IV Phenytoin/Levetiracetam | "LAPSE" - Lorazepam Always Precedes Second-line E |
| Infantile Spasms | Vigabatrin + ACTH | "VIG"orous ACTHion for infantile |
| Focal seizures | Carbamazepine / Levetiracetam | "CARVE" - Carbamazepine / leVEtiracetam |
| Trigeminal neuralgia | Carbamazepine | "Car"bamazepine for triGEMinal |
| Bipolar mood stabilizer | Valproate / Lamotrigine | "VaL = Vibe and Love" |
| Neuropathic pain | Gabapentin / Pregabalin | "GabaPain" |
| Migraine prophylaxis | Valproate / Topiramate | "VaTo = Valproate + Topiramate" |
3. SIDE EFFECTS - Unique "Signature" Effects
Each drug has ONE unforgettable signature side effect:
| Drug | Signature Side Effect | Mnemonic |
|---|---|---|
| Phenytoin | Gingival hyperplasia + hirsutism | "PHENYToin → PHYsically ugly" (gums, hair, face coarsening) |
| Carbamazepine | SIADH / hyponatremia | "Carba-WATER-zepine" (dilutes sodium) |
| Valproate | Weight gain + teratogenicity | "Valpro = Valuable but FAT and DANGEROUS in pregnancy" |
| Phenobarbital | Sedation + cognitive dulling | "PHENObarb = PHENOmenally sedating" |
| Lamotrigine | SJS/Stevens-Johnson Syndrome | "LAMOtrigine = LAMEntable skin" |
| Levetiracetam | Irritability / rage | "LEVEtiracetam = LEVEl your rage" |
| Topiramate | Cognitive slowing ("Dopamax") | "TOPIRA = TOP of dumb" - word finding difficulty |
| Topiramate | Kidney stones | "TOPIRAmate = TOPazolite stones" (carbonic anhydrase inhibition) |
| Vigabatrin | Visual field defects (retinal) | "VIGAbatrin → VIsion Gone" |
| Ethosuximide | GI upset + insomnia | "Etho-SUCKS for your stomach" |
| Gabapentin/Pregabalin | Weight gain + sedation | "GABApen = GABAng up the weight" |
4. ENZYME INDUCERS vs. INHIBITORS vs. NEUTRAL
Enzyme INDUCERS (speed up drug metabolism - reduce levels of other drugs)
"Carb Please Permit Barb to Induce"
Carbamazepine - Phenytoin - Primidone - Barbiturates (phenobarbital)
Also: Oxcarbazepine, eslicarbazepine (mild)
Consequence: Reduce OCP levels → contraceptive failure
"INDUCERS = Reduce OCP → Babies"
Enzyme INHIBITOR
Valproate ONLY among classic AEDs
"VALproate = VALidly INhibits everything (accumulates phenytoin, phenobarb, lamotrigine)"
Neutral (no significant interactions)
"LEVetiracetam = LEVel-headed, no interactions" Gabapentin, pregabalin, lacosamide - also minimal interactions
5. TERATOGENICITY - "VALVE"
Valproate (worst - spina bifida, cognitive impairment)
All enzyme inducers reduce folic acid
Lamotrigine (relatively safer)
Vitamin K deficiency caused by enzyme-inducing AEDs (neonatal bleeding)
Every pregnant patient needs folate 4-5 mg/day
"AVOID VALproate in women of childbearing age if possible"
6. RENAL EXCRETION (need dose reduction in CKD)
"LEGS need adjustment in renal failure"
Levetiracetam - Everything gabapentin/pregabalin - Gabapentin - Some topiramate
7. BROAD SPECTRUM vs. NARROW SPECTRUM
Broad Spectrum (work for focal AND generalized):
"VaLe, LeVeL, ToZ, LaCo" Valproate, Lamotrigine, Levetiracetam, Topiramate, Zonisamide, Lacosamide
Narrow Spectrum (focal/tonic-clonic only - can WORSEN absence/myoclonic):
"CBZ PHenyToin = Narrow" - Carbamazepine, Phenytoin These can worsen absence and JME - don't use them!
8. ONE-LINE SUMMARY per Drug
| Drug | One-line |
|---|---|
| Phenytoin | Old Na+ blocker, ugly side effects, nonlinear kinetics |
| Carbamazepine | Na+ blocker, autoinducer, hyponatremia, SJS risk |
| Valproate | Jack-of-all-trades, teratogenic, enzyme inhibitor |
| Ethosuximide | Absence seizures only, T-type Ca2+ blocker |
| Phenobarbital | GABA enhancer, sedating, enzyme inducer, old-school |
| Lamotrigine | Safe in pregnancy (relatively), SJS if titrated fast |
| Levetiracetam | No interactions, renal clearance, causes rage |
| Topiramate | Makes you dumb + thin + get kidney stones |
| Vigabatrin | Infantile spasms, destroys your vision |
| Gabapentin | Alpha-2-delta, NOT a GABA drug despite the name |
| Pregabalin | Gabapentin's smarter sibling - also used for anxiety |
| Lacosamide | New Na+ blocker, slow inactivation, minimal interactions |
| Perampanel | AMPA blocker, once daily, adjunctive |
Quick Revision Flowchart
Seizure type?
├── ABSENCE → Ethosuximide (± valproate)
├── FOCAL → Carbamazepine / Levetiracetam
├── JME/Myoclonic → Valproate / Levetiracetam
├── Generalized TC → Valproate / Lamotrigine / LEV
├── STATUS → Lorazepam → Phenytoin/LEV → Propofol
└── INFANTILE SPASMS → Vigabatrin + ACTH
Print this out, cover the right column, and quiz yourself on each drug's signature effect - that's the fastest way to lock it in!
Create flashcard deck (Anki format) for AEDs
Running Command
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace not found"
Running Command
mkdir -p /home/daytona/workspace/aed-anki
Writing File
~/aed-anki/AED_Flashcards.txt
#separator:tab
#html:true
#notetype:Basic
#deck:Antiepileptic Drugs (AEDs)
#tags:pharmacology neurology AED antiepileptic
What are the 6 main mechanisms of action of antiepileptic drugs? <ol><li><b>Voltage-gated Na⁺ channel blockade</b></li><li><b>T-type Ca²⁺ channel blockade</b></li><li><b>GABA enhancement</b> (receptor potentiation, reuptake block, or metabolism inhibition)</li><li><b>Glutamate receptor blockade</b> (NMDA, AMPA)</li><li><b>SV2A synaptic vesicle modulation</b></li><li><b>α2δ Ca²⁺ channel subunit blockade</b></li></ol>
Which AEDs act by blocking voltage-gated sodium channels? <b>Phenytoin, Carbamazepine, Oxcarbazepine, Eslicarbazepine, Lamotrigine, Lacosamide, Valproate (partial), Zonisamide, Rufinamide, Felbamate (partial)</b><br><br>Mnemonic: <i>"Please Call Lola – Very Lazy, Often Eats Zucchini, Ruining Felbamate's Reputation"</i>
What is the unique mechanism of lacosamide compared to other Na⁺ channel blockers? Lacosamide enhances <b>slow inactivation</b> of voltage-gated Na⁺ channels (not fast inactivation like phenytoin/carbamazepine).<br>This reduces repetitive neuronal firing with less effect on normal neurotransmission.
Which AEDs act via T-type calcium channel blockade? <b>Ethosuximide</b> (primary mechanism) and <b>Valproate</b> (partial)<br><br>T-type Ca²⁺ channels drive thalamic pacemaker oscillations → responsible for <b>absence seizures</b>
What is the mechanism of action of levetiracetam? Binds <b>SV2A</b> (synaptic vesicle glycoprotein 2A) on presynaptic vesicles → reduces vesicular neurotransmitter release<br><br>Mnemonic: <i>"racetam = race to the vesicle"</i>
What is the mechanism of action of gabapentin and pregabalin? Bind the <b>α2δ subunit</b> of voltage-gated Ca²⁺ channels → reduce presynaptic Ca²⁺ influx → reduce neurotransmitter release<br><br>⚠️ Despite having GABA in the name, they do <b>NOT</b> act on GABA receptors
How do benzodiazepines differ from barbiturates in their GABA-A mechanism? <b>Benzodiazepines</b>: increase <b>FREQUENCY</b> of Cl⁻ channel opening<br><b>Barbiturates</b>: increase <b>DURATION</b> of Cl⁻ channel opening<br><br>Mnemonic: <i>"Benzo = Frequency, Barb = Duration"</i> (B before D alphabetically)
What is the mechanism of vigabatrin? <b>Irreversible inhibitor of GABA-transaminase (GABA-T)</b> → prevents GABA breakdown → increases synaptic GABA levels<br><br>Mnemonic: <i>"VIGAbatrin → Very Irrevocably Gorges on GABA-T"</i>
What is the mechanism of tiagabine? Blocks <b>GABA reuptake transporter (GAT-1)</b> → increases synaptic GABA concentration<br><br>Think: "like an SSRI, but for GABA"
What is the mechanism of valproate? <b>Multiple mechanisms:</b><ol><li>Na⁺ channel blockade</li><li>T-type Ca²⁺ channel blockade</li><li>Enhances GABA (increases synthesis, inhibits catabolism)</li><li>NMDA receptor inhibition</li></ol>Truly "broad spectrum" because it hits everything.
What is the drug of choice for absence seizures? <b>Ethosuximide</b> (first-line)<br><b>Valproate</b> (second-line, or if mixed seizure types)<br><br>⚠️ Carbamazepine and phenytoin can <b>WORSEN</b> absence seizures
What is the drug of choice for juvenile myoclonic epilepsy (JME)? <b>Valproate</b> (first-line in males and non-pregnant females)<br><b>Levetiracetam</b> or <b>Lamotrigine</b> (if valproate not suitable, e.g., women of childbearing age)
What is the treatment sequence for status epilepticus? <b>1st line:</b> <b>Lorazepam</b> IV (or diazepam)<br><b>2nd line:</b> <b>Phenytoin/Fosphenytoin</b> or <b>Levetiracetam</b> or Valproate IV<br><b>3rd line (refractory):</b> Propofol, midazolam infusion, or phenobarbital<br><br>Mnemonic: <i>"LAPSE" – Lorazepam Always Precedes Second-line Emergency</i>
What is the drug of choice for infantile spasms (West syndrome)? <b>Vigabatrin</b> + <b>ACTH</b> (adrenocorticotropic hormone)<br><br>Mnemonic: <i>"VIGorous ACTHion for infantile spasms"</i>
Which AED is the drug of choice for trigeminal neuralgia? <b>Carbamazepine</b><br><br>Also used for: bipolar disorder (mood stabilizer), focal seizures
Which AEDs are "broad spectrum" (effective for both focal AND generalized seizures)? <b>Valproate, Lamotrigine, Levetiracetam, Topiramate, Zonisamide, Lacosamide</b><br><br>Mnemonic: <i>"VaLe, LeVeL, ToZ, LaCo"</i>
Which AEDs are "narrow spectrum" and can WORSEN absence/myoclonic seizures? <b>Carbamazepine, Phenytoin, Oxcarbazepine, Gabapentin, Pregabalin, Tiagabine</b><br><br>⚠️ Never use narrow-spectrum AEDs as monotherapy when absence or JME is suspected
What are the unique (signature) side effects of phenytoin? <ul><li><b>Gingival hyperplasia</b></li><li><b>Hirsutism</b></li><li>Coarsening of facial features</li><li>Nystagmus, ataxia, diplopia (toxicity)</li><li>Peripheral neuropathy (long-term)</li><li>Osteoporosis</li><li>Nonlinear (saturable) pharmacokinetics</li></ul>Mnemonic: <i>"PHENYToin = PHYsically ugly"</i>
What is the unique pharmacokinetics of phenytoin? <b>Zero-order (nonlinear/saturable) kinetics</b> at therapeutic levels<br>→ Once plasma levels exceed ~10 µg/mL, small dose increases cause <b>disproportionately large</b> rises in levels and toxicity<br>→ Half-life increases as levels rise (12–36 h)
What are the unique (signature) side effects of carbamazepine? <ul><li><b>SIADH → Hyponatremia</b></li><li><b>Stevens-Johnson Syndrome (SJS)</b> – especially HLA-B*1502 (South/East Asian patients)</li><li>Aplastic anemia (rare)</li><li>Diplopia, ataxia</li><li>Autoinduction of own metabolism</li></ul>Mnemonic: <i>"Carba-WATER-zepine" (dilutes sodium)</i>
What is autoinduction and which AED is famous for it? <b>Carbamazepine</b> induces its own metabolism (CYP3A4)<br>→ Doses adequate at start of therapy become subtherapeutic after <b>weeks</b> as enzyme activity builds up<br>→ Requires dose increases after initial stabilization
What are the unique (signature) side effects of valproate? <ul><li><b>Teratogenicity</b> (neural tube defects, cognitive impairment in offspring)</li><li><b>Hepatotoxicity</b> (especially children under 2 on polytherapy)</li><li>Weight gain</li><li>Tremor</li><li>Hair loss (alopecia)</li><li>Pancreatitis</li><li>Thrombocytopenia</li></ul>Mnemonic: <i>"Valpro = Valuable but FAT, HAIRY-less, and DANGEROUS in pregnancy"</i>
What are the teratogenic risks of valproate specifically? <ul><li><b>Neural tube defects</b> (spina bifida) – ~1–2%</li><li><b>Cognitive impairment</b> in offspring (IQ reduction)</li><li>Major malformation rate: <b>6–11%</b> (highest of all AEDs)</li><li>Fetal valproate syndrome: midface hypoplasia, limb defects</li></ul>⚠️ Avoid in women of childbearing age if possible; use folate 4–5 mg/day if must use
What is the most teratogenic AED? What is the safest? <b>Most teratogenic: Valproate</b> (6–11% major malformation rate)<br><b>Relatively safest: Lamotrigine and Levetiracetam</b><br><br>⚠️ No AED is entirely safe in pregnancy. All patients should take <b>folate 4–5 mg/day</b>
What are the unique (signature) side effects of lamotrigine? <ul><li><b>Stevens-Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN)</b><br>→ Risk increased by: rapid dose titration + valproate co-administration</li><li>Headache, dizziness</li></ul>Mnemonic: <i>"LAMOtrigine = LAMEntable skin"</i><br><br>⚠️ Always titrate SLOWLY, especially with valproate
What are the unique (signature) side effects of levetiracetam? <ul><li><b>Irritability, mood disturbance</b></li><li><b>Depression, psychosis</b> (rare)</li><li>Behavioral changes ("levetiracetam rage")</li></ul>Mnemonic: <i>"LEVEtiracetam = LEVEl your rage"</i><br>Advantage: virtually no pharmacokinetic interactions
What are the unique (signature) side effects of topiramate? <ul><li><b>Cognitive slowing</b> – word-finding difficulty ("Dopamax")</li><li><b>Nephrolithiasis</b> (kidney stones) – carbonic anhydrase inhibition</li><li><b>Weight loss</b></li><li>Metabolic acidosis</li><li>Paraesthesias</li></ul>Mnemonic: <i>"Topiramate = TOP stupidity + kidney TOPaz stones + TOPpling weight"</i>
What are the unique (signature) side effects of vigabatrin? <b>Irreversible, concentric visual field constriction</b> (retinal toxicity/peripheral vision loss)<br><br>→ Up to 30–40% of patients develop visual field defects<br>→ Must monitor with perimetry regularly<br><br>Mnemonic: <i>"VIGAbatrin → VIsion Gone"</i>
What are the side effects of gabapentin and pregabalin? <ul><li>Sedation, dizziness</li><li><b>Weight gain</b></li><li>Peripheral edema</li><li>Ataxia</li></ul>Both require dose reduction in <b>renal impairment</b> (renally excreted)
Which AEDs are hepatic enzyme INDUCERS? <b>Carbamazepine, Phenytoin, Phenobarbital, Primidone</b> (also oxcarbazepine – mild)<br><br>Mnemonic: <i>"Carb Please Permit Barb to Induce"</i><br><br>Consequence: reduce levels of OCP, warfarin, other drugs
Which AED is a hepatic enzyme INHIBITOR? <b>Valproate</b> (only classic AED that inhibits enzymes)<br><br>→ Increases levels of: phenytoin, phenobarbital, lamotrigine (doubles lamotrigine t½!)<br><br>Mnemonic: <i>"VALproate = VALidly INhibits"</i>
Which AEDs have minimal/no pharmacokinetic drug interactions? <b>Levetiracetam</b> (drug of choice for polypharmacy patients)<br><b>Gabapentin, Pregabalin, Lacosamide</b> also minimal interactions<br><br>Why levetiracetam? Minimal protein binding, minimal hepatic metabolism, renal excretion unchanged
How does valproate interact with lamotrigine? Valproate <b>inhibits glucuronidation</b> of lamotrigine → <b>doubles</b> lamotrigine half-life<br>→ Risk of <b>SJS</b> increases greatly<br>→ Must start lamotrigine at <b>half the normal dose</b> and titrate even more slowly
How does valproate interact with phenytoin? Valproate <b>displaces phenytoin from plasma proteins</b> → increased free (active) phenytoin<br>→ <b>Phenytoin toxicity</b> despite normal total levels<br>→ Measure <b>free phenytoin</b> levels if co-administering
Which AEDs require dose reduction in renal impairment (CKD)? <b>Levetiracetam, Gabapentin, Pregabalin, Topiramate (partial)</b><br><br>Mnemonic: <i>"LEGS need adjustment in renal failure"</i><br>L=Levetiracetam, E=Everything gabapentinoid, G=Gabapentin, S=Some topiramate
What effect do enzyme-inducing AEDs have on oral contraceptives? Reduce OCP plasma levels via CYP450 induction → <b>contraceptive failure</b><br><br>Affected drugs: Carbamazepine, Phenytoin, Phenobarbital, Primidone<br><br>→ Use higher-dose OCP or alternative contraception (IUD preferred)
What effect do AEDs have on bone health? Most AEDs (especially enzyme inducers) increase risk of <b>osteoporosis and fracture</b><br><br>Mechanism: CYP450 induction → increased vitamin D degradation → reduced Ca²⁺ absorption<br><br>Management: Calcium + Vitamin D supplementation; periodic DEXA scan
What is the class-wide FDA warning for all AEDs? All AEDs carry an <b>FDA black-box warning for increased risk of suicidality</b> (suicidal ideation and behavior)<br><br>Applies to patients with epilepsy AND psychiatric conditions
What are the pharmacokinetics of levetiracetam? <ul><li>Oral bioavailability: >95%</li><li>Minimal protein binding (<10%)</li><li>Minimal hepatic metabolism (hydrolysed in blood)</li><li>Excreted <b>unchanged</b> in urine (~66%)</li><li>t½: 6–11 h</li><li>No significant drug interactions</li></ul>
What is the half-life of phenobarbital and what does this mean clinically? t½ = <b>80–120 hours</b> (very long)<br>→ Once-daily dosing<br>→ Takes <b>weeks</b> to reach steady state<br>→ Also takes weeks to clear after stopping (useful in neonatal seizures, longer time window)<br>→ Slow titration needed
What is the role of carbamazepine epoxide and why does it matter clinically? Carbamazepine is metabolized to <b>carbamazepine-10,11-epoxide</b>, which is pharmacologically active and contributes to toxicity<br><br>Valproate inhibits epoxide hydrolase → <b>epoxide accumulates</b> → toxicity even with normal carbamazepine levels<br>→ Measure epoxide separately if unexplained toxicity
What is the mechanism and use of ethosuximide? <b>Mechanism:</b> T-type Ca²⁺ channel blocker (reduces thalamic pacemaker bursting)<br><b>Use:</b> <b>Absence seizures ONLY</b><br><b>Not effective for</b> focal or tonic-clonic seizures<br><br>Mnemonic: <i>"Ethosux... absence only, other seizures suck for it"</i>
What is the mechanism, use, and key side effect of perampanel? <b>Mechanism:</b> Selective non-competitive antagonist at postsynaptic <b>AMPA receptors</b> (blocks glutamate excitation)<br><b>Use:</b> Adjunctive therapy for focal and primary generalized tonic-clonic seizures<br><b>Side effects:</b> Dizziness, somnolence, behavioral/psychiatric effects<br><b>Dosing:</b> Once daily (long t½ ~105 h)
What are the indications for topiramate beyond epilepsy? <ol><li><b>Migraine prophylaxis</b></li><li><b>Weight loss</b> (combined with phentermine as Qsymia)</li><li>Binge eating disorder</li></ol>
What are the indications for valproate beyond epilepsy? <ol><li><b>Bipolar disorder</b> (mood stabilizer)</li><li><b>Migraine prophylaxis</b></li><li>Schizoaffective disorder (adjunctive)</li></ol>
What are the indications for gabapentin and pregabalin beyond epilepsy? <b>Gabapentin:</b><ol><li>Neuropathic pain (diabetic neuropathy, post-herpetic neuralgia)</li><li>Restless legs syndrome</li></ol><b>Pregabalin:</b><ol><li>Neuropathic pain</li><li>Generalized anxiety disorder (GAD)</li><li>Fibromyalgia</li></ol>
What is the mechanism behind AED-associated SJS/TEN and which drugs most commonly cause it? Mechanism: Immune-mediated (T-cell) reaction to drug-protein hapten complexes → keratinocyte apoptosis<br><br><b>Most common AED causes:</b> Carbamazepine, Lamotrigine, Phenytoin, Oxcarbazepine<br><br>Risk factors: HLA-B*1502 (carbamazepine in South/East Asian patients) — mandatory genetic screening before prescribing carbamazepine in these populations
Summarize the AED drug of choice for each seizure type in one line each. <table><tr><th>Seizure Type</th><th>Drug of Choice</th></tr><tr><td>Absence</td><td>Ethosuximide</td></tr><tr><td>JME</td><td>Valproate / Levetiracetam</td></tr><tr><td>Focal</td><td>Carbamazepine / Levetiracetam</td></tr><tr><td>Generalized TC</td><td>Valproate / Lamotrigine / LEV</td></tr><tr><td>Status epilepticus</td><td>Lorazepam → Phenytoin/LEV</td></tr><tr><td>Infantile spasms</td><td>Vigabatrin + ACTH</td></tr><tr><td>Trigeminal neuralgia</td><td>Carbamazepine</td></tr><tr><td>Neuropathic pain</td><td>Gabapentin / Pregabalin</td></tr><tr><td>Migraine prophylaxis</td><td>Valproate / Topiramate</td></tr></table>
What is the first drug to use in a patient with epilepsy on multiple medications (polytherapy) where drug interactions are a concern? <b>Levetiracetam</b><br><br>Reasons:<ul><li>No hepatic enzyme induction or inhibition</li><li>Minimal protein binding</li><li>No significant interactions with chemotherapy, anticoagulants, or other AEDs</li></ul>
What AED should be AVOIDED in young women of childbearing age, and why? <b>Valproate</b><br><br>Reasons:<ul><li>Highest teratogenic risk (6–11% malformation rate)</li><li>Neural tube defects</li><li>Cognitive impairment in offspring</li></ul>Alternatives: Lamotrigine, Levetiracetam (if monotherapy needed)
Name the AED associated with each mnemonic: (1) "Dopamax" (2) "Carba-WATER-zepine" (3) "VIsion Gone" (4) "PHYsically ugly" <ol><li>"Dopamax" = <b>Topiramate</b> (cognitive slowing)</li><li>"Carba-WATER-zepine" = <b>Carbamazepine</b> (hyponatremia/SIADH)</li><li>"VIsion Gone" = <b>Vigabatrin</b> (retinal toxicity)</li><li>"PHYsically ugly" = <b>Phenytoin</b> (gingival hyperplasia, hirsutism, coarse features)</li></ol>
What is the mechanism of action of phenobarbital? What seizures is it used for? <b>Mechanism:</b> Enhances GABA-A receptor function by increasing duration of Cl⁻ channel opening; at high doses, directly opens Cl⁻ channels<br><b>Indications:</b> Focal + generalized tonic-clonic seizures; neonatal seizures; status epilepticus (2nd/3rd line)<br><b>Side effects:</b> Sedation, cognitive dulling, paradoxical hyperactivity in children, tolerance, dependence
What is fosphenytoin and when is it used? <b>Fosphenytoin</b> is a water-soluble <b>prodrug of phenytoin</b><br>→ Rapidly converted to phenytoin in vivo<br><b>Advantages over IV phenytoin:</b><ul><li>Can be given IM</li><li>Faster IV administration (less cardiovascular risk)</li><li>No propylene glycol vehicle → less hypotension/arrhythmia</li></ul><b>Used for:</b> Status epilepticus (IV/IM), acute seizure management
How is AED blood level monitoring used clinically? <b>Useful for:</b> Phenytoin (narrow TI, nonlinear kinetics), carbamazepine, phenobarbital, valproate<br><br><b>Free drug levels</b> should be measured in:<ul><li>Hypoalbuminemia</li><li>Renal failure (uremia alters protein binding)</li><li>Suspected drug interactions displacing from proteins</li></ul><br>Levetiracetam, gabapentin, lamotrigine: levels less routinely monitored
What is the monitoring required for patients on vigabatrin? Regular <b>visual field testing (perimetry)</b><br>→ Due to risk of irreversible concentric visual field constriction (peripheral vision loss)<br>→ Monitoring frequency: every 3–6 months during treatment<br>→ The visual toxicity is dose-related and usually irreversible
What folate supplementation is recommended for pregnant women on AEDs? <b>4–5 mg/day</b> of folic acid (high-dose)<br><br>Rationale: Enzyme-inducing AEDs (carbamazepine, phenytoin, phenobarbital) reduce folate levels → increased risk of neural tube defects<br><br>⚠️ Start BEFORE conception ideally
What is the significance of HLA-B*1502 in AED prescribing? <b>HLA-B*1502</b> allele is associated with <b>carbamazepine-induced SJS/TEN</b><br>→ Predominantly in <b>South and Southeast Asian</b> populations (Han Chinese, Thai, Malaysian)<br><b>Clinical implication:</b> Screen for HLA-B*1502 before prescribing carbamazepine in Asian patients<br>Also relevant: HLA-A*3101 (carbamazepine hypersensitivity in Europeans/Japanese)
Which AEDs are safe to use as monotherapy in absence epilepsy and which are contraindicated? <b>Safe (first-line):</b> Ethosuximide, Valproate, Lamotrigine<br><br><b>Contraindicated/worsen absence:</b> Carbamazepine, Phenytoin, Oxcarbazepine, Gabapentin, Tiagabine, Vigabatrin<br><br>⚠️ These drugs can precipitate or worsen absence and myoclonic seizures
What AED can be used for both epilepsy AND bipolar disorder AND migraine? <b>Valproate (Valproic acid / Divalproex sodium)</b><br><br>Triple role:<ul><li>Broad-spectrum AED</li><li>Mood stabilizer in bipolar disorder</li><li>Migraine prophylaxis</li></ul>
What is the mechanism of action of rufinamide? <b>Na⁺ channel blocker</b> (limits sustained firing) with additional mechanisms<br><b>Use:</b> Adjunctive therapy for <b>Lennox-Gastaut syndrome</b> (drop attacks)<br><b>Pharmacokinetics:</b> t½ 6–10 h; well absorbed (>85%); minimal protein binding (35%)
What drugs are used for Lennox-Gastaut syndrome? <ul><li><b>Valproate</b></li><li><b>Topiramate</b></li><li><b>Rufinamide</b></li><li><b>Clobazam</b></li><li><b>Lamotrigine</b> (reduces drop attacks)</li><li><b>Felbamate</b> (reserved – hepatotoxicity/aplastic anemia risk)</li></ul>
What is the clinical significance of carbamazepine-induced SIADH? Carbamazepine stimulates ADH secretion → <b>syndrome of inappropriate ADH (SIADH)</b> → dilutional <b>hyponatremia</b><br><br>→ Can cause confusion, seizures, nausea, coma if severe<br>→ Monitor serum sodium (Na⁺), especially in elderly<br>→ Oxcarbazepine causes hyponatremia more frequently than carbamazepine
Compare levetiracetam and brivaracetam. Both are <b>SV2A ligands</b> with similar mechanisms<br><br><b>Brivaracetam advantages:</b><ul><li>Higher affinity for SV2A</li><li>Less behavioral/psychiatric side effects than levetiracetam</li><li>Fewer drug interactions</li></ul><b>Levetiracetam:</b> More widely used, well-established efficacy data
What is the general principle for starting antiepileptic therapy? <ul><li>Start with <b>monotherapy</b> at a low dose</li><li>Titrate up slowly</li><li>Prefer <b>once or twice daily dosing</b> for adherence</li><li>70% patients controlled with medications</li><li>~50% respond to first agent</li><li>3rd+ agent adds very little benefit</li><li>Combination of some newer drugs may be more successful than older polytherapy</li></ul>
When is it appropriate to discontinue AEDs? After <b>2–5 seizure-free years</b> (depending on epilepsy type/syndrome)<br><br>Factors favoring discontinuation: single seizure type, normal EEG, normal MRI, seizure-free >2 years<br><br>Factors against: JME (high relapse rate ~90%), abnormal MRI, abnormal EEG, symptomatic epilepsy<br><br>Taper slowly over <b>months</b> to avoid withdrawal seizures
Running Command
wc -l /home/daytona/workspace/aed-anki/AED_Flashcards.txt && echo "---" && head …
Your Anki deck is ready:
AED Flashcards
Text File · TXT
What's inside - 65 cards across 9 categories:
| Category | Cards |
|---|---|
| Mechanisms of Action | 10 cards |
| Drug of Choice by Seizure Type | 9 cards |
| Broad vs Narrow Spectrum | 2 cards |
| Side Effects (signature per drug) | 12 cards |
| Pharmacokinetics | 7 cards |
| Drug Interactions | 7 cards |
| Special Populations (pregnancy, renal, elderly) | 6 cards |
| Mnemonics recall | 3 cards |
| Clinical principles (when to start/stop) | 9 cards |
How to import into Anki:
- Open Anki → click Import File
- Select
AED_Flashcards.txt - Confirm settings:
- Separator: Tab (auto-detected)
- Notetype: Basic
- Deck: Antiepileptic Drugs (AEDs) (auto-created)
- Click Import - done!
The cards use HTML formatting (bold, lists, tables) so answers display cleanly in Anki. All the mnemonics from the previous session are embedded directly into the relevant cards so context and memory trick appear together.
This is a shared conversation. Sign in to Orris to start your own chat.