Diabetic Neuro pathy
Reading File
Finding Sources
Searching PubMed
"diabetic neuropathy"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"diabetic peripheral neuropathy"[MeSH Terms] AND "pain management"
Finding Sources
Searching PubMed
"diabetic neuropathy" AND pathogenesis
Reading File
Reading File
Now I have comprehensive information from multiple authoritative textbooks. Let me compile this into a thorough response.
Diabetic Neuropathy
Overview
Diabetic neuropathy is the most common cause of peripheral neuropathy in developed countries, affecting an estimated ~50% of diabetic patients over their lifetime. Up to 80% of those who have had diabetes for more than 15 years show some evidence of peripheral nerve damage. The prevalence at the time of diagnosis is around 15%, rising to 50% after 25 years of disease.
- Adams and Victor's Principles of Neurology, p. 2367
- Robbins & Kumar Basic Pathology, p. 461
Classification of Diabetic Neuropathies
Diabetes causes several distinct neuropathic syndromes, which may occur alone or in combination:
| Type | Key Features |
|---|---|
| Distal symmetric sensorimotor polyneuropathy (DSPN) | Most common; sensory loss starting in toes, ascending "stocking-glove" |
| Autonomic neuropathy | Orthostatic hypotension, gastroparesis, bowel/bladder/sexual dysfunction |
| Diabetic radiculoplexopathy (amyotrophy / Bruns-Garland syndrome) | Asymmetric proximal lower limb pain, weakness, atrophy |
| Cranial mononeuropathy | Third nerve palsy most common (pupil-sparing); sixth nerve also affected |
| Peripheral mononeuropathy/multiple mononeuropathy | Median neuropathy at wrist (CTS), ulnar at elbow, peroneal at fibular head |
| Painful diabetic cachexia | Severe pain, weight loss, rare |
- Harrison's Principles of Internal Medicine 22E, p. 587
- Adams and Victor's, p. 2369
1. Distal Symmetric Sensorimotor Polyneuropathy (DSPN)
The most common form. Sensory axons are more severely affected than motor axons.
Clinical features:
- Paresthesias, numbness, tingling, burning pain beginning in the toes
- Gradual ascent up the legs in a "stocking" distribution; eventually involves fingers/arms ("glove" distribution)
- Severe cases: sensory loss on the trunk (first midline anteriorly, then laterally)
- Deep aching pains may be present
- Loss of ankle reflexes is typical
- Large-fiber loss: reduced vibration, proprioception; small-fiber loss: reduced pain/temperature
Nerve biopsy findings:
- Axonal degeneration (dying-back centripetal pattern)
- Segmental demyelination and remyelination
- Endothelial hyperplasia and microvascular changes in endoneurial capillaries
- Thickened/duplicated basement membranes of intraneural capillaries
- Painless form affects large fibers; painful form shows depletion of small myelinated and unmyelinated fibers with active regeneration generating neuropathic pain
Nerve conduction studies (NCS):
-
Reduced amplitudes
-
Mild to moderate slowing of conduction velocities
-
Proximodistal gradient
-
Bradley and Daroff's Neurology, p. 961
-
Harrison's 22E, p. 589
2. Autonomic Neuropathy
Usually accompanies DSPN. Can manifest as:
- Cardiovascular: Resting tachycardia, orthostatic hypotension, exercise intolerance, loss of heart rate variability
- Sudomotor: Anhidrosis, heat intolerance, hyperhidrosis
- GI: Gastroparesis (nausea, vomiting, early satiety, bloating), nocturnal diarrhea alternating with constipation
- Genitourinary: Cystopathy (urinary retention), erectile dysfunction, retrograde ejaculation, female sexual dysfunction
- Pupillary: Reduced pupillary response to darkness
- Dry eyes and mouth
Abnormal tests include sympathetic skin responses and quantitative sudomotor axon reflex testing (QSART).
- Harrison's 22E, p. 591
3. Diabetic Amyotrophy (Radiculoplexopathy / Bruns-Garland Syndrome)
-
Presents with severe pain in the low back, hip, and thigh - often unilateral
-
Weakness and atrophy of proximal and distal muscles develop within days to weeks
-
Often accompanied by dramatic weight loss
-
Is the presenting feature of DM in ~1/3 of patients
-
CSF protein is usually elevated; ESR is often raised
-
EMG/NCS: active denervation in proximal/distal limb muscles and paraspinal muscles
-
Nerve biopsy may show axonal degeneration and perivascular inflammation
-
Gradual spontaneous recovery is typical but residual deficits are common; high-dose glucocorticoids are sometimes used in the acute phase (evidence is limited)
-
Harrison's 22E, p. 596
4. Cranial and Peripheral Mononeuropathies
- Third nerve palsy: Most common cranial mononeuropathy in diabetics; typically pupil-sparing (distinguishes it from compressive CN III palsy which affects the pupil)
- Sixth nerve palsy: Next most common
- Seventh nerve palsy: Relatively common but may have non-diabetic etiologies
- Peripheral: Median nerve at wrist, ulnar at elbow, peroneal at fibular head, lateral femoral cutaneous nerve (meralgia paresthetica)
- Mechanism: ischemic infarction of nerve fascicles from vasa nervorum occlusion
Pathogenesis
The pathogenesis is complex and multifactorial:
| Mechanism | Detail |
|---|---|
| Polyol pathway | Hyperglycemia activates aldose reductase → accumulation of sorbitol and fructose in nerve tissue |
| Advanced glycation end products (AGEs) | Cross-link nerve proteins, impair function |
| Oxidative stress | Auto-oxidation of glucose generates reactive oxygen species (ROS), causing nerve injury |
| Protein kinase C (PKC) activation | Causes vascular damage in endoneurial vessels |
| Myoinositol depletion | Competitive inhibition of myoinositol uptake reduces Na+/K+-ATPase activity |
| Endoneurial ischemia/hypoxia | Endothelial hyperplasia narrows endoneurial capillaries → reduced nerve blood flow → axonal atrophy, reduced NCV |
| Neurotrophic factor deficiency | Reduced NGF, VEGF, erythropoietin in diabetic nerves |
| Autoimmune mechanisms | Perivascular inflammation found in proximal radiculoplexus syndromes |
| Insulin deficiency | Impairs neurotrophin signaling independent of glucose control |
The predominant current view is that microvascular occlusion of the vasa nervorum (endoneurial capillaries and epineural arterioles with thickened, hyalinized basement membranes) is central to most forms of diabetic neuropathy.
- Bradley and Daroff's Neurology, p. 968-974
- Adams and Victor's, p. 2427-2434
Diagnosis
- Clinical examination: Loss of vibration and position sense (posterior column), reduced ankle jerks, reduced monofilament sensation
- Nerve conduction studies (NCS) / EMG: Reduced amplitudes, slowed velocities; denervation in amyotrophy
- Quantitative sensory testing (QST)
- Skin punch biopsy: Intraepidermal nerve fiber density - most sensitive for small-fiber neuropathy
- Autonomic testing: Heart rate variability, Valsalva ratio, tilt-table testing, QSART
- Lab: HbA1c, B12 levels (metformin reduces B12 absorption), folate, TSH (to exclude other causes)
Treatment
Glycemic Control (Primary Prevention)
Strict glycemic control is the cornerstone of management and the best way to prevent or slow progression. It is most effective early; in long-standing disease, hypoglycemia unawareness may limit targets.
Lifestyle Modifications
- Exercise and diet have evidence for benefit in type 2 DM with DSPN
- Avoid neurotoxins: alcohol, smoking
- Correct vitamin deficiencies (B12, folate)
Pain Management in Painful DSPN
First-line agents (no head-to-head comparisons exist; switching is reasonable if no response):
| Drug Class | Examples | Notes |
|---|---|---|
| SNRIs | Duloxetine, venlafaxine, desvenlafaxine | FDA-approved for painful diabetic neuropathy |
| Gabapentinoids | Pregabalin, gabapentin | FDA-approved; effective for neuropathic pain |
| TCAs | Amitriptyline, nortriptyline | Efficacious; limited by side effects (anticholinergic) |
| Sodium channel blockers | Carbamazepine, lidocaine patch | Variable efficacy |
| Topical capsaicin patch (8%) | - | Some efficacy; depletes substance P |
| Tapentadol | - | FDA-approved centrally acting opioid; modest efficacy; addiction risk - NOT first-line |
Opioids are not first-line due to modest efficacy and addiction risk. Referral to a pain management center may be needed for refractory cases.
- Harrison's 22E, p. 1673-1674
Autonomic Neuropathy Management
- Orthostatic hypotension: Salt and fluid intake, compression stockings, avoid dehydration and diuretics, physical activity; pharmacologic: midodrine, droxidopa (FDA-approved)
- Resting tachycardia: Beta-blockers (with caution if hypoglycemia unawareness)
- Gastroparesis: Dietary modification (small frequent meals), metoclopramide, erythromycin (short-term)
- Erectile dysfunction: PDE-5 inhibitors, referral to urology
- GI symptoms in type 1 DM: Evaluate for associated celiac disease
Foot Care (Critical)
-
Daily foot inspection for cracks, fissures, ulcers, or inflammation
-
Avoid walking barefoot; wear protective footwear at all times
-
Avoid heating pads on feet (thermal injury risk)
-
Podiatry referral for deformities, calluses, nonhealing ulcers
-
Charcot foot deformity results from undetected repeated fractures from loss of protective sensation
-
Goldman-Cecil Medicine, p. 1425-1435
Risk Factors for Development
- Long duration of diabetes (strongest predictor)
- Poor glycemic control
- Presence of retinopathy and nephropathy
- Age > 50 years
- Type 1 and type 2 both susceptible (rates similar)
- Metabolic syndrome components: hypertension, hypertriglyceridemia, obesity
- Smoking (promotes microvascular disease)
Recent Literature
Recent reviews in the literature include:
- Zhu et al. (2023) - "Diabetic peripheral neuropathy: pathogenetic mechanisms and treatment" [PMID: 38264279]
- Strand et al. (2024) - "Diabetic Neuropathy: Pathophysiology Review" [PMID: 38558164] - Curr Pain Headache Rep
- Yang et al. (2025) - "Diabetic neuropathy: cutting-edge research and future directions" [PMID: 40274830] - Signal Transduct Target Ther
These are primarily review articles and do not significantly change the management recommendations outlined above from the 2025 Harrison's edition.
Key take-home points:
- DSPN is the most common form - stocking-glove sensory loss with neuropathic pain
- Glycemic control is the only disease-modifying treatment; symptomatic pain treatment only manages symptoms
- Multiple mechanisms converge on endoneurial ischemia and metabolic nerve injury
- Foot care and daily foot inspection are non-negotiable to prevent ulceration and amputation
- Autonomic neuropathy carries significant morbidity - cardiac, GI, and genitourinary involvement must all be screened for
?
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Here is the deep dive:
Distal Symmetric Sensorimotor Polyneuropathy (DSPN) - Deep Dive
What It Is
DSPN is the most common form of diabetic neuropathy and one of the most common neuropathies overall in developed countries. It accounts for more hospitalizations than all other diabetic complications combined and is responsible for 50-75% of nontraumatic lower-extremity amputations.
- Washington Manual of Medical Therapeutics, p. 4953
Clinical Presentation
DSPN manifests as a length-dependent neuropathy - the longest axons fail first, so symptoms begin in the toes and feet before ascending.
Symptom Progression
Toes → Feet → Ankles → Lower legs → Fingers → Hands → Forearms
(classic "stocking-glove" distribution)
Advanced: sensory loss on trunk (midline anteriorly first, then laterally)
Up to 50% of patients are asymptomatic - neuropathy is detected only on screening. This is why annual screening is mandatory.
Positive (Painful) Symptoms
These arise from abnormal spontaneous discharges from damaged and regenerating small fibers:
- Burning pain, especially in feet
- Tingling and paresthesias
- Electric-shock-like sensations
- Hyperesthesia (even light touch is painful)
- Dysesthesias (unpleasant, abnormal sensations to touch)
- Pain is typically worse at night and at rest
Negative (Loss) Symptoms
- Numbness and sensory loss
- Loss of pain and temperature sensation (small fiber loss)
- Loss of vibration and proprioception (large fiber loss)
- Difficulty with balance (due to proprioceptive loss)
- Loss of ankle deep-tendon reflexes (early and reliable sign)
Motor Involvement (Later)
- Distal muscle wasting and weakness
- Foot drop (peroneal involvement)
- Foot deformities (hammer toes, high arch) from intrinsic muscle imbalance
Key Clinical Course Note
In painful DSPN, pain often paradoxically subsides as the neuropathy worsens - because the fibers generating the pain are eventually destroyed. Persistent sensory deficit remains even after pain resolves. This can falsely reassure the patient.
- Harrison's 22E, p. 1647-1648
Histopathology
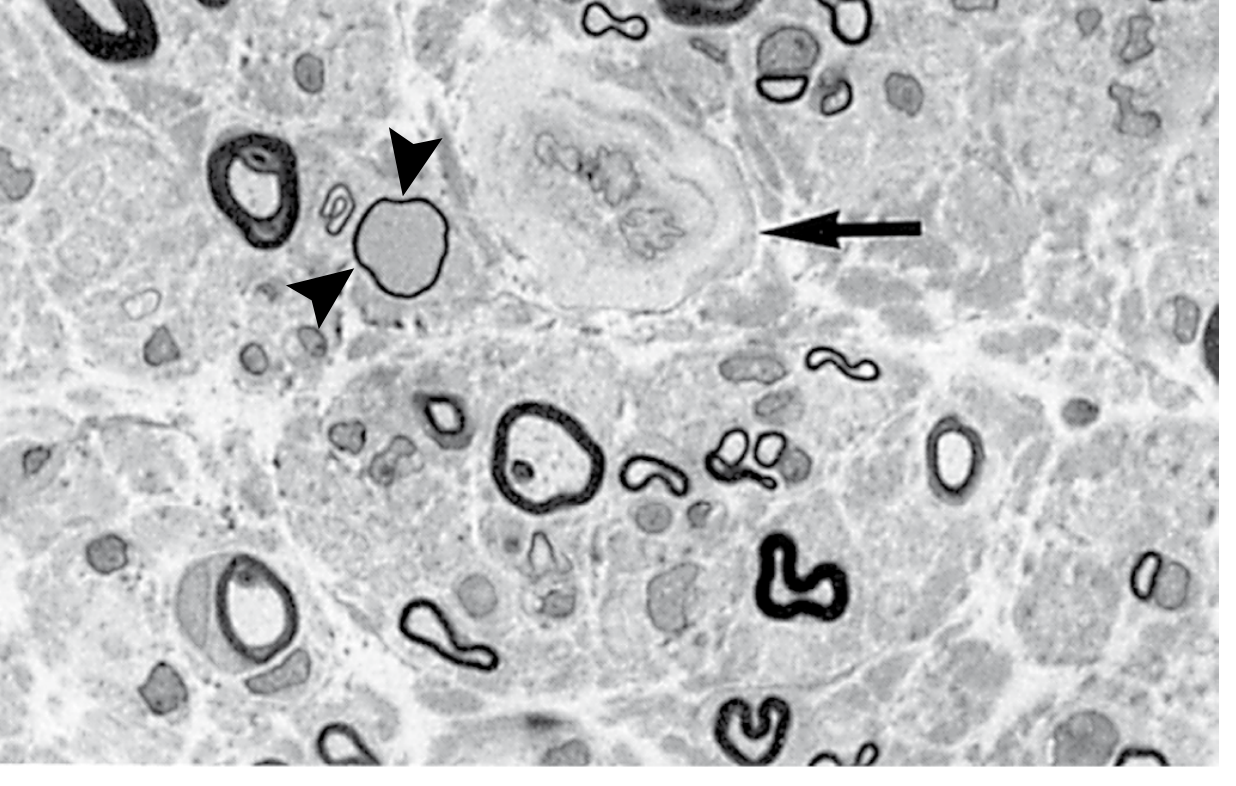
Fig. Diabetic neuropathy - sural nerve biopsy. Note: marked loss of myelinated fibers, thinly myelinated fiber (arrowheads), and endoneurial vessel wall thickening (arrow). - Robbins, Cotran & Kumar Pathologic Basis of Disease
Key histologic findings:
| Finding | Significance |
|---|---|
| Reduced axon density (myelinated and unmyelinated) | Axonal loss - primary pathology |
| Degenerating myelin sheaths | Ongoing axonal damage |
| Regenerative axonal clusters | Attempted (often incomplete) repair |
| Endoneurial arteriole changes | Thickening, hyalinization, PAS-positive walls, reduplicated basement membranes |
| Small fiber (C-fiber) dropout in skin | Correlates with positive/painful symptoms |
| Differential fascicular fiber loss | Pattern of multifocal ischemic damage, not uniform dying-back |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 2454
- Bradley and Daroff's Neurology, p. 961
Large Fiber vs. Small Fiber Involvement
| Fiber Type | Modalities Carried | Clinical Loss | Detected By |
|---|---|---|---|
| Large myelinated (Aβ) | Vibration, proprioception, light touch | Loss of balance, loss of reflexes | NCS, 128 Hz tuning fork, monofilament |
| Small myelinated (Aδ) | Sharp pain, cold temperature | Loss of pain/temperature | Pin-prick, temperature testing |
| Unmyelinated (C fibers) | Burning pain, warm temperature, autonomic | Painful burning (early), then loss | Skin punch biopsy (IENFD), QSART |
- Painless DSPN predominantly affects large fibers
- Painful DSPN shows marked depletion of small myelinated and unmyelinated fibers, with active regeneration generating ectopic discharges
Electrodiagnostics (NCS/EMG)
NCS findings in DSPN:
- Reduced sural nerve amplitude (sensory) - earliest and most sensitive change
- Reduced amplitude in peroneal and tibial motor nerves
- Mild-to-moderate slowing of conduction velocities (reflects secondary demyelination, not primarily a demyelinating process)
- Proximodistal gradient - abnormalities worse distally
- EMG may show mild denervation in intrinsic foot muscles in advanced cases
Note: NCS may be normal in pure small-fiber neuropathy - skin punch biopsy for intraepidermal nerve fiber density (IENFD) is needed in that case.
Diagnosis Screening Protocol
Annual screening for DSPN:
- Type 1 DM: Begin 5 years after diagnosis
- Type 2 DM: Begin at time of diagnosis (neuropathy may precede clinical DM diagnosis)
Screening Tools
| Test | What It Detects |
|---|---|
| 10-g Semmes-Weinstein monofilament | Loss of protective sensation (LOPS) - large fiber |
| 128-Hz tuning fork | Vibration perception - large fiber |
| Pinprick | Small fiber (Aδ) |
| Temperature testing | Small fiber (C fiber) |
| Ankle reflex | Large fiber; one of earliest abnormalities |
Loss of protective sensation (LOPS) = inability to feel 10-g monofilament at the plantar surface. LOPS is the key clinical threshold for foot ulceration risk.
- Harrison's 22E, p. 1647-1648; Washington Manual, p. 4958
Pathogenesis (DSPN-Specific)
The converging mechanisms all ultimately produce endoneurial ischemia and axonal metabolic failure:
Hyperglycemia
│
├──► Polyol pathway ──► Sorbitol/fructose accumulation
│ └──► Myoinositol depletion ──► ↓ Na+/K+-ATPase ──► Axonal dysfunction
│
├──► AGE formation ──► Protein crosslinking + vascular damage
│
├──► PKC activation ──► Endoneurial vasoconstriction ──► Ischemia
│
├──► Oxidative stress (ROS) ──► Direct axonal/Schwann cell injury
│
└──► Endoneurial capillary changes:
- Endothelial hyperplasia
- Basement membrane reduplication
- Luminal narrowing
└──► Nerve hypoxia ──► Axonal atrophy + ↓ NCV
Plus: ↓ NGF, VEGF, erythropoietin (neurotrophic factor deficiency)
The multifocal fascicular pattern of fiber loss (worse distally) is consistent with repeated small ischemic insults from vasa nervorum disease, not a purely metabolic dying-back neuropathy.
- Bradley and Daroff's Neurology, p. 968-974
Treatment (Detailed)
1. Disease Modification
Glycemic control is the only disease-modifying intervention. It reduces risk of developing DSPN and can improve early neuropathy, but has limited effect on established long-standing DSPN. Hypoglycemia unawareness may limit tight control targets in advanced cases.
2. Lifestyle
- Exercise and dietary modification: evidence for benefit in type 2 DM
- Avoid alcohol and smoking (neurotoxins + worsen microvascular disease)
- Check and replace B12 (metformin depletes B12; pernicious anemia more common in type 1 DM)
- Check folate
3. Symptomatic Pain Treatment
First-line options (no single agent is clearly superior - pick based on comorbidities and side-effect profile):
| Drug | Dose | Notes |
|---|---|---|
| Duloxetine (SNRI) | 60-120 mg/day | FDA-approved for diabetic peripheral neuropathic pain; also treats depression |
| Pregabalin | 150-300 mg/day | FDA-approved; also helps anxiety/sleep |
| Gabapentin | 900-3600 mg/day | Off-label but widely used; cheaper than pregabalin |
| Amitriptyline (TCA) | 10-150 mg at bedtime | Effective but anticholinergic side effects; caution in elderly, cardiac disease |
| Venlafaxine / Desvenlafaxine (SNRIs) | Variable | Alternative SNRIs |
| Topical capsaicin 0.075% cream | Applied QID | Burning sensation on application; depletes substance P |
| Capsaicin 8% patch | Single application | Longer-lasting relief |
| Carbamazepine | 100-400 mg PO BID | Sodium channel blocker; monitor for blood dyscrasias |
Not first-line:
- Tapentadol (centrally acting opioid): FDA-approved but modest efficacy + addiction risk
- Opioids: Generally avoid - limited evidence, high addiction risk
Investigational/adjunctive:
-
α-Lipoic acid 600 mg TID: antioxidant; some evidence in early DPN
-
High-dose thiamine (benfotiamine) 50-100 mg TID: tested in early DPN
-
Washington Manual, p. 4965; Harrison's 22E, p. 1673-1674
4. Foot Care (Non-Negotiable)
LOPS dramatically increases the risk of silent foot trauma, pressure ulcers, and Charcot arthropathy. Once a foot ulcer forms in a diabetic:
- Aggressive debridement of necrotic tissue
- Culture-guided systemic antibiotics if infected
- Pressure off-loading (total contact casting, special footwear)
- Revascularization if peripheral arterial disease is present
Prevention:
- Daily self-inspection of feet
- Never walk barefoot (even indoors)
- Avoid heating pads on feet
- Podiatry referral for deformities, extensive callus, or nonhealing ulcers
Key Points to Remember
- Up to 50% of DSPN patients are asymptomatic - screening is essential
- Pain paradoxically diminishes as neuropathy worsens (fibers are destroyed)
- NCS can be normal in pure small-fiber neuropathy - biopsy is gold standard
- Glycemic control is the only disease-modifying treatment - everything else is symptomatic
- LOPS (failure to feel 10-g monofilament) is the critical threshold for foot ulceration risk
- Annual screening: type 1 DM at 5 years, type 2 DM at diagnosis
- The histologic hallmark is axonal loss with endoneurial microvascular disease - NOT primarily demyelination
This is a shared conversation. Sign in to Orris to start your own chat.