Treatment of hydrocephalus
Reading File
Finding Sources
Searching PubMed
"hydrocephalus"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Searching the Web
hydrocephalus treatment guidelines 2024 2025 ETV vs shunt
I now have comprehensive material. Let me compile the full answer.
Treatment of Hydrocephalus
Overview
Hydrocephalus management depends on whether it is obstructive (non-communicating) or communicating, and on the acuity of presentation. Acute obstructive hydrocephalus is a neurosurgical emergency - rapid progression to coma and death ("hydrocephalic attack") can occur without prompt CSF diversion. - Bailey & Love's Short Practice of Surgery, 28th Ed.
1. Emergency / Temporary Measures
External Ventricular Drain (EVD)
The first-line bridge for acute or perioperative hydrocephalus.
- Inserted through a burr hole at Kocher's point (right of midline, anterior to coronal suture), perpendicular to brain surface
- Catheter tip sits at the foramen of Monro in the lateral ventricle
- Can also deliver intrathecal antibiotics
- Lumbar drains are an alternative for communicating hydrocephalus
Treating the Underlying Cause
When an obstructive tumour is resectable, surgery may resolve hydrocephalus directly without permanent CSF diversion.
2. Long-Term Surgical Treatment
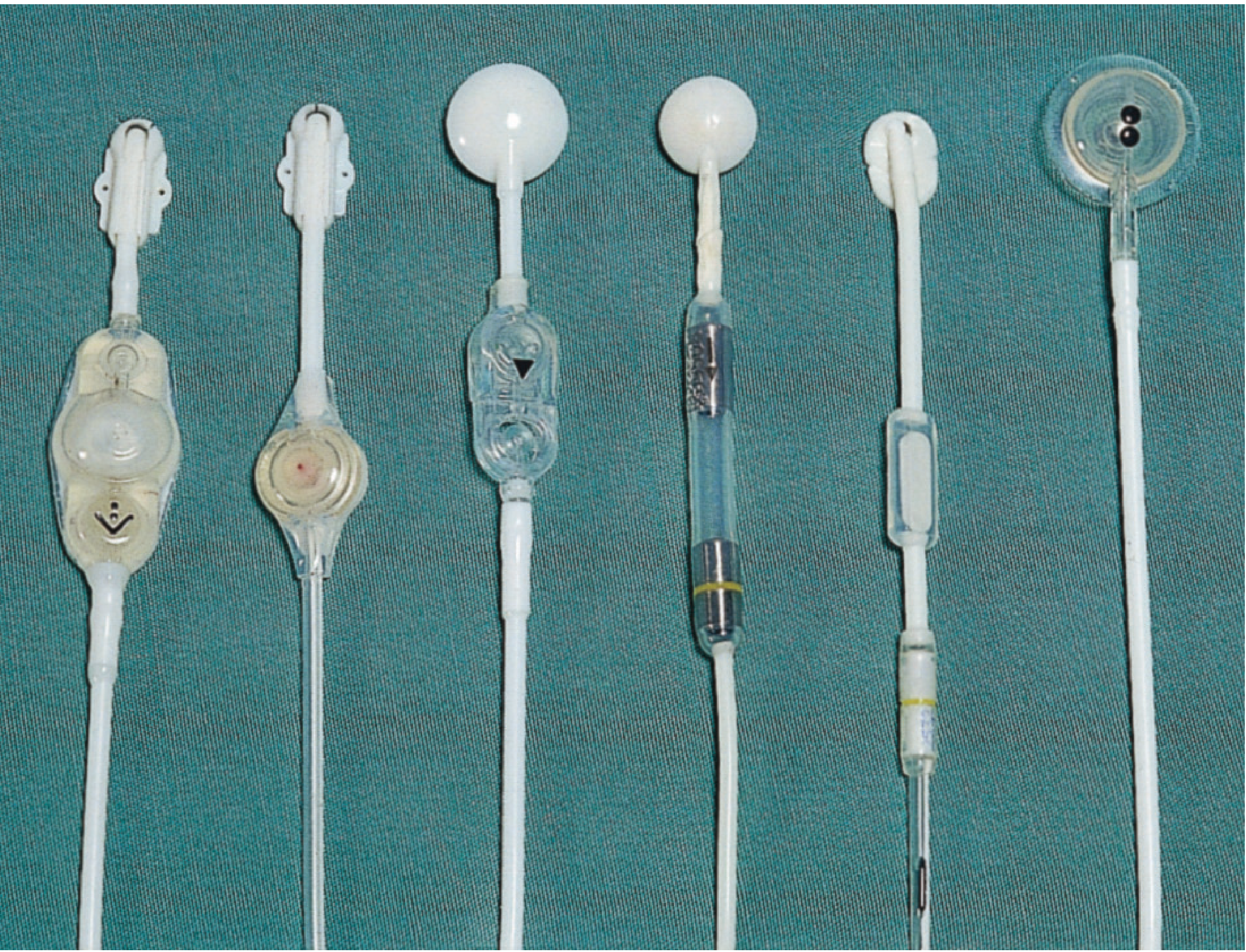
A. Ventriculoperitoneal (VP) Shunt - The Mainstay
The VP shunt is the most widely used definitive treatment. It consists of:
- Proximal (ventricular) catheter - inserted into the lateral ventricle
- Shunt valve - regulates CSF flow by opening at a predetermined pressure; includes a CSF reservoir for percutaneous sampling
- Distal catheter - tunnelled subcutaneously to the peritoneal cavity
Additional features:
- Anti-siphon device - prevents excess drainage in the upright position
- Programmable (adjustable) valves - opening pressure can be changed non-invasively using an external magnetic device
Alternative shunt sites (less common):
| Type | Distal Location | Notes |
|---|---|---|
| Ventriculoatrial (VA) | Right atrium | Rare complications: pulmonary HTN, embolism, VA nephritis (Staph) |
| Ventriculopleural | Pleural space | Risk of pleural effusion |
| Lumboperitoneal | Peritoneum (lumbar) | For communicating hydrocephalus |
B. Endoscopic Third Ventriculostomy (ETV)
Best for: obstructive hydrocephalus due to aqueduct stenosis - avoids indwelling hardware entirely.
Procedure:
- Neuroendoscope inserted into the frontal horn of the lateral ventricle
- Advanced into the third ventricle via the foramen of Monro
- Floor of the third ventricle is fenestrated between the mammillary bodies and the pituitary recess
- Creates free drainage into adjacent subarachnoid cisterns
Advantages: No implanted tubing, no infection risk from hardware
Limitations:
- Re-blockage is common - many patients eventually require a shunt
- Serious rare complications: basilar artery injury, fornix damage causing permanent memory impairment
ETV/CPC (ETV + Choroid Plexus Cauterization): Used particularly in infants under 2 years with non-communicating hydrocephalus (e.g., post-infectious, myelomeningocele-associated). Reduces CSF production by cauterizing the choroid plexus, improving ETV success rates.
ETV vs VP Shunt (current evidence): ETV shows lower infection rates and shunt dependency, especially in patients >1 year with obstructive hydrocephalus. A recent RCT (Surgical Neurology Int.) found ETV success 77% vs VPS 91%, though VPS had more complications overall. The ETV Success Score (ETVSS) helps predict who will benefit.
3. Shunt Complications (15-20% require revision within 3 years)
| Complication | Features | Management |
|---|---|---|
| Infection | Fever, headache, meningism; 75% within 1 month of insertion | Remove shunt + EVD or serial LPs, antibiotics; reinsert shunt at new site when CSF clears |
| Blockage | Symptoms/signs of raised ICP; reservoir hard to compress or slow to refill | Emergency in obstructive hydrocephalus; CT confirms ventricular enlargement; shunt replacement |
| Overdrainage | Postural headaches (worse on standing), subdural hygroma/haematoma | Programmable valve adjustment, anti-siphon device |
| Slit ventricle syndrome | Children; tiny non-compliant ventricles; ICP spikes with coughing/straining | Raise valve opening pressure or add antisiphon device |
| VA-specific | Pulmonary HTN, pulmonary embolism, immune nephritis | Due to chronic Staph colonization |
4. Special Conditions
Normal Pressure Hydrocephalus (NPH)
Classic triad: gait disturbance, urinary incontinence, cognitive decline in elderly patients.
- Treatment of choice: VP shunt - ventricular size often normalises within weeks, gait improves fastest
- Predicting responders is difficult; large-volume LP tap test (improvement in gait after removing ~40 mL CSF) helps select patients
- Acetazolamide has been tried but clinical benefit is minimal
- Goldman-Cecil Medicine, Bradley & Daroff's Neurology
Idiopathic Intracranial Hypertension (IIH / Pseudotumor Cerebri)
No true ventricular enlargement; raised ICP with normal CSF.
- Weight loss (most effective long-term in obese patients)
- Acetazolamide 250-500 mg twice daily, up to 4 g/day - reduces CSF production via carbonic anhydrase inhibition
- Serial lumbar punctures - temporizing measure
- CSF diversion (VP/LP shunt or optic nerve sheath fenestration) - reserved for visual loss or refractory cases
- Bailey & Love; Tintinalli's Emergency Medicine
Post-Hemorrhagic Hydrocephalus (Neonatal/Preterm)
- Early CSF removal may reduce need for VP shunt and attenuate neurodevelopmental impairment
- Guidelines are locale-specific
- Bradley & Daroff's Neurology
Childhood/Infantile Hydrocephalus
- Catheter placed in anterior horn (avoids choroid plexus) to reduce blockage
- Complications unique to children: peritoneal pseudocysts, slit ventricle syndrome, skull growth failure
- Controversial whether to shunt all hydrocephalic infants immediately - outcomes for normal IQ (70-100) in ~72% of shunted children in one series
- Adams & Victor's Principles of Neurology
Summary
| Situation | Preferred Treatment |
|---|---|
| Acute obstructive hydrocephalus | EVD (emergency), then definitive treatment |
| Communicating / long-term | VP shunt (mainstay) |
| Obstructive (aqueduct stenosis, >1 yr) | ETV (first choice to avoid hardware) |
| Infants <2 yr with obstructive | ETV/CPC |
| NPH | VP shunt |
| IIH | Weight loss + acetazolamide; shunt/fenestration for refractory/visual loss |
| Shunt infection | Remove shunt + antibiotics, reinsert when CSF clear |
Sources: Bailey & Love's Short Practice of Surgery 28th Ed. | Adams & Victor's Principles of Neurology 12th Ed. | Bradley & Daroff's Neurology in Clinical Practice | Goldman-Cecil Medicine | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.