Heart block
Reading File
Finding Sources
Searching PubMed
"heart block" OR "atrioventricular block" management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive material from Braunwald's Heart Disease and Symptom to Diagnosis. Let me compile the full response.
Heart Block (Atrioventricular Block)
Heart block is a disturbance of impulse conduction in which atrial impulses are conducted with delay or fail to reach the ventricles when the AV junction is not physiologically refractory. It must be distinguished from interference, which is normal block caused by physiologic refractoriness after a preceding impulse.
Anatomy of Block
Block can occur at the level of:
- The AV node (nodal block) - usually more benign, tends to be congenital
- The bundle of His (intrahisian)
- The bundle branches / Purkinje system (infranodal / trifascicular) - usually acquired, more serious prognosis
Classification
| Degree | AV Conduction | PR Interval | QRS | Clinical Features | Treatment |
|---|---|---|---|---|---|
| 1st degree | 1:1 (all conducted) | >0.20 s, always | Usually normal | Asymptomatic | None |
| 2nd degree - Mobitz I (Wenckebach) | Intermittent | Progressive lengthening until drop | <0.12 s (narrow) | Associated with inferior MI; rarely progresses | Observation or atropine |
| 2nd degree - Mobitz II | Intermittent | Fixed, no change before drop | May be widened, BBB pattern | Associated with anterior MI; often progresses to complete block | Pacemaker |
| High-grade (Advanced) | 2+ consecutive P waves blocked | Variable | Variable | Indistinguishable from 3rd degree clinically | Pacemaker |
| 3rd degree (Complete) | None | No relationship (AV dissociation) | Wide (escape rhythm) | Ventricular rate <40 bpm; syncope, death | Pacemaker |
First-Degree AV Block
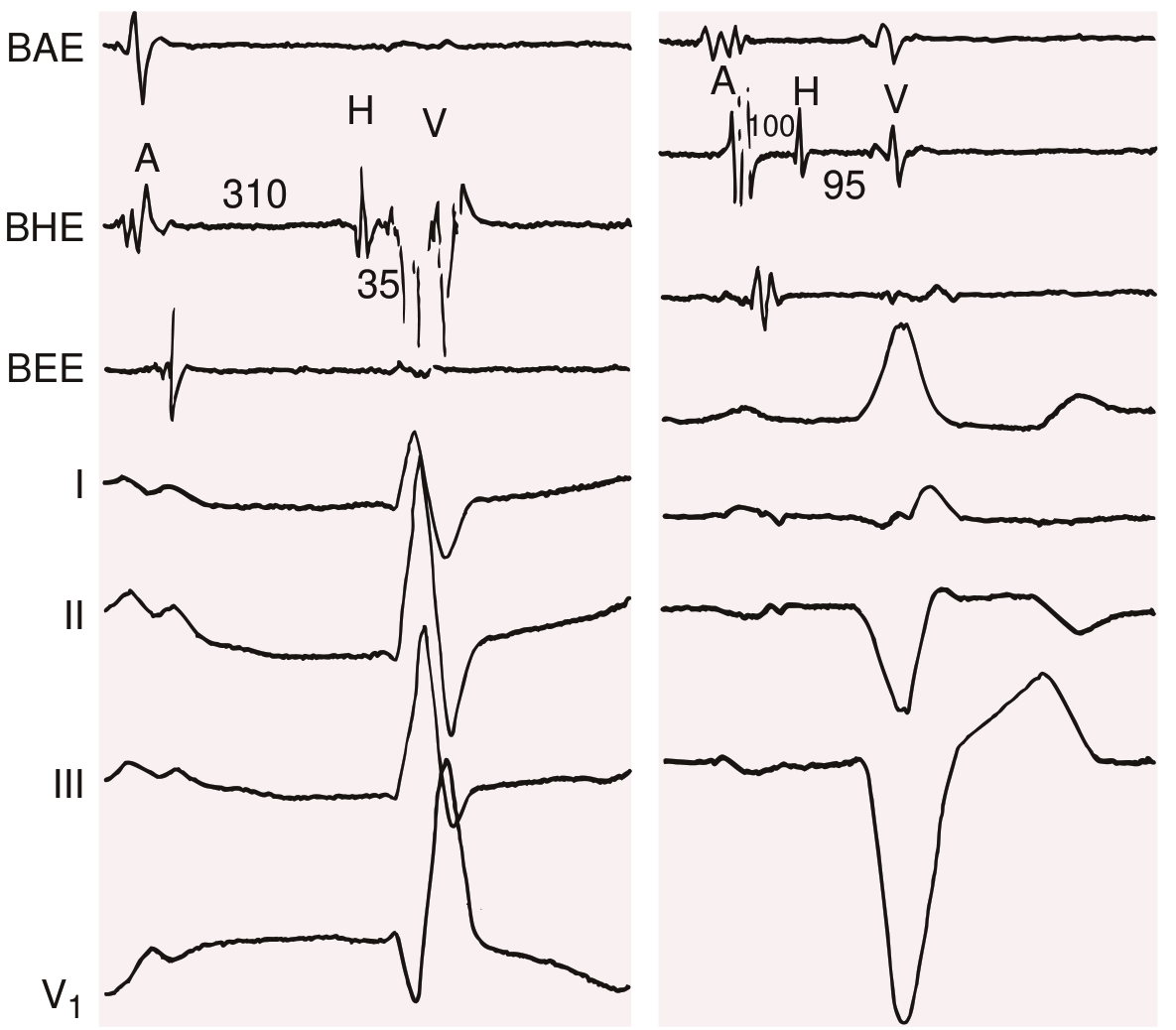
Every atrial impulse reaches the ventricles, but the PR interval exceeds 0.20 s (can reach up to 1.0 s). The delay resides in the AV node if the QRS is narrow; in the His-Purkinje system if a BBB pattern is present (His bundle electrogram needed to localize in that case).
ECG showing first-degree AV block with His bundle recordings (A-H 310 ms left; 100 ms right):
Second-Degree AV Block
Some impulses are blocked. Two subtypes with very different prognoses:
Mobitz Type I (Wenckebach):
- PR interval progressively lengthens until one P wave is dropped
- RR intervals shorten before the dropped beat, then a pause
- Narrow QRS; block is at the AV node
- Often benign; seen with inferior MI, increased vagal tone, medications
Mobitz Type II:
- Sudden unexpected P-wave block without prior PR lengthening
- PR interval is fixed before the dropped beat
- Widened QRS / BBB pattern common (infranodal block)
- High risk of progressing to complete heart block - pacemaker required
2:1 AV Block - special case where you cannot always distinguish Mobitz I from II (need His bundle recordings or look for BBB pattern and QRS width)
High-Grade AV Block
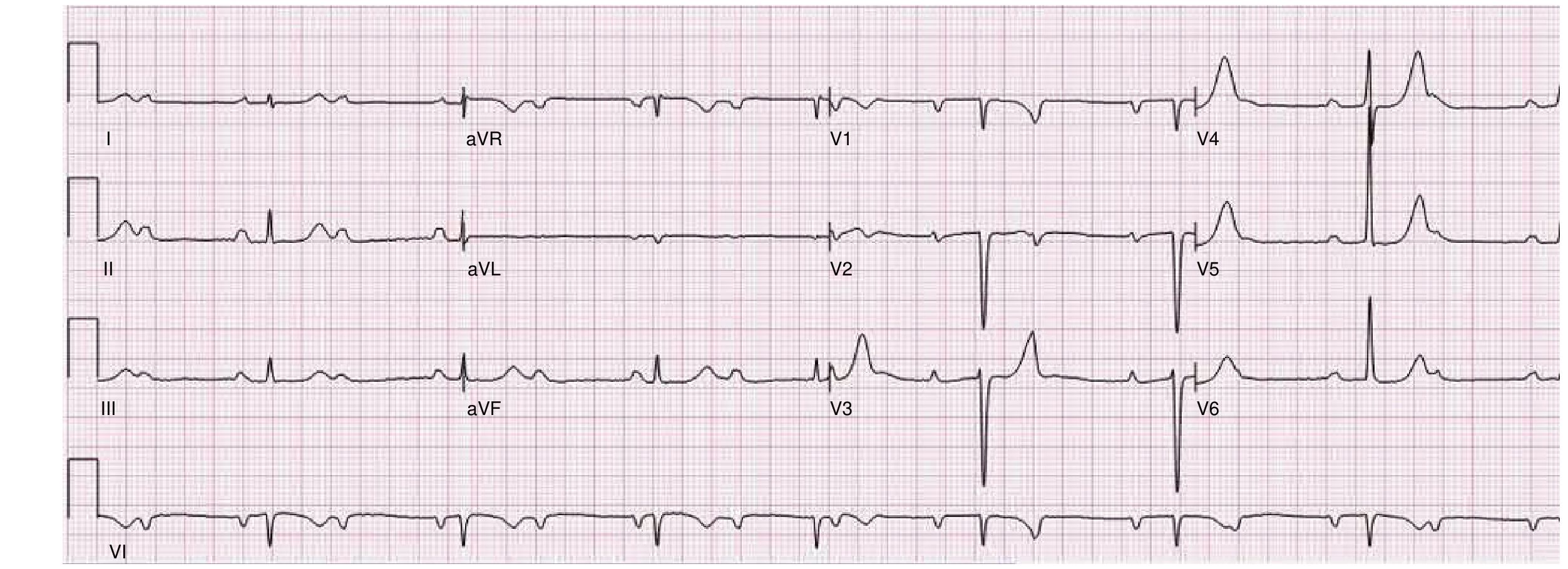
Two or more consecutive non-conducted P waves, with intermittent (not complete) conduction. ECG below shows sinus rate 82 bpm with variable RR intervals confirming intermittent - not complete - block:
Third-Degree (Complete) AV Block
No atrial impulse reaches the ventricles. Atria and ventricles are controlled by independent pacemakers (complete AV dissociation).
- Proximal to His (usually congenital): narrow QRS escape at 40-60 bpm; atropine speeds both atrial and ventricular rates; better prognosis
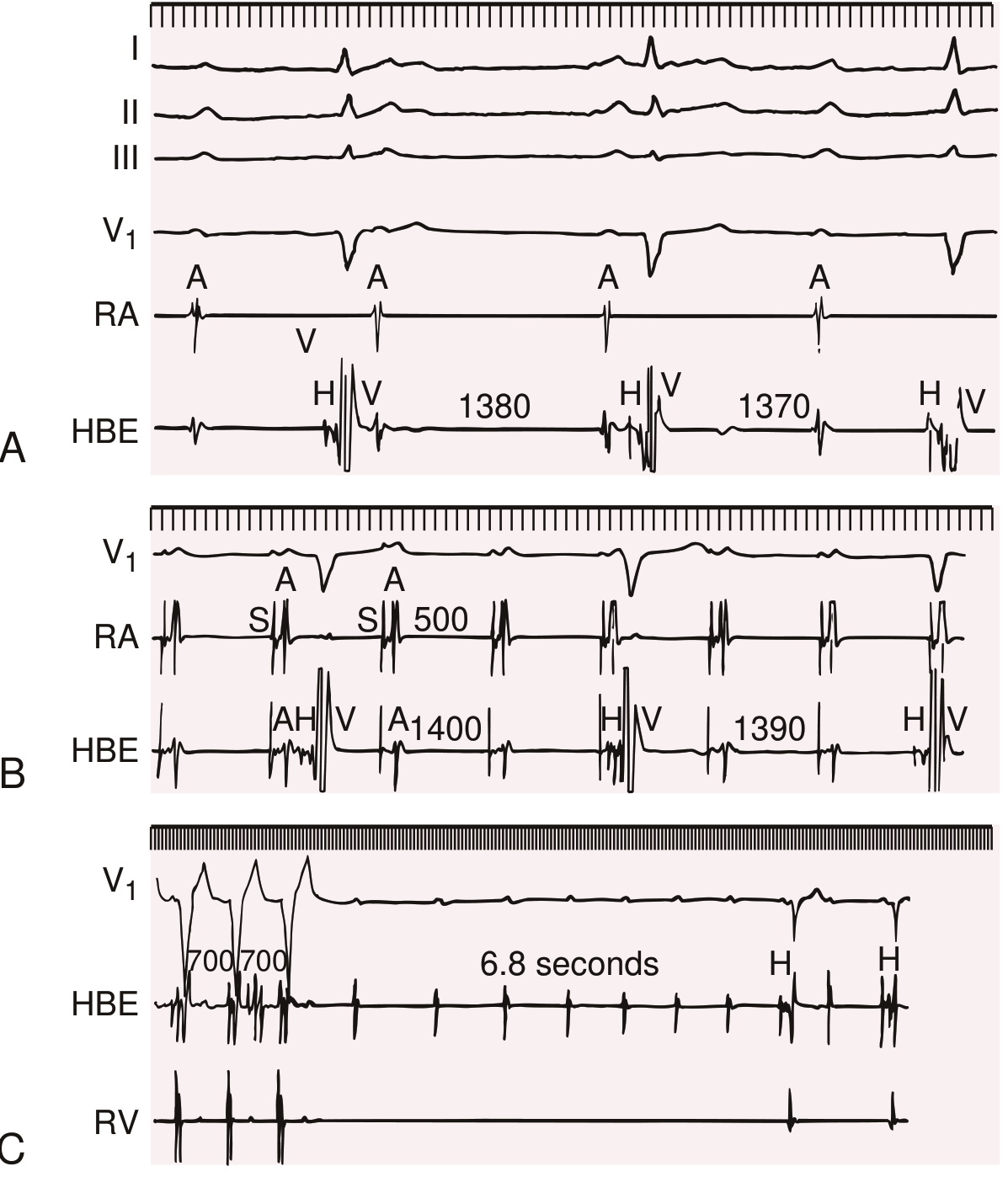
- Distal to His (usually acquired): wide QRS escape at <40 bpm; atropine only speeds atrial rate; each P wave is followed by a His deflection but escape QRS is not preceded by one; requires pacemaker
His bundle recordings in congenital complete AV block - P waves not followed by His deflection; each QRS preceded by His deflection:
Etiology
| Category | Examples |
|---|---|
| Fibrosis/degeneration | Lev disease, Lenègre disease (SCN5A mutation) |
| Ischemia | Inferior MI (AV nodal artery) → Mobitz I; Anterior MI → Mobitz II/complete |
| Medications | Beta-blockers, verapamil, diltiazem, digoxin, adenosine, amiodarone |
| Infiltrative/inflammatory | Sarcoidosis (common cause in <60 y/o), amyloidosis, scleroderma, myocarditis |
| Infectious | Lyme disease, Chagas disease, rheumatic fever |
| Electrolyte | Hyperkalemia |
| Structural | Calcific aortic stenosis extending into the conduction system |
| Congenital | Maternal anti-Ro/SSA antibodies crossing the placenta |
| Procedural | TAVI (transcatheter aortic valve implantation) |
| Autonomic/vagal | Vasovagal syncope, carotid sinus hypersensitivity, inferior MI (Bezold-Jarisch reflex) |
Key note: Sarcoidosis accounts for ~34% of unexplained 2nd/3rd-degree AV block in patients under 60 - consider it even without a prior diagnosis. Of such patients, 27% subsequently develop VT or heart failure. - Symptom to Diagnosis, 4th Ed.
Most patients with AV block attributed to verapamil, diltiazem, or beta-blockers also have underlying conduction disease - >80% experience AV block even when off these medications.
Clinical Presentation
Symptoms correlate with ventricular rate and degree of block:
- First-degree: asymptomatic
- Second-degree (Mobitz I): often asymptomatic; palpitations
- Mobitz II / Complete block: syncope, pre-syncope, dizziness, dyspnea, angina, hypotension, sudden cardiac death
- Atrial fibrillation with slow ventricular response (not on AV-nodal drugs) - suspect AV nodal disease
Physical exam clues:
- Variable intensity of S1 (as PR interval changes)
- Cannon a waves in the jugular venous pulse (atria contracting against closed tricuspid valve)
- Bruit de canon - intense S1 followed by sudden reduction in intensity as P waves "march through" the cycle
ECG Diagnosis
Pacemaker indications require documentation of one of:
- Third-degree AV block
- Advanced second-degree AV block (≥2 consecutive blocked P waves) plus any of:
- Symptoms
- Ventricular arrhythmias secondary to AV block
- Asystole ≥3 seconds, escape rate <40 bpm, or escape rhythm below AV node
- AF with pauses ≥5 seconds
- Symptomatic second-degree AV block (any type)
- Unexplained syncope with chronic bifascicular block (especially HV interval ≥70 ms on EPS)
Treatment
| Situation | Approach |
|---|---|
| Acute/emergent | Atropine (0.5-1 mg IV); transcutaneous pacing; dopamine/epinephrine infusion |
| Reversible cause | Stop offending medications; treat ischemia; correct electrolytes |
| Permanent pacemaker | Third-degree block, advanced 2nd-degree, symptomatic 2nd-degree, bifascicular block with syncope |
| First-degree / asymptomatic Mobitz I | Observation; treat underlying cause |
For complete AV block: permanent pacemaker is the definitive treatment. Dual-chamber pacing (DDD) is generally preferred to maintain AV synchrony.
AV Block vs. AV Dissociation
These are related but not synonymous:
- Complete AV block always causes complete AV dissociation
- Complete AV dissociation does NOT always mean complete AV block (can result from accelerated junctional rhythm, VT, or interference)
- AV dissociation is a finding, not a diagnosis - always identify the cause
Sources: Braunwald's Heart Disease, 12th Ed., Ch. 68; Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed., Ch. 31; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.