I now have comprehensive content from all three major surgery textbooks. Let me compile the complete, detailed answer.
Fissure-in-Ano: A Comprehensive Surgical Account
(Sources: Bailey & Love's Short Practice of Surgery 28e, Sabiston Textbook of Surgery, Schwartz's Principles of Surgery 11e)
1. Definition
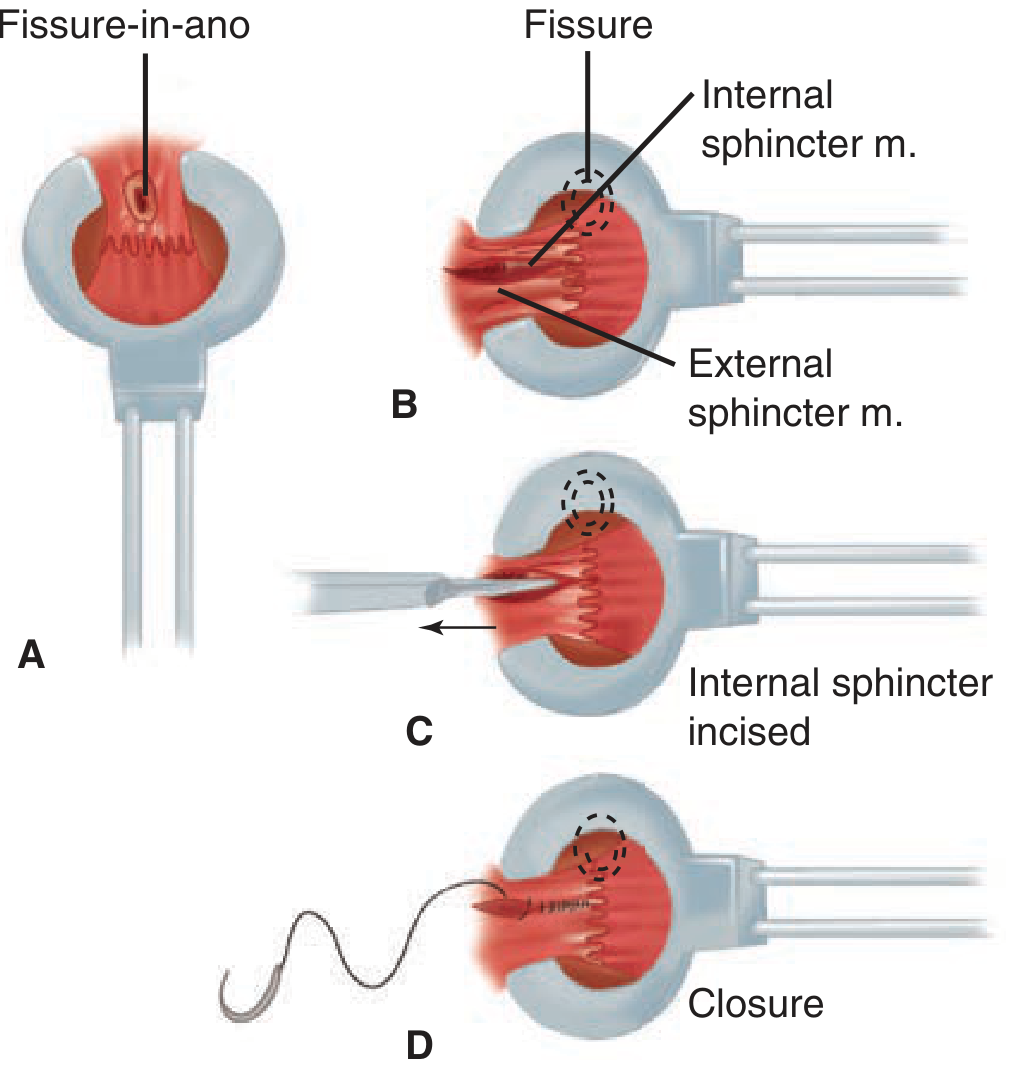
An anal fissure (fissure-in-ano) is a longitudinal ulcer (elliptical or oval-shaped tear) in the anoderm of the distal anal canal. It extends from the anal verge proximally toward - but not beyond - the dentate line. Acute fissures appear as a shallow tear; chronic fissures develop ulceration, heaped-up edges, and visible internal anal sphincter (IAS) fibers at the base.
"An anal fissure is an elliptical or oval-shaped tear in the anal canal starting at the anal verge and extending proximally for a varying length toward the dentate line." - Sabiston Textbook of Surgery
2. Aetiology and Pathophysiology
The underlying mechanism is a vicious cycle of pain - spasm - ischaemia:
- Initiating trauma - passage of hard stool (constipation), prolonged diarrhea, anal receptive intercourse, or childbirth tears the anoderm.
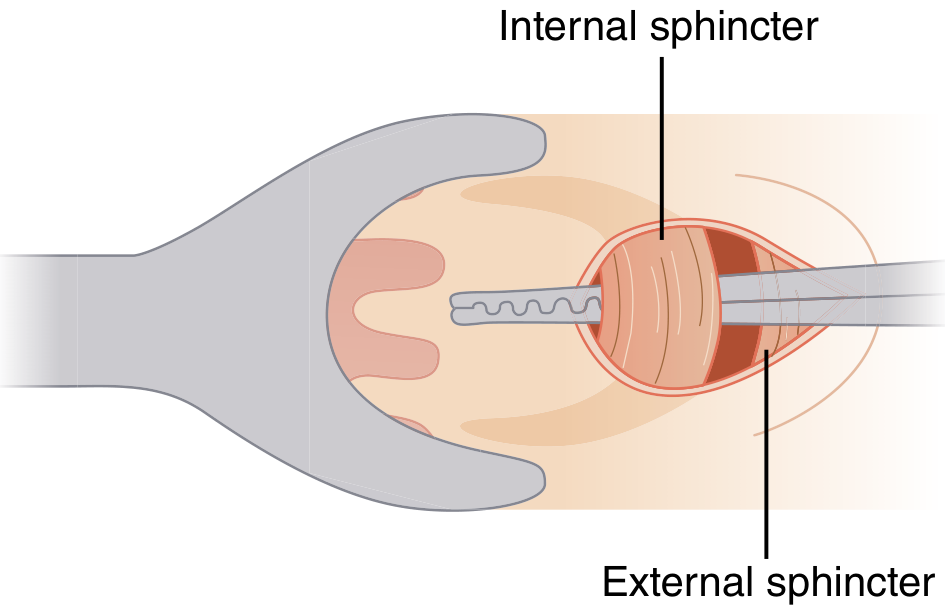
- IAS hypertonia - the pain from the tear causes reflex spasm of the internal anal sphincter, which is involuntary smooth muscle.
- Ischaemia - the hypertonic IAS decreases blood supply to the posterior midline anoderm, creating relative tissue ischaemia.
- Non-healing - ischaemia prevents wound healing; further defecation re-tears the fissure, perpetuating the cycle.
Why the posterior midline?
- 75% of fissures occur here. The posterior midline has a relatively less robust blood supply compared to other quadrants.
- Shearing forces during defecation are maximal at the posterior midline.
- The anoderm here is less elastic and has an increased density of longitudinal muscle extensions.
- Anterior fissures (10-15%) are more common in women, often following vaginal delivery.
- Less than 1% occur off the midline - these must raise suspicion of a secondary cause.
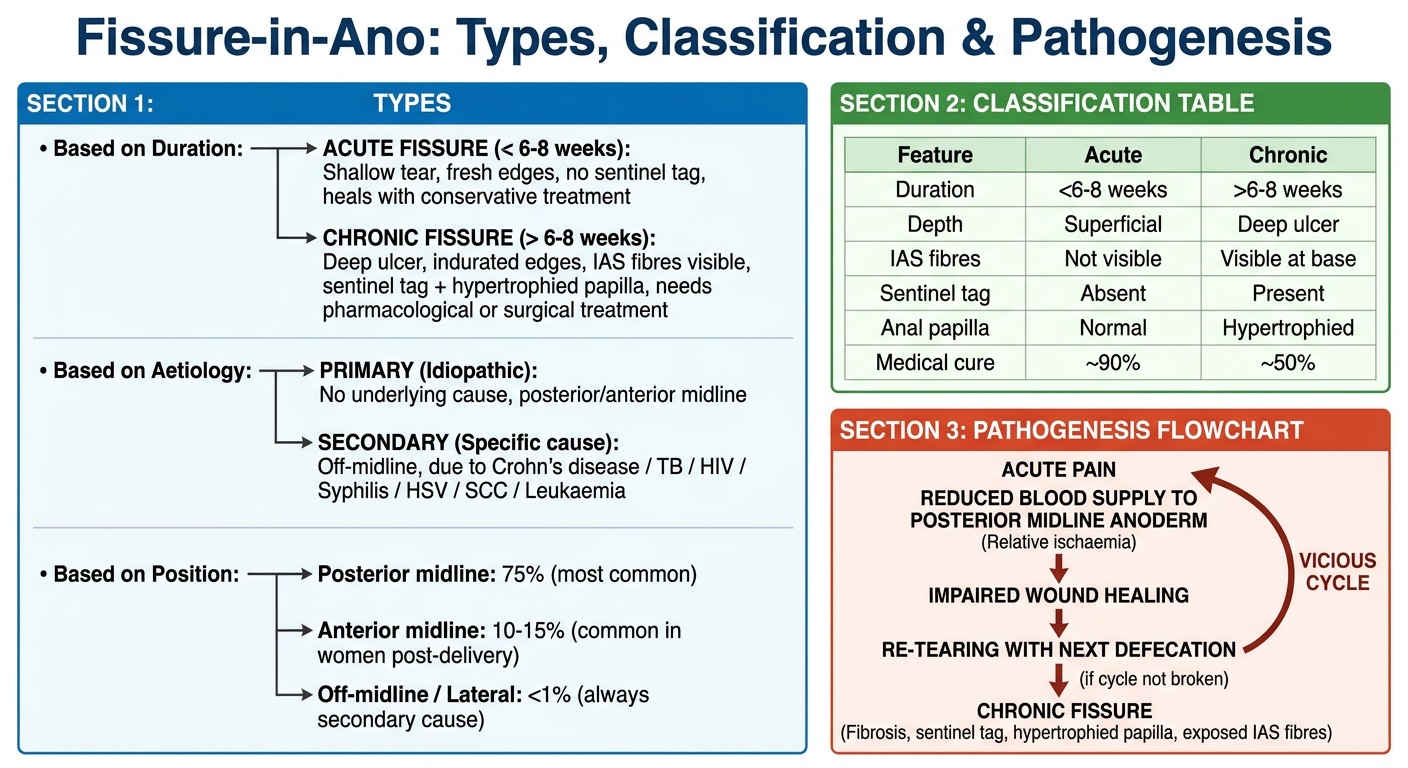
3. Classification
| Feature | Acute Fissure | Chronic Fissure |
|---|
| Duration | < 6-8 weeks | > 6-8 weeks |
| Appearance | Shallow tear, fresh | Deep ulcer, indurated edges, IAS fibers visible at base |
| Sentinel tag | Absent | Present externally |
| Hypertrophied papilla | Absent | Present internally (at dentate line) |
| Associated fistula | Absent | May have intersphincteric fistula |
| Response to medical Rx | Almost always heals | ~50% healing with medical therapy |
4. Clinical Features
Symptoms:
- Severe anal pain during defecation - classically described as "passing pieces of glass" or "razor blades" or "a knife cutting." The pain typically resolves then recurs with the next bowel movement.
- Throbbing and anal spasm - can persist for minutes to hours after defecation.
- Bright-red bleeding - usually a trace on toilet paper; rarely more than that.
- Pruritus ani - from irritation by the sentinel tag or discharge.
- Mucus discharge - from the ulcer or an associated intersphincteric fistula.
- In severe chronic cases, patients may avoid oral intake (and lose weight) due to dread of defecation.
Signs:
- The fissure is often visible by gently separating the buttocks - examine in this gentle manner first.
- Chronic fissure triad:
- Sentinel skin tag/pile externally (at the anal verge)
- Indurated ulcer with visible IAS fibers at the base
- Hypertrophied anal papilla proximally (at dentate line)
- Digital rectal examination, anoscopy, and proctoscopy are often deferred because even gentle palpation reproduces intolerable pain.
- If the fissure is not clearly visible, focal pressure with a fingertip or cotton-tip applicator at the posterior or anterior anal canal reproduces pain.
5. Atypical / Secondary Fissures
A fissure that is off the midline or has atypical features must raise suspicion of an underlying cause. A lateral anal fissure or one that fails to heal is an indication for examination under anaesthesia (EUA) with biopsy and culture to exclude:
- Crohn's disease
- Tuberculosis
- HIV-related ulcers
- Syphilis, Chlamydia, chancroid, lymphogranuloma venereum (LGV)
- Herpes simplex virus (HSV), Cytomegalovirus (CMV)
- Kaposi's sarcoma, B-cell lymphoma
- Squamous cell carcinoma (SCC)
- Leukaemia
6. Treatment
Treatment is stepwise, aimed at breaking the cycle of pain - spasm - ischaemia.
6.1 Conservative (First-Line for All Fissures)
- Increased fibre and fluid intake - bulk-forming agents to produce soft, formed stools.
- Stool softeners - to minimise anal trauma.
- Warm sitz baths - demonstrated to provide significant pain relief in >90% of patients with acute fissures.
- Topical local anaesthetics (e.g., 2% lidocaine jelly) - additional symptomatic relief.
- Anorectal biofeedback - for patients with normal bowel habits but excessive straining.
These conservative measures heal almost all acute fissures and the majority of chronic fissures.
6.2 Chemical Sphincterotomy (Pharmacological Relaxation of IAS)
When simple measures fail, "chemical sphincterotomy" is employed using agents that relax the smooth muscle of the IAS.
a) Topical Glyceryl Trinitrate (GTN) / Nitroglycerin
- A nitric oxide donor that causes smooth muscle relaxation and vasodilation.
- 0.2% ointment, applied 2-3 times per day to the anal margin.
- Healing rate: approximately 50% of chronic fissures.
- Major side effect: severe headaches - limits acceptability; patients stop therapy in up to 20%.
b) Topical Calcium Channel Blockers
- Diltiazem 2% (applied twice daily) or nifedipine - relax the IAS and promote vasodilation.
- Healing rates similar to GTN for chronic fissures.
- Significantly better side-effect profile - fewer headaches - making these the preferred first-line topical agents (Sabiston).
- Note: No readily available commercial formulation in some countries; must be obtained from compounding pharmacies.
c) Botulinum Toxin (Botox) Injection
- Causes temporary muscle paralysis by preventing acetylcholine release from presynaptic nerve terminals.
- Dose: 20-100 IU (10-100 units) injected into the IAS in a single or divided dose.
- Produces IAS relaxation lasting approximately 3 months.
- Can be done in-office or as an outpatient procedure with sedation.
- Healing rate: ~50% (similar to topical therapies as first-line; modest improvement as second-line after failed topical therapy).
- Side effects: temporary incontinence to flatus (up to 10%); rarely - increased urinary residual volume, heart block.
- Used as an alternative to surgical sphincterotomy at some centres.
6.3 Surgical Treatment (For Chronic Fissures Failing Medical Therapy)
A. Lateral Internal Sphincterotomy (LIS) - Procedure of Choice
LIS is the gold standard surgical treatment for chronic anal fissure. The aim is to decrease IAS spasm by dividing a portion of the internal sphincter laterally (away from the fissure, usually at the 3 or 9 o'clock position), thereby reducing resting anal canal pressure and improving blood flow to the posterior midline.
Why lateral? - To avoid iatrogenic defects in the already-ulcerated posterior midline, and to reduce keyhole deformity.
Extent of division: Approximately 30% (the distal third) of the IAS fibers are divided, to the level of the apex of the fissure - dividing too much increases incontinence risk; too little fails to heal the fissure.
Technique - Two approaches, with equivalent results:
1. Open Lateral Internal Sphincterotomy
- A radial incision is made in the anoderm at the lateral position (3 or 9 o'clock), exposing the distal IAS muscle fibers.
- The distal segment of the IAS is divided sharply for a length corresponding to the length of the fissure.
- The wound can be left open or closed primarily with absorbable sutures.
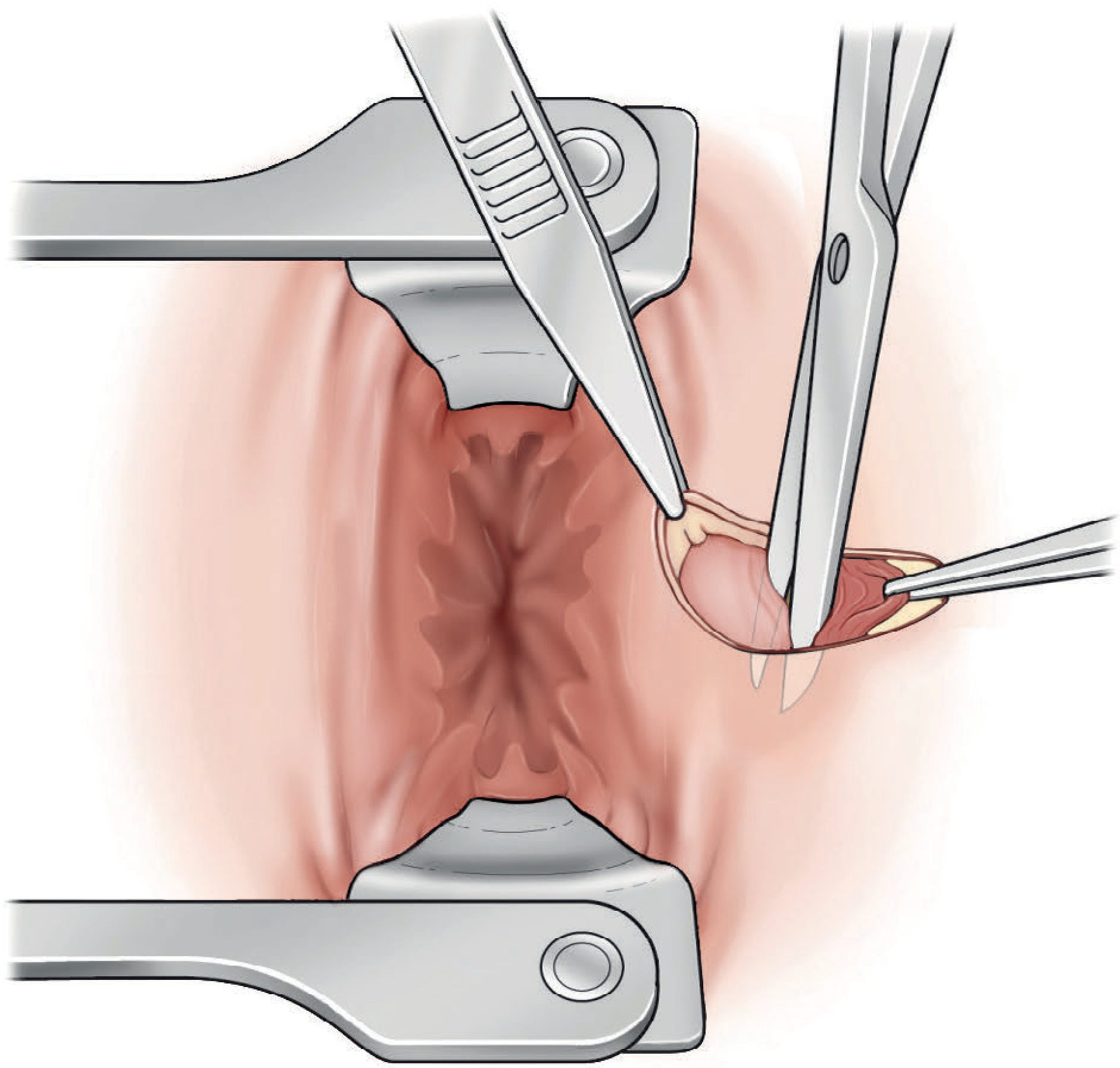
2. Closed Lateral Internal Sphincterotomy
- The distal IAS is palpated with a bivalved speculum at the intersphincteric groove.
- A small no. 11 blade scalpel is inserted directly into the intersphincteric groove, advanced parallel to the sphincter.
- The blade is then rotated so its sharp edge faces the IAS, dividing the distal third laterally.
- Alternatively, dissecting scissors open the intersphincteric space and divide the IAS:
- Pressure is applied to the wound for a few minutes to prevent haematoma formation.
- Wound is closed with absorbable sutures.
Position: Lithotomy or prone jack-knife. Anaesthesia: Local, regional, or general.
Outcomes of LIS:
| Outcome | Rate |
|---|
| Healing rate | 85-95% (Sabiston: 88-100%) |
| Recurrence | < 10% |
| Immediate pain relief | Most patients |
| Flatus incontinence | 5-15% (Bailey & Love: 9%) |
| Soiling | ~6% |
| Solid stool incontinence | <1% |
Early complications: Haemorrhage, haematoma, bruising, perianal abscess, fistula.
Patients at higher risk for post-LIS incontinence (in whom LIS should be avoided or used cautiously):
- Baseline incontinence
- Females with prior obstetric injuries
- Previous anorectal operations
- Documented anal sphincter injury
B. Anal Sphincter Dilatation (Lord's Procedure)
- Forcible dilatation of the anal canal (manually) to reduce sphincter tone.
- Largely abandoned - disrupts the anal sphincters at multiple unpredictable sites with an unacceptably high risk of incontinence.
- Rarely indicated in current practice.
C. Fissurectomy
- Surgical excision of the fibrotic edges of the fissure, curettage of the base, and excision of the sentinel tag and/or anal papilla.
- Used as an alternative to LIS when there are contraindications to sphincterotomy.
- Frequently combined with an anal advancement flap anoplasty.
D. Anal Advancement Flap Anoplasty
- Should be considered in patients with increased risk of altered continence after LIS - especially postpartum women and those with normal or low resting anal pressures.
- After fissurectomy, an inverted house-shaped flap of perianal skin is carefully mobilised on its blood supply and advanced to cover the fissure.
- VY advancement flaps with or without sphincterotomy have also been reported to successfully treat chronic fissures (Schwartz's).
7. Management Algorithm Summary
Anal Fissure Diagnosed
|
Acute (<6-8 wks) Chronic (>6-8 wks)
| |
Conservative Rx Conservative + Chemical
(Fibre, sitz baths, Sphincterotomy
stool softeners) (GTN/CCB topically →
| Botox if fails)
Healed ✓ |
Fails (~50%)
|
Off-midline? → EUA + Biopsy
Midline → Lateral Internal
Sphincterotomy
High incontinence risk →
Advancement Flap
8. Key Points to Remember (Surgical Summary)
- Location: 75% posterior midline; 10-15% anterior (more common in women); <1% lateral (always secondary cause).
- Pathophysiology: Tear → IAS spasm → ischaemia → non-healing (vicious cycle).
- Triad of chronic fissure: Sentinel tag + ulcer with IAS fibers exposed + hypertrophied anal papilla.
- First-line medical: Topical CCBs (diltiazem) preferred over GTN due to fewer headaches.
- Botox: Office procedure, 3-month effect, 50% healing, 10% temporary incontinence.
- Surgery of choice: Lateral internal sphincterotomy - divides distal 1/3 of IAS laterally.
- Open vs Closed LIS: Equivalent results; both heal 85-95%.
- Risk of LIS: Flatus incontinence 5-15%; warn all patients preoperatively.
- Advancement flap: Alternative for patients at high incontinence risk.
Bailey and Love's Short Practice of Surgery 28e, pp. 1449-1450 | Sabiston Textbook of Surgery (9780443124341), pp. 2159-2160 | Schwartz's Principles of Surgery 11e, pp. 1339-1341