Z effect in Proximal femoral nail
"Z effect" proximal femoral nail intertrochanteric fracture
"Z effect" "proximal femoral nail" screw migration
PMID: 25983456
Z effect reverse Z effect proximal femoral nail intertrochanteric fracture mechanism prevention
Z effect proximal femoral nail lateral migration lag screw medial migration anti-rotation screw mechanism treatment
Z effect reverse Z effect proximal femoral nail screw migration diagram
Z Effect in Proximal Femoral Nail (PFN)
Background
Z Effect
| Feature | Detail |
|---|---|
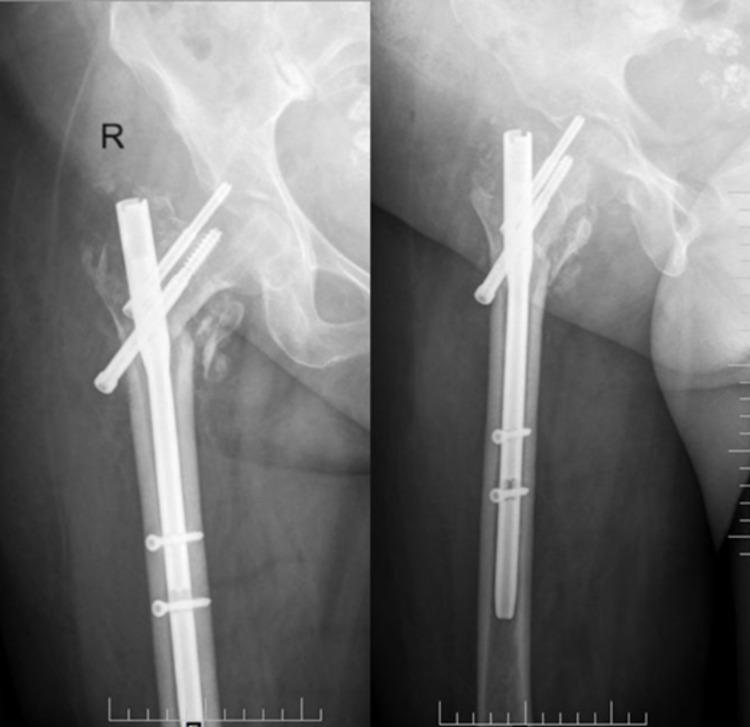
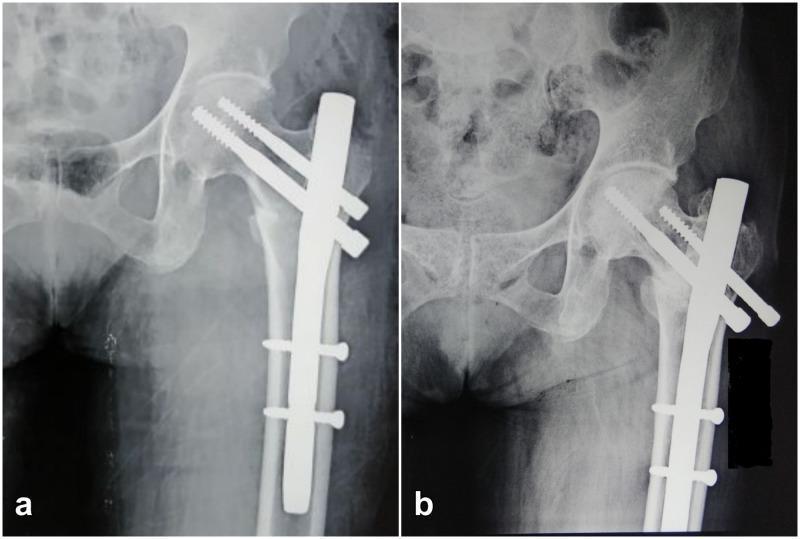
| Definition | Differential migration of the two screws in opposite directions, forming a "Z" pattern on X-ray |
| Inferior lag screw | Migrates laterally (backs out through the lateral cortex) |
| Superior anti-rotation screw | Migrates medially (cuts into / through the femoral head, risking acetabular penetration) |
| Pattern on X-ray | Resembles the letter Z |
- The fracture undergoes varus collapse and the proximal fragment tilts
- With cyclic loading, the inferior lag screw (which can slide freely within the nail) migrates laterally because it has poor bony purchase in the neck
- This transfers all load to the superior locked anti-rotation screw, which is forced medially through the femoral head
- Ultimately, the superior screw can cut out medially into the acetabulum — catastrophic failure
Reverse Z Effect
| Feature | Detail |
|---|---|
| Superior anti-rotation screw | Migrates laterally (backs out) |
| Inferior lag screw | Migrates medially (penetrates femoral head, risks intrapelvic migration) |
| Pattern on X-ray | Resembles a reverse Z |
Radiographic Appearances
Summary Table
| Z Effect | Reverse Z Effect | |
|---|---|---|
| Inferior screw | → Lateral migration (backs out) | → Medial migration (cuts in) |
| Superior screw | → Medial migration (cuts in) | → Lateral migration (backs out) |
| X-ray pattern | Z shape | Reverse Z shape |
| Dangerous consequence | Superior screw → acetabular penetration | Inferior screw → intrapelvic migration |
Risk Factors
- Unstable intertrochanteric fractures (reverse oblique, comminuted, lack of medial cortical support)
- Poor bone quality / osteoporosis
- Inadequate fracture reduction before nailing
- Nail toggling within the femoral canal (toggling = nail not snugly seated)
- Lack of bony purchase in the femoral neck for the inferior lag screw
- High tip-apex distance (TAD > 25 mm)
Prevention
- Adequate fracture reduction before nail insertion — restoring medial cortical support minimizes toggle
- Proper screw placement — center-center position in the femoral head, TAD < 25 mm
- Use of single-screw designs (e.g., PFN-A with a helical blade, or PFNA) — eliminates the two-screw differential migration problem entirely; the blade provides rotational stability without a second screw
- Ensure inferior screw has good bony purchase in the femoral neck
- Use of long nails for fractures with distal extension to minimize nail toggling
Treatment
| Severity | Management |
|---|---|
| Asymptomatic / minimal symptoms | Conservative observation if fracture healing is progressing |
| Symptomatic hardware prominence (lateral back-out) | Remove the backed-out screw |
| Medial screw cut-out into acetabulum | Urgent revision — implant removal + arthroplasty (hemi or THA) |
| Intrapelvic screw migration | Surgical extraction ± vascular surgery backup; conversion to arthroplasty |
Clinical Significance
Proximal femoral bionic nail
proximal femoral bionic nail design features biomechanics intertrochanteric fracture
"proximal femoral bionic nail" intertrochanteric fracture
PMID: 36719445
PMID: 40783984
PMID: 41163169
proximal femoral bionic nail PFBN design trochanteric support screw N-triangle theory components technique
PFBN proximal femoral bionic nail components intramedullary nail trochanteric screw cephalocervical screw triangular support surgical technique
PMID: 38938983
proximal femoral bionic nail PFBN design diagram X-ray
PFBN "bionic nail" "trochanteric support screw" OR "lateral support screw" Ward triangle N-triangle Zhang intertrochanteric fracture advantages disadvantages
Proximal Femoral Bionic Nail (PFBN)
Background & Concept
Theoretical Basis — Zhang's N-Triangle Theory
- Ward's triangle identifies the area of least bone density in the femoral neck, bounded by tensile and compressive trabecular systems
- Zhang's N-triangle theory extends this by proposing that internal fixation of the proximal femur must simultaneously address both tensile and compressive stress trajectories to restore physiological load balance
- Multiple overlapping stable triangular areas are formed by the fixation construct, mimicking the natural trabecular architecture — hence the term "bionic"
- The theory also addresses the lever arm problem: in conventional nails, the lever point of the construct is far from the anatomical fulcrum, increasing the moment arm and shear stress at the fracture. The PFBN's triangular support structure reconstructs the lever point closer to the anatomical support point, shortening the moment arm
Design & Components
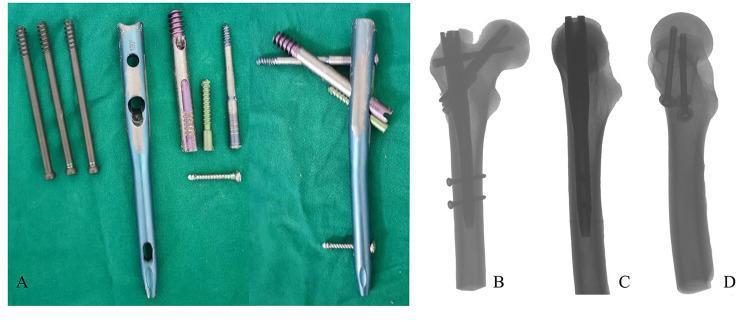
| Component | Description |
|---|---|
| Intramedullary nail (main nail) | Standard femoral canal nail with 3 proximal screw holes |
| Traction/fixation screw (cephalocervical lag screw) | Passes into the femoral head along the neck axis; has a central hole through which the support screw passes |
| Trochanteric/lateral support screw | Passes through the nail and through the hole in the traction screw, then anchors into the greater trochanter / lateral cortex, forming a cross-intersection |
- PFN — two parallel screws (prone to Z effect)
- PFNA — single helical blade (no cross-support)
- InterTAN — two interlocking screws but no trochanteric lateral support arm
Biomechanical Advantages
- Triangular support structure — the cross-screw design forms stable triangular fixation areas, distributing both compressive and tensile loads along the trabecular lines
- Reduced stress concentration — FEA studies show 9.36%–59.32% reduction in maximum von Mises stress at the implant compared to PFNA, InterTAN, and Gamma nail (PMID 38938983)
- Greater trochanter anchoring — the lateral support screw locks into the greater trochanter, providing a lateral buttress against varus collapse
- Shorter effective moment arm — the construct's lever point is closer to the anatomical fulcrum of the hip joint
- No Z effect — the cross-locked screw design prevents differential independent migration of the two screws (unlike classic PFN)
- Improved fracture interface stability — FEA shows lower fracture interface displacement (0.21 mm) vs PFNA (0.24 mm) and DHS+DS (0.25 mm)
Indications
- Unstable intertrochanteric fractures (AO/OTA 31-A2 and 31-A3)
- Reverse obliquity intertrochanteric fractures (31-A3) — where conventional nails perform poorly
- Subtrochanteric fractures — biomechanical studies support its use
- Basicervical femoral neck fractures — finite element analysis demonstrates superiority (PMID 38053203)
- Particularly suited to elderly, osteoporotic bone where implant failure rates are high
Clinical Evidence
Meta-Analyses (2025)
| Outcome | PFBN | PFNA | Significance |
|---|---|---|---|
| Fracture healing time | Shorter | Reference | p < 0.01 |
| Time to weight-bearing | Earlier (–13.5 days) | Reference | p < 0.01 |
| Harris Hip Score | Higher (+0.93 pts) | Reference | p < 0.05 |
| Operative time | Longer (+6 min) | Reference | p < 0.01 |
| Intraoperative blood loss | More (+9.6 mL) | Reference | p < 0.01 |
| Complication rate | No significant difference | — | NS |
- PFBN: significantly shorter fracture healing time and earlier weight-bearing vs both comparators
- PFBN: longer surgery duration than PFNA (no difference vs InterTAN)
- No significant difference in blood loss, hospital stay, Harris Hip Score, or complication rates
- GRADE: moderate to high certainty evidence
Original Clinical Study
- Mean op time: 90 min (A2: 83 min, A3: 105 min)
- Harris Hip Score at 12 months: 82.6 ± 4.6
- No major implant failures reported
Advantages vs Conventional Nails
| Feature | PFBN | PFNA | PFN | InterTAN |
|---|---|---|---|---|
| Z effect risk | None | None | High | Low |
| Rotational control | Cross-screw | Blade compaction | Derotation screw | Interlocking screws |
| Lateral trochanteric support | Yes | No | No | No |
| Fracture healing time | Faster | Reference | — | Similar |
| Operative time | Longer | Shorter | — | Similar |
| Biomechanical stability (FEA) | Superior | Reference | — | Similar/inferior |
| Established clinical track record | Limited (recent) | Extensive | Established | Established |
Limitations & Disadvantages
- Longer operative time — the cross-screw assembly is technically more demanding
- Slightly more blood loss intraoperatively vs PFNA
- Relatively new implant — limited long-term follow-up data; most studies are retrospective, single-centre, from China
- Learning curve — assembly of the interlocking cross-screw mechanism is unfamiliar to most surgeons trained on PFNA
- Limited availability outside China currently