Heart physiology and cardiac cycle and heart sound and murmur how produce detail explanation
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
cardiac cycle pressure volume heart sounds Wiggers diagram
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from Guyton & Hall and Costanzo Physiology to write a thorough, well-structured response. Let me compose the answer.
Heart Physiology, Cardiac Cycle, Heart Sounds & Murmurs
1. Heart Physiology Overview
The heart is a muscular pump divided into four chambers: right atrium, right ventricle, left atrium, left ventricle. Its primary function is to maintain two separate circulations:
- Pulmonary circulation: Right heart → lungs → oxygenation
- Systemic circulation: Left heart → body → oxygen delivery
The cardiac output (CO) = Heart Rate × Stroke Volume. At rest (72 bpm, SV ~70 mL), CO ≈ 5 L/min.
Initiation of the Heartbeat
Each cardiac cycle is initiated by a spontaneous action potential in the sinoatrial (SA) node — located in the superior lateral wall of the right atrium near the superior vena cava. The impulse travels:
SA node → Both atria → AV node (0.1 s delay) → Bundle of His → Bundle branches → Purkinje fibers → Ventricular myocardium
The 0.1 s AV nodal delay is critical: it allows atrial contraction (the "atrial kick") to complete before ventricular contraction begins, maximizing ventricular filling. The atria thus act as primer pumps for the ventricles.
2. The Cardiac Cycle — Seven Phases
The cardiac cycle = all events from the beginning of one heartbeat to the next. At 72 bpm, total duration ≈ 0.833 seconds (systole ~0.3 s, diastole ~0.5 s).
Here is the full Wiggers diagram (Costanzo Physiology) showing all phases simultaneously — pressure curves, ventricular volume, venous pulse, heart sounds, and ECG:
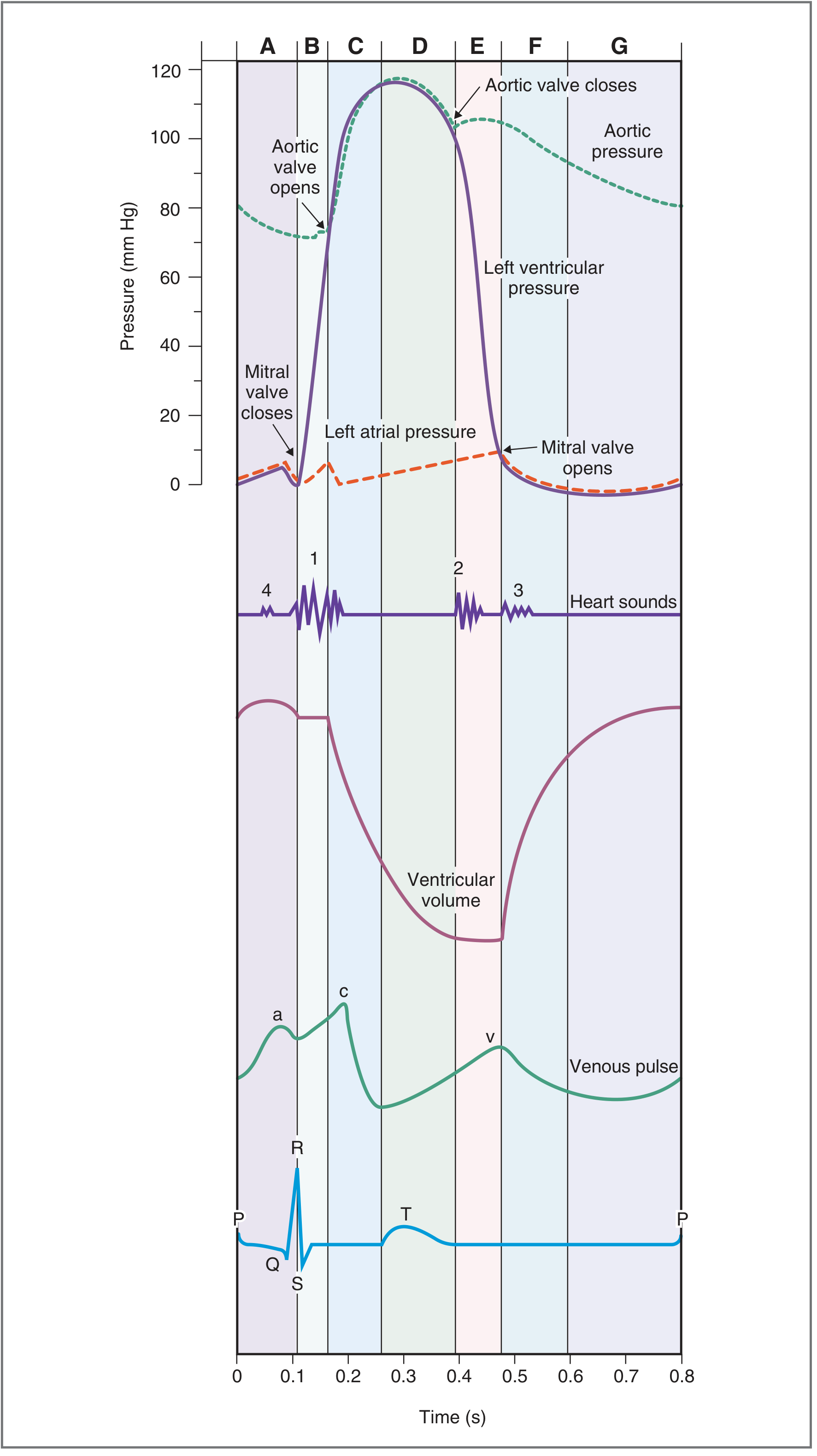
Phase A — Atrial Systole
- ECG event: P wave (atrial depolarization)
- Mechanism: Left atrium contracts → left atrial pressure rises → blood is actively pushed through the open mitral valve into the left ventricle
- Valve status: Mitral valve open; aortic valve closed
- Volume: Ventricular volume increases slightly (~final 20–30 mL of filling = "atrial kick")
- Venous pulse: a wave (atrial contraction reflected back to jugular veins)
- Heart sound: S4 — not heard in normal adults; heard if ventricular compliance is reduced (e.g., hypertrophy)
- Clinical note: At end of atrial systole, the ventricle reaches end-diastolic volume (EDV) ≈ 120–130 mL
Phase B — Isovolumetric Ventricular Contraction (IVC)
- ECG event: QRS complex (ventricular depolarization)
- Mechanism: Ventricles begin contracting → ventricular pressure rises rapidly → mitral valve snaps closed when LV pressure exceeds LA pressure
- Valve status: All valves CLOSED — no blood leaves or enters; volume is constant (hence "isovolumetric")
- Pressure: LV pressure rises steeply but has not yet exceeded aortic pressure (~80 mmHg)
- Heart sound: S1 ("lub") — caused by closure and vibration of mitral + tricuspid valves
- Duration: Very short (~0.05 s)
Phase C — Rapid Ventricular Ejection
- ECG event: ST segment
- Mechanism: LV pressure exceeds aortic pressure (~80 mmHg) → aortic valve opens → blood is rapidly ejected into aorta
- Valve status: Aortic valve open; mitral valve closed
- Volume: Ventricular volume falls rapidly (ejects ~70% of stroke volume here)
- Pressure: Both LV and aortic pressure rise to maximum (~120 mmHg)
- Venous pulse: c wave (tricuspid valve bulging into right atrium)
Phase D — Reduced Ventricular Ejection
- ECG event: T wave begins (ventricular repolarization)
- Mechanism: Ventricles continue ejecting but rate slows; ventricular pressure begins to fall; aortic pressure also slowly falls as blood runs off into the arterial tree
- Volume: Ventricular volume reaches minimum = end-systolic volume (ESV) ≈ 50–60 mL
- Stroke volume = EDV − ESV ≈ 70 mL
Phase E — Isovolumetric Ventricular Relaxation (IVR)
- ECG event: After T wave
- Mechanism: Ventricles relax → LV pressure falls rapidly below aortic pressure → aortic valve closes
- Valve status: All valves CLOSED again
- Volume: Constant (no flow)
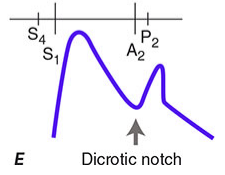
- Heart sound: S2 ("dub") — caused by closure and vibration of aortic + pulmonary valves
- Dicrotic notch: Brief backflow of blood against the closed aortic valve creates a small notch on the aortic pressure tracing
Phase F — Rapid Ventricular Filling
- Mechanism: LV pressure falls below left atrial pressure → mitral valve opens → blood flows passively and rapidly from atrium into ventricle
- Volume: LV volume rises steeply
- Venous pulse: v wave (blood accumulated in atrium during ventricular systole now empties)
- Heart sound: S3 — a low-frequency "gallop" sound at the beginning of rapid filling; normal in children/young adults; pathological in adults over 40 (indicates reduced ventricular compliance or heart failure)
Phase G — Reduced Ventricular Filling (Diastasis)
- Mechanism: Filling slows as pressure gradients equalize; ventricle passively fills at a much slower rate
- Volume: Gradual further increase until the next atrial systole
- This phase shortens significantly at high heart rates
Summary Table (Costanzo Physiology, Table 4.5)
| Phase | Events | ECG | Valves | Sound |
|---|---|---|---|---|
| A Atrial Systole | Atria contract; final ventricular filling | P wave | — | S4 |
| B Isovolumetric Contraction | LV pressure rises; all valves closed | QRS | Mitral closes | S1 |
| C Rapid Ejection | Aortic valve opens; LV ejects blood | ST segment | Aortic opens | — |
| D Reduced Ejection | Slower ejection; LV volume reaches minimum | T wave | — | — |
| E Isovolumetric Relaxation | LV pressure falls; all valves closed | — | Aortic closes | S2 |
| F Rapid Filling | Mitral opens; passive ventricular filling | — | Mitral opens | S3 |
| G Diastasis | Slow filling | — | — | — |
3. Heart Sounds in Detail
Normal auscultation: "lub-dub" — S1 followed by S2, with a silent systole between them and a longer silent diastole.
S1 — First Heart Sound ("lub")
- Timing: Beginning of systole (phase B)
- Cause: Closure of the mitral + tricuspid valves. Sudden backflow of blood against the closing AV valves causes them to bulge toward the atria, the chordae tendineae snap taut, and blood reverberates within the ventricle — generating vibrations that travel through the chest wall.
- Characteristics: Low pitch, longer (~0.14 s), heard best at the apex (mitral area)
- Components: M1 (mitral) precedes T1 (tricuspid) by a few milliseconds; normally heard as a single sound
S2 — Second Heart Sound ("dub")
- Timing: Beginning of diastole (phase E)
- Cause: Closure of the aortic + pulmonary valves. Blood rebounds back toward the ventricles, striking the closed semilunar valves and reverberating in the arterial walls.
- Characteristics: Higher pitch, shorter (~0.11 s) — semilunar valves are tauter than AV valves and produce shorter vibration
- Physiological splitting: During inspiration, increased venous return fills the RV → pulmonic valve (P2) closes slightly later than aortic valve (A2). This physiological split of S2 on inspiration is normal.
- Fixed splitting: In ASD (atrial septal defect), splitting doesn't vary with respiration
- Paradoxical splitting: In aortic stenosis or LBBB, A2 is delayed — the split is heard on expiration
S3 — Third Heart Sound
- Timing: Early diastole, during rapid ventricular filling (phase F)
- Cause: Vibrations from rapid, turbulent filling of a ventricle that suddenly decelerates when it reaches its elastic limit
- Normal in: Children, young adults, pregnant women
- Pathological in: Adults >40 years → indicates heart failure (ventricular dysfunction/increased preload) or mitral regurgitation
- Quality: Low-pitched, soft, heard best with the bell of the stethoscope at the apex
- Rhythm: Produces a "gallop" — "lub-dub-dub" (Ken-tuc-ky)
S4 — Fourth Heart Sound
- Timing: Late diastole, just before S1, during atrial systole (phase A)
- Cause: Vibrations when atria contract forcefully against a stiff (non-compliant) ventricle
- Always pathological in adults — heard in:
- Left ventricular hypertrophy (hypertension, aortic stenosis)
- Hypertrophic cardiomyopathy
- Acute MI (stiff, ischemic ventricle)
- Quality: Low-pitched; heard with bell at the apex
- Rhythm: "Ten-nes-see" — "dub-lub-dub"
4. Cardiac Murmurs — Mechanism and Classification
A murmur is produced when blood flow becomes turbulent rather than laminar. The Reynolds number determines when turbulence occurs: turbulence is more likely with high velocity, low viscosity, or large vessel diameter.
General Mechanisms of Murmur Production:
- Forward flow through a stenotic (narrowed) valve — high-velocity jet through a small orifice creates turbulence (e.g., aortic stenosis, mitral stenosis)
- Backward flow (regurgitation) through an incompetent valve — blood jets retrograde creating turbulence (e.g., mitral regurgitation, aortic regurgitation)
- Abnormal communications — blood flows between chambers/vessels at different pressures (e.g., VSD, PDA)
- High flow states — increased cardiac output can produce "innocent" flow murmurs even through normal valves (anemia, fever, pregnancy, hyperthyroidism)
Murmur Grading (Levine Scale, I–VI):
| Grade | Description |
|---|---|
| I/VI | Barely audible, requires effort |
| II/VI | Soft but easily heard |
| III/VI | Moderately loud, no thrill |
| IV/VI | Loud, with thrill palpable |
| V/VI | Very loud; heard with stethoscope barely touching chest |
| VI/VI | Heard without stethoscope |
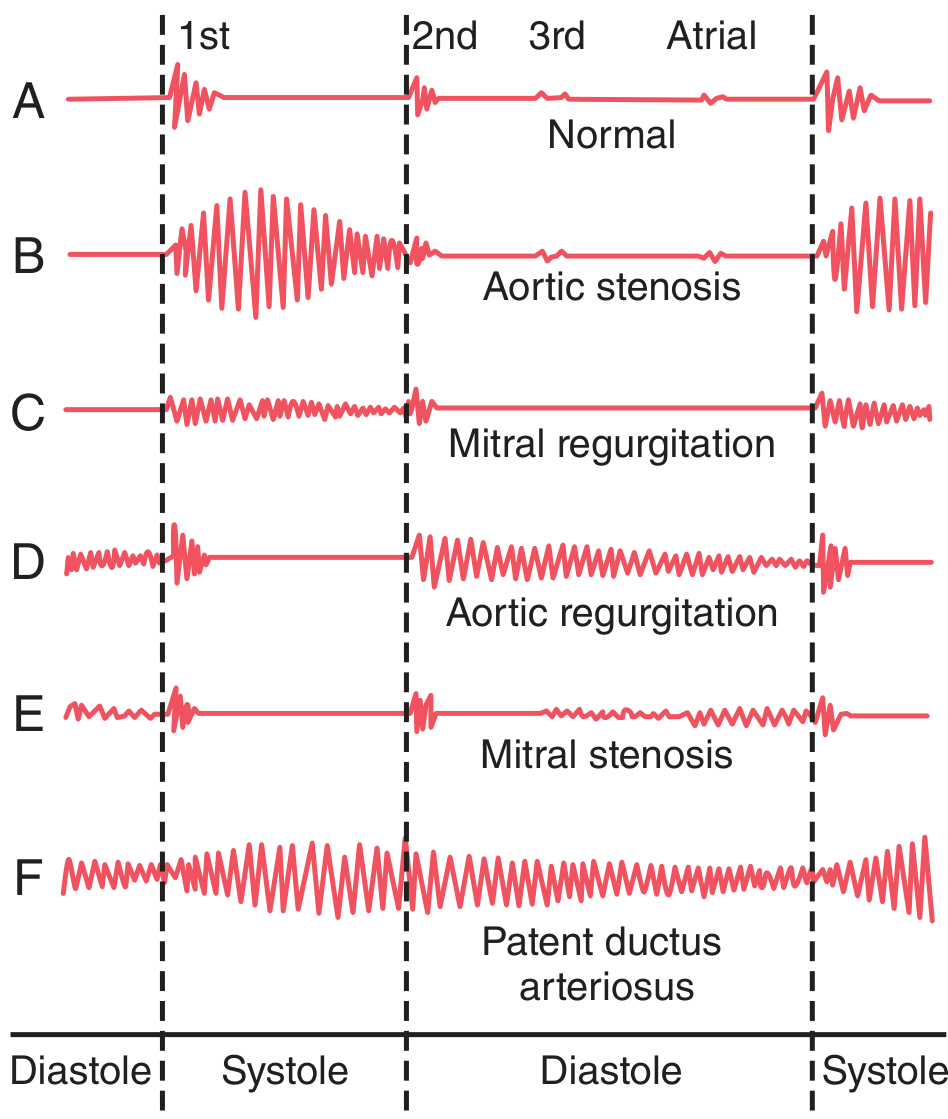
Phonocardiograms of Valvular Murmurs:
Individual Murmur Descriptions
🔴 Aortic Stenosis — Systolic Ejection Murmur
- Timing: Systolic (between S1 and S2)
- Mechanism: Blood is forced through a narrow, fibrotic/calcified aortic valve orifice. LV pressure may reach 300 mmHg. A nozzle effect creates a high-velocity jet into the aortic root → severe turbulence → loud vibration of the aortic walls.
- Character: Harsh, crescendo-decrescendo (diamond-shaped), systolic ejection murmur
- Radiation: Upper sternal border → carotid arteries
- Associated signs: Thrill at the upper chest/neck; soft/absent A2; slow-rising carotid pulse (pulsus parvus et tardus)
- Best heard: Right upper sternal border (aortic area), 2nd right intercostal space
🔴 Mitral Regurgitation — Systolic Murmur
- Timing: Systolic (holosystolic — throughout systole)
- Mechanism: Incompetent mitral valve fails to close properly → blood jets backward from high-pressure LV into low-pressure LA during systole → turbulent, high-frequency "blowing" sound
- Character: High-pitched, blowing, holosystolic
- Radiation: To the axilla
- Best heard: Apex of the heart
- Functional MR: In dilated cardiomyopathy, papillary muscle displacement pulls leaflets apart
🔵 Aortic Regurgitation — Diastolic Murmur
- Timing: Diastolic (immediately after S2, during IVR and filling)
- Mechanism: Incompetent aortic valve allows blood to flow backward from high-pressure aorta into the LV during diastole → turbulent jet into low-pressure ventricle → "blowing" sound
- Character: High-pitched, blowing, decrescendo, "soft and swishing"
- Best heard: Left sternal border (3rd/4th intercostal space), with patient leaning forward
- Duration: Starts immediately after A2; length correlates with severity
🔵 Mitral Stenosis — Diastolic Murmur
- Timing: Diastolic (mid-to-late diastole, during ventricular filling)
- Mechanism: Fibrotic/fused mitral valve leaflets restrict flow from LA into LV during diastole. Because LA pressure rarely exceeds 30 mmHg, the pressure differential is small → weak, low-frequency rumble. The ventricle is so empty and flabby that blood does not reverberate well.
- Character: Low-pitched, rumbling, presystolic accentuation (if sinus rhythm — atrial kick amplifies flow just before S1)
- Opening snap: High-pitched early diastolic sound immediately after S2 (stiff leaflets opening under LA pressure)
- Best heard: Apex, with patient in left lateral decubitus position
🟡 Patent Ductus Arteriosus (PDA) — Continuous "Machinery" Murmur
- Timing: Continuous — throughout systole and diastole (both phases)
- Mechanism: The ductus arteriosus connects the aorta to the pulmonary artery. Aortic pressure exceeds pulmonary artery pressure in both systole and diastole → continuous left-to-right shunt → turbulent flow in the pulmonary artery throughout the entire cardiac cycle
- Character: "Machinery murmur" — waxes during systole (higher aortic pressure) and wanes during diastole (lower pressure)
- Best heard: Left upper sternal border/infraclavicular area
Right Heart Murmurs
- Pulmonic stenosis: Systolic ejection murmur, best at left upper sternal border
- Tricuspid regurgitation: Holosystolic, left lower sternal border; increases with inspiration (Carvallo's sign) — more venous return to RV during inspiration increases regurgitant flow
5. Key Clinical Points — Differentiating Murmurs
| Feature | Systolic Murmur | Diastolic Murmur |
|---|---|---|
| Timing | Between S1 and S2 | Between S2 and S1 |
| Causes | AS, MR, PS, TR, VSD, HCM | AR, MS, PR, TS |
| Significance | May be innocent (flow murmur) or pathological | Always pathological |
| Murmur | Timing | Location | Radiation | Character |
|---|---|---|---|---|
| Aortic Stenosis | Systolic | R 2nd ICS | Carotids | Harsh, crescendo-decrescendo |
| Mitral Regurgitation | Holosystolic | Apex | Axilla | Blowing, high-pitched |
| Aortic Regurgitation | Early diastolic | L sternal border | — | Blowing, decrescendo |
| Mitral Stenosis | Mid-diastolic | Apex | — | Low rumble, opening snap |
| PDA | Continuous | L infraclavicular | — | Machinery murmur |
6. Integration: ECG-Cardiac Cycle-Heart Sounds
ECG: P Q R S T
| | |
Sounds: S4 S1 S2 S3
| | | |
Events: Atrial IVC Ejection IVR Filling
systole
Valves: MV AoV opens AoV MV
closes closes opens
- P wave → atrial depolarization → atrial systole → (S4 if present)
- QRS → ventricular depolarization → ventricular contraction → S1 (MV/TV closure)
- ST segment → rapid ejection phase
- T wave → ventricular repolarization → ventricular relaxation begins
- After T → S2 (AoV/PV closure) → diastole begins
- Early diastole → S3 (if present, during rapid filling)
Sources: Guyton and Hall Textbook of Medical Physiology (Chapters 9, 23) | Costanzo Physiology, 7th Edition (Chapter 4) | Harrison's Principles of Internal Medicine, 22nd Edition (Chapter 44)
Cardiology 4th year heart regurgitaon and stenosis of valvular disease detail explnation from standard textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
aortic stenosis mitral stenosis valvular heart disease echocardiography pathology
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Loading Image
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.