Uterus anatomy
Reading File
Finding Sources
Searching the Web
uterus anatomy structure layers
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
Here is a thorough overview of uterus anatomy drawn from Gray's Anatomy for Students, Sabiston's Surgery, Junqueira's Histology, and the Color Atlas of Human Anatomy.
Uterus Anatomy
Overview
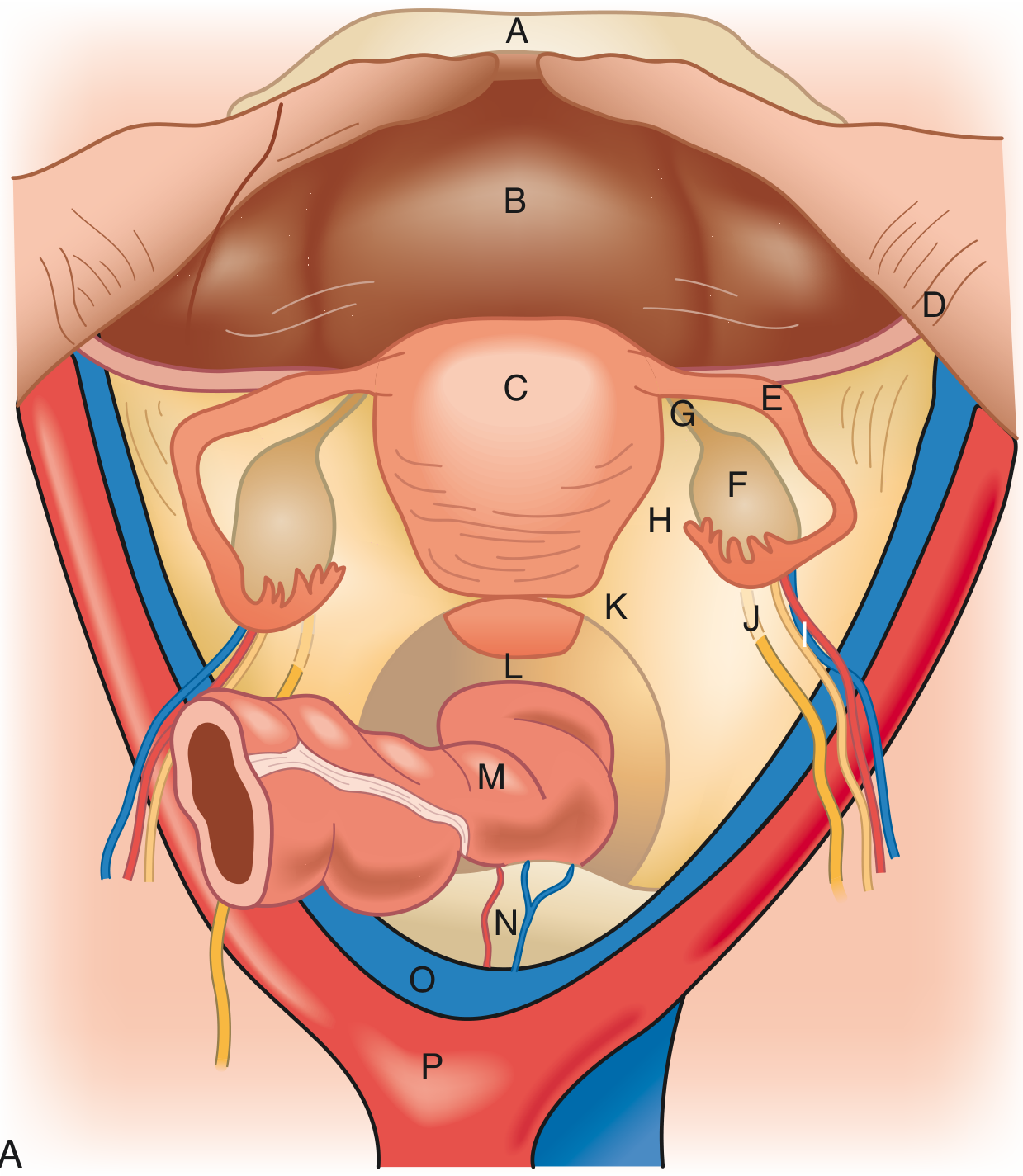
The uterus is a thick-walled, pear-shaped muscular organ that sits in the midline of the pelvis, posterior to the bladder and anterior to the rectum. It is an intraperitoneal organ. In the nonpregnant adult, it typically weighs 40-80 g. It is smaller before puberty and after menopause.
Anatomical Divisions
The uterus is divided into four regions:
| Region | Description |
|---|---|
| Fundus | The rounded superior part, above the openings of the uterine tubes |
| Body (Corpus) | The main bulk of the organ; flattened anteroposteriorly; cavity is triangular when viewed anteriorly |
| Isthmus | A narrow constriction between the body and cervix |
| Cervix | The lower cylindrical portion projecting into the vagina; ~3 cm long; mostly fibrous tissue |
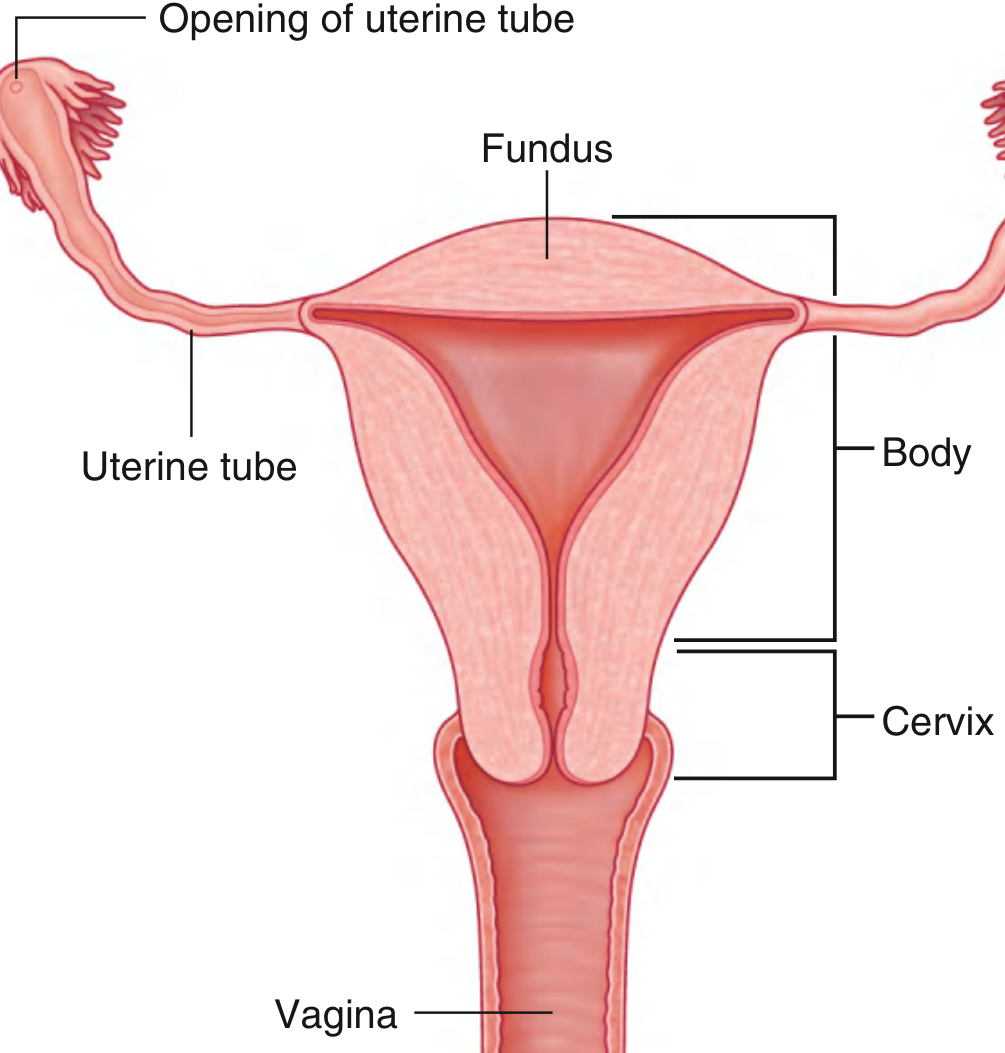
The uterine cavity is a narrow slit when viewed from the side, and triangular when viewed anteriorly. Its superior corners communicate with the lumen of each uterine tube; the inferior corner continues into the cervical canal.
The cervix has:
- An internal os - opens into the isthmus
- An external os - opens into the vagina
- The transformation zone - where the ectocervix squamous epithelium transitions to endocervical columnar epithelium; the site where cervical intraepithelial neoplasia (CIN) develops
Position
The normal adult uterus is:
- Anteverted with respect to the vagina (tilted forward)
- Anteflexed with respect to the cervix (body bent forward on the cervix)
Its exact position changes with bladder and rectal distension.
Wall Layers
The uterine wall has three layers:
1. Perimetrium (Serosa)
- The outermost layer - a thin connective tissue layer covered by mesothelium (peritoneum)
- Continuous with the broad ligaments and pelvic peritoneum
- Absent over the anterior cervix (where the bladder is adjacent)
2. Myometrium
- The thickest layer, composed of smooth muscle, connective tissue, and vessels
- Organized into three sublayers:
- Outer (supravascular) - thin
- Middle - thickest; very richly vascular with a sponge-like appearance; its 3D smooth muscle meshwork is the main layer driving fetal expulsion during labor
- Inner (subvascular) - thin
- During pregnancy, smooth muscle cells hypertrophy, allowing the uterus to expand to ~7-10x its original size
- Benign smooth muscle tumors of the myometrium = leiomyomas (fibroids)
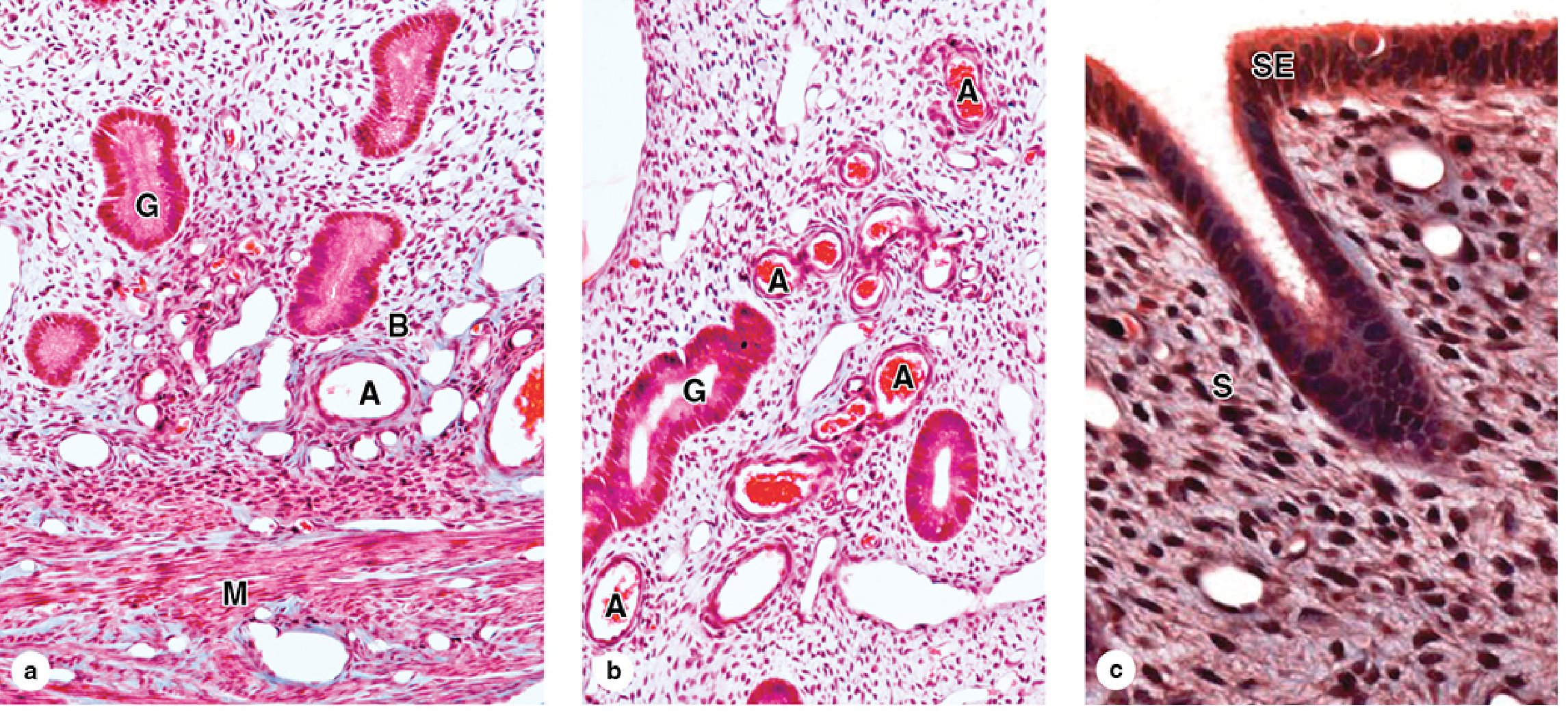
3. Endometrium
- The innermost mucosal lining; simple columnar epithelium
- Contains uterine glands (tubular invaginations of the epithelium) and a cellular connective tissue stroma
- Divided into two functional layers:
- Basalis (basal layer) - permanent; not shed during menstruation; regenerates the functionalis
- Functionalis (functional layer) - undergoes cyclic changes under ovarian hormones; shed during menstruation
Endometrial Cycle
During reproductive years, the functionalis undergoes monthly changes:
| Phase | Days | Hormone | Changes |
|---|---|---|---|
| Desquamation (menstruation) | 1-4 | Hormone withdrawal | Functional layer shed |
| Proliferative | 5-14 | Estradiol | Glands and stroma regenerate and grow |
| Secretory | 15-28 | Progesterone + estrogen | Glands produce viscous secretion; spiral arteries multiply; compact and spongy zones form |
- Curettage removes only the functionalis; the basalis remains intact
- Endometriosis = endometrial tissue migrating outside the uterus to the ovary or pelvic peritoneum
Ligaments (Supports)
The uterus is held in place by several ligaments:
| Ligament | Origin | Insertion | Function |
|---|---|---|---|
| Broad ligament | Lateral borders of uterus | Continuous with pelvic peritoneum | Drapes over uterus/tubes/ovaries |
| Round ligament | Uterine cornua | Through inguinal ring to labia majora | Maintains anteversion |
| Cardinal (transverse cervical) ligaments | Lateral pelvic diaphragm | Cervix and upper vagina | Main structural support at the cervical level |
| Uterosacral ligaments | Upper posterior cervix | Sacrum (S3) | Support; arch frames the rectum |
Blood Supply
- Uterine arteries - branches of the internal iliac arteries; travel within the cardinal ligament then run superiorly along the lateral uterus
- Ovarian arteries - arise directly from the abdominal aorta; anastomose with uterine arteries
- Venous drainage mirrors the arterial supply via the uterine venous plexus
Surgical note: During hysterectomy, the uterine arteries must be ligated with careful identification of the ureters (which cross directly beneath the uterine arteries - "water under the bridge").
Innervation
| Type | Pathway |
|---|---|
| Sympathetic | Hypogastric and ovarian plexus |
| Parasympathetic | Lumbosacral plexus (S2-S4) |
| Afferent (pain) | With sympathetic fibers via lumbosacral plexus (T11-T12) |
Cervix Histology
The cervical mucosa differs from the uterine body:
- Ectocervix - stratified squamous epithelium (like vagina)
- Endocervix - simple columnar epithelium with branching mucus-secreting glands
- No functional/basal division - the cervical mucosa does not shed cyclically
- The transformation zone (squamocolumnar junction) is the clinically important region for cervical cancer screening (Pap smear)
Key Clinical Points
- Blastocyst implantation normally occurs in the body of the uterus
- During pregnancy, the uterus expands dramatically into the abdominal cavity
- Fibroids (leiomyomas) are the most common benign uterine tumors
- Hysterectomy (removal of uterus) can be total (body + cervix) or subtotal (cervix spared)
Sources: Gray's Anatomy for Students; Sabiston Textbook of Surgery; Color Atlas of Human Anatomy Vol. 2 (Internal Organs); Junqueira's Basic Histology, 17e
This is a shared conversation. Sign in to Orris to start your own chat.