I now have comprehensive, authoritative data from multiple major textbooks. Let me compile the full detailed response.
Shock: Detailed Overview
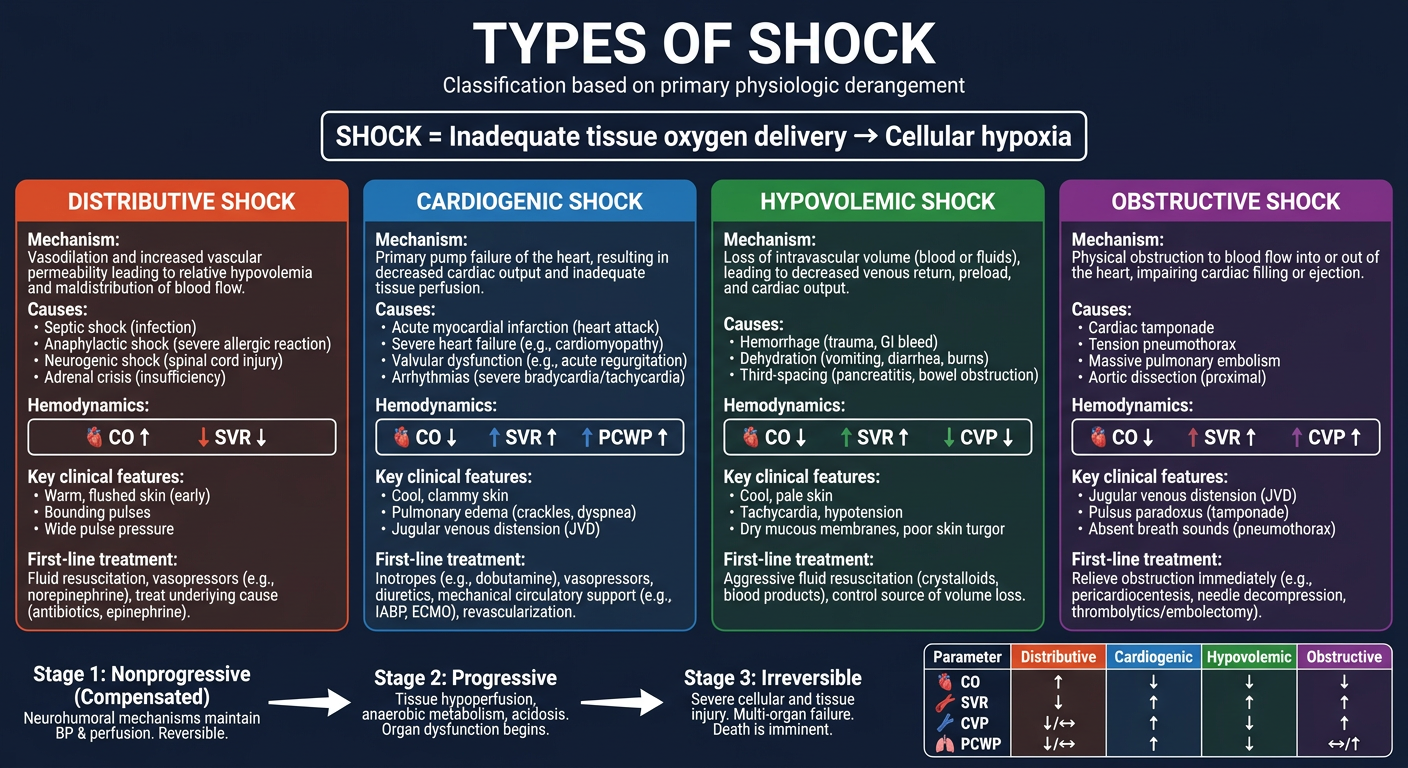
Shock is a life-threatening state of systemic tissue hypoperfusion resulting from an imbalance between oxygen delivery and cellular oxygen demand, leading to cellular hypoxia and, if untreated, irreversible organ dysfunction and death. The cellular oxygen imbalance is most commonly related to impaired oxygen delivery in the setting of circulatory failure.
- Harrison's Principles of Internal Medicine 22E, p. 2353
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 134
Pathophysiology (Cellular Level)
When oxygen supply is insufficient, cells shift from aerobic to anaerobic metabolism:
- Glucose is metabolized to lactate instead of entering the TCA cycle
- ATP production drops dramatically (2 ATP/glucose vs. 36-38 in aerobic)
- ATP-dependent Na+/K+ ATPase fails → cellular swelling, ionic dysregulation
- Intracellular calcium influx activates phospholipases and proteases → cell death
- Intracellular contents leak into extracellular space, triggering inflammatory cascades
- Lactic acidosis develops, blunting vasomotor responses
The key formula governing oxygen delivery:
DO₂ = CO × CaO₂ (Cardiac Output × Arterial Oxygen Content)
SV ∝ (Preload × Contractility) / SVR
CaO₂ = (Hb × 1.34 × SaO₂) + (PaO₂ × 0.003)
Any disease process disrupting heart rate, preload, contractility, SVR, hemoglobin, or oxygen saturation can precipitate shock.
Classification of Shock
The four major types recognized by Harrison's, based on the primary physiologic derangement:
| Type | CVP | PCWP | Cardiac Output | SVR |
|---|
| Distributive | ↓ | ↓ | ↑ | ↓ |
| Cardiogenic | ↑ | ↑ | ↓ | ↑ |
| Obstructive | ↑ | ↓/↑ | ↓ | ↑ |
| Hypovolemic | ↓ | ↓ | ↓ | ↑ |
CVP = central venous pressure; PCWP = pulmonary capillary wedge pressure
- Harrison's, p. 2354 (Table 314-2)
1. Distributive Shock
Definition: Primary reduction in systemic vascular resistance (SVR) leading to maldistribution of blood flow. CO is characteristically elevated as compensation, but peripheral pooling prevents adequate tissue perfusion.
1a. Septic Shock
The most common form of distributive shock.
- Definition: Sepsis (life-threatening organ dysfunction from dysregulated host response to infection) + persistent hypotension requiring vasopressors + elevated lactate despite adequate volume resuscitation
- Organisms: Gram-positive bacteria (most common), gram-negative bacteria, fungi; can follow SARS-CoV-2 and other viral infections
- Pathogenesis:
- Microbial PAMPs (e.g., endotoxin, enterotoxin B) engage TLRs on innate immune cells
- Activation of NF-κB → massive cytokine release: TNF, IL-1, IL-6, IL-12, IL-18, IFN-γ, HMGB1
- Endothelial activation: loosened tight junctions → vascular leak and widespread edema
- Upregulation of nitric oxide (NO) and vasodilatory mediators → profound vasodilation
- Procoagulant state: increased tissue factor, decreased thrombomodulin and protein C → DIC in up to 50% of patients
- Metabolic derangements: insulin resistance, hyperglycemia, lactic acidosis
- Counter-inflammatory immunosuppression may follow the initial cytokine storm (oscillation between hyper- and hypoinflammatory states)
- Hemodynamic profile: Initially warm, flushed skin (vasodilation), high CO, low SVR; later may become cold and clammy as cardiac function deteriorates
- Mortality: ~40% despite modern critical care
- Robbins, Cotran & Kumar, p. 135-137
1b. Anaphylactic Shock
- Trigger: IgE-mediated hypersensitivity reaction to allergens (food, drugs, insect stings)
- Mechanism: Massive histamine release from mast cells and basophils → profound venous and arterial vasodilation; up to 35% of circulating blood volume can extravasate within 10 minutes
- Features: Urticaria, angioedema, bronchospasm, hypotension; can be rapidly fatal
- Treatment: Epinephrine is the cornerstone
1c. Neurogenic Shock
- Trigger: Severe brain or spinal cord injury
- Mechanism: Disruption of autonomic pathways regulating vascular tone → loss of sympathetic vasoconstriction → venous pooling → reduced venous return and decreased CO
- Characteristic feature: Hypotension with bradycardia (loss of sympathetic tone) - distinguishes it from other shock types that typically cause tachycardia; also presents with hypothermia and wide pulse pressure
- Harrison's, p. 2354; Harriet Lane Handbook
1d. Endocrine (Adrenal) Shock
- Cause: Adrenal insufficiency - from chronic steroid use, immune checkpoint inhibitors, metastatic malignancy, adrenal hemorrhage, TB, HIV, autoimmune adrenalitis, amyloidosis
- Mechanism: Inability to increase cortisol in stress states → vasodilation; aldosterone deficiency → hypovolemia
- Often recognized during superimposed stress (infection, surgery)
1e. Other Distributive Causes
- Severe pancreatitis, extensive burns, liver failure - mediated by inflammatory mediator release
- Harrison's, p. 2354
2. Cardiogenic Shock
Definition: Reduced oxygen delivery due to primary cardiac pump failure, leading to low CO with compensatory increase in SVR.
Causes:
- Intrinsic myocardial damage: Acute MI (most common), myocarditis, cardiomyopathy
- Mechanical complications: Ventricular rupture, acute mitral regurgitation, VSD
- Arrhythmias: Sustained VT/VF, complete heart block
- Extrinsic compression: Cardiac tamponade
- RV failure: Massive pulmonary embolism, RV infarction
Hemodynamic Profile:
- Left ventricular involvement: ↑ PCWP, ↑ CVP, ↓ CO, ↑ SVR
- Right ventricular involvement: ↑ CVP, ↓ PCWP, ↓ CO, ↑ SVR
Clinical Features:
- Cold, clammy skin, weak rapid pulse, hypotension
- Pulmonary edema (in LV failure) - differentiates from hypovolemic shock
- Jugular venous distension (JVD), S3 gallop
- Oliguria, altered mental status
Management:
- Treat the underlying cause (reperfusion in MI, pericardiocentesis in tamponade)
- Inotropes (dobutamine), vasopressors (norepinephrine)
- Mechanical circulatory support (IABP, Impella, ECMO) in refractory cases
- Robbins, Cotran & Kumar, p. 134; Harrison's p. 2354
3. Hypovolemic Shock
Definition: Reduced CO due to insufficient intravascular volume. Characterized by low CVP, low PCWP, low CO, and elevated SVR.
Causes:
- Hemorrhagic (most common in trauma):
- External bleeding (lacerations, penetrating trauma)
- Internal bleeding (GI hemorrhage, ruptured aortic aneurysm, ectopic pregnancy, splenic rupture, pelvic fractures)
- Non-hemorrhagic:
- Fluid loss: vomiting, diarrhea, fistula drainage, excessive diuresis
- Burns (massive plasma protein loss)
- Third-spacing (pancreatitis, bowel obstruction, peritonitis)
ATLS Classification of Hemorrhagic Shock:
| Parameter | Class I | Class II | Class III | Class IV |
|---|
| Blood loss (%) | 0-15% | 15-30% | 30-40% | >40% |
| Pulse (bpm) | <100 | >100 | >120 | >140 |
| Blood pressure | Normal | Normal | Decreased | Decreased |
| Pulse pressure | Normal | Decreased | Decreased | Decreased |
| Respiratory rate | 14-20 | 20-30 | 30-40 | >35 |
| Urine output (mL/h) | >30 | 20-30 | 5-15 | Negligible |
| CNS | Slightly anxious | Mildly anxious | Anxious/confused | Confused/lethargic |
| Fluid resuscitation | Crystalloid | Crystalloid | Crystalloid + blood | Crystalloid + blood |
Note: ATLS classes are clinically useful but have limitations - elderly patients decompensate earlier; children compensate until a tipping point then rapidly deteriorate.
- Sabiston Textbook of Surgery, p. 567 (Table 33.1)
Clinical Features:
- Cold, clammy, pale skin (sympathetic vasoconstriction)
- Tachycardia, hypotension, narrow pulse pressure
- Oliguria (renal vasoconstriction)
- Flat neck veins (low venous pressure)
- No pulmonary edema (distinguishes from cardiogenic)
4. Obstructive Shock
Definition: Shock caused by a mechanical obstruction to cardiac filling or outflow, resulting in decreased effective CO despite normal myocardial function.
Causes:
Obstruction to cardiac filling (inflow):
- Cardiac tamponade: Pericardial fluid compresses the heart; Beck's triad (hypotension, JVD, muffled heart sounds)
- Tension pneumothorax: Mediastinal shift compresses the great veins, reducing venous return
- Constrictive pericarditis: Chronic pericardial fibrosis restricts diastolic filling
Obstruction to cardiac outflow:
- Massive pulmonary embolism: Right heart obstruction
- Venous air embolism / fat embolism: Right heart obstruction
- Aortic dissection: Left ventricular outflow obstruction
- Severe aortic stenosis
Hemodynamic Profile:
- ↑ CVP (elevated right-sided pressures)
- PCWP variable (↓ in PTX/tamponade, ↑ in LV outflow obstruction)
- ↓ CO, ↑ SVR
Clinical Features:
-
JVD with hypotension (key clue)
-
Tracheal deviation and absent breath sounds (tension PTX)
-
Pulsus paradoxus (tamponade)
-
Clinical urgency: must be recognized and treated immediately (needle decompression, pericardiocentesis, thrombolytics)
-
Harrison's, p. 2354; Tintinalli's Emergency Medicine; Washington Manual
5. Mixed Shock
Multiple shock types frequently coexist. For example:
-
Sepsis may cause distributive shock AND secondary cardiogenic shock (sepsis-induced cardiomyopathy)
-
Trauma may cause hypovolemic shock AND obstructive shock (tension pneumothorax)
-
The dominant type should guide initial therapy while addressing all components
-
Harrison's, p. 2354
Stages of Shock (Any Type)
All forms of shock follow a common progression described by Robbins and Guyton:
Stage 1: Nonprogressive (Compensated)
- Neurohumoral compensatory mechanisms activated: baroreceptor reflexes, catecholamine release, ADH, RAAS activation, generalized sympathetic stimulation
- Net result: tachycardia, peripheral vasoconstriction, renal fluid conservation
- Blood is shunted from skin to vital organs (heart and brain)
- Skin is cool, pale (except septic shock - may be warm and flushed)
- Vital organ perfusion maintained; recovery possible without major intervention
Stage 2: Progressive
- If underlying cause not corrected, tissue hypoxia worsens
- Anaerobic glycolysis → lactic acid accumulation → metabolic acidosis
- Arterioles dilate; blood pools in microcirculation
- Endothelial cells at risk for anoxic injury → potential DIC
- Vital organs begin to fail
Stage 3: Irreversible
-
Widespread cell injury; lysosomal enzyme leakage further worsens the state
-
Myocardial contractility deteriorates (increased NO synthesis)
-
Ischemic bowel allows intestinal flora to enter circulation → superimposed bacteremic shock
-
Renal failure (acute tubular necrosis)
-
Despite maximal intervention, death occurs
-
Robbins, Cotran & Kumar, p. 137; Guyton & Hall Medical Physiology
Morphological Changes in Shock (Pathology)
| Organ | Change |
|---|
| Brain | Ischemic encephalopathy, "watershed" infarcts (border zones) |
| Heart | Subendocardial hemorrhage/necrosis, band necrosis |
| Kidney | Acute tubular necrosis (cortical pallor); most common cause of reversible acute kidney injury |
| Adrenals | Cortical lipid depletion (stress response - increased steroid synthesis) |
| Lungs | "Shock lung" = diffuse alveolar damage / ARDS (in septic or traumatic shock) |
| GI tract | Hemorrhagic enteropathy; ischemic colitis; bacterial translocation |
| Liver | Centrilobular necrosis (zone 3, most distal from portal blood) |
| Kidney glomeruli | Fibrin thrombi (especially in DIC/septic shock) |
Note: Neurons and cardiomyocytes, once lost, cannot fully recover. Most other tissues can recover if the patient survives.
- Robbins, Cotran & Kumar, p. 137
Clinical Features Summary
| Feature | Hypovolemic | Cardiogenic | Distributive (Septic) | Obstructive |
|---|
| Skin | Cold, pale, clammy | Cold, pale, clammy | Warm, flushed (early) | Variable |
| Neck veins | Flat | Distended | Flat/variable | Distended |
| Breath sounds | Clear | Crackles (pulm. edema) | Clear | May be absent (PTX) |
| Heart sounds | Normal | S3 gallop, murmur | Normal | Muffled (tamponade) |
| Pulse pressure | Narrow | Narrow | Wide | Narrow |
| Fever | No | No | Yes (sepsis) | No |
General Management Principles
- Identify and treat the underlying cause - this is the single most important intervention
- Airway and oxygenation - secure airway, supplemental O₂, consider intubation
- Vascular access - large-bore IV or central venous access
- Fluid resuscitation:
- Hypovolemic: crystalloids first, then blood products (Class III-IV hemorrhage)
- Cardiogenic: cautious fluids (risk of worsening pulmonary edema)
- Septic: 30 mL/kg crystalloid within 3 hours (Surviving Sepsis guidelines)
- Obstructive: definitive treatment of obstruction (pericardiocentesis, needle decompression)
- Vasopressors: Norepinephrine is first-line for most shock states requiring vasopressor support; target MAP ≥65 mmHg
- Inotropes: Dobutamine for cardiogenic shock with low CO
- Specific therapies:
- Epinephrine for anaphylaxis
- Antibiotics + source control for sepsis
- Reperfusion (PCI/thrombolytics) for MI
- Needle decompression for tension pneumothorax
- Pericardiocentesis for cardiac tamponade
- Monitor: Lactate clearance, urine output, MAP, mental status as endpoints of resuscitation
Key Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 314
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 4
- Sabiston Textbook of Surgery, Chapter 33
- Guyton & Hall Textbook of Medical Physiology
- Tintinalli's Emergency Medicine; Washington Manual of Medical Therapeutics