E xplain diarrhoea
Reading File
Finding Sources
Searching PubMed
"diarrhea"[MeSH Terms] AND pathophysiology
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have rich, comprehensive content. Let me compile the full answer.
Diarrhoea
Definition
Diarrhoea is a symptom, not a disease, defined as the passage of abnormally loose or watery stools, typically three or more times per day. Objectively, stool output exceeding 200 g/day is generally accepted as the upper limit of normal in Western countries. It is classified as:
- Acute - lasting < 4 weeks (most cases resolve within days)
- Chronic - lasting ≥ 4 weeks, which warrants investigation to exclude serious pathology
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 204
Epidemiology
- 7.5% of Americans have acute gastroenteritis symptoms in any given month
- Over 3.5 million outpatient visits for diarrhoea occur annually in the USA, with >180,000 hospital admissions and ~3,000 deaths per year
- Chronic diarrhoea affects ~6.6% of the general population per year
- In developing countries, acute infectious diarrhoea remains a leading cause of death, especially in children
- Sleisenger and Fordtran's, p. 204
Pathophysiology
Normally, the small intestine and colon absorb 99% of the ~9-10 litres of fluid that passes the ligament of Treitz daily (from oral intake plus secretions from salivary glands, stomach, liver, and pancreas). A reduction in net water absorption of as little as 1% is sufficient to cause diarrhoea.
Three fundamental mechanisms disrupt this:
- Altered rate of mucosal water/electrolyte transport in the small intestine or colon
- Rapid transit - less time available for water absorption, especially in the colon
- Altered stool solids composition - changing stool consistency independent of water content
- Sleisenger and Fordtran's, p. 205
Classification of Diarrhoea by Mechanism
The four general pathophysiological mechanisms are:
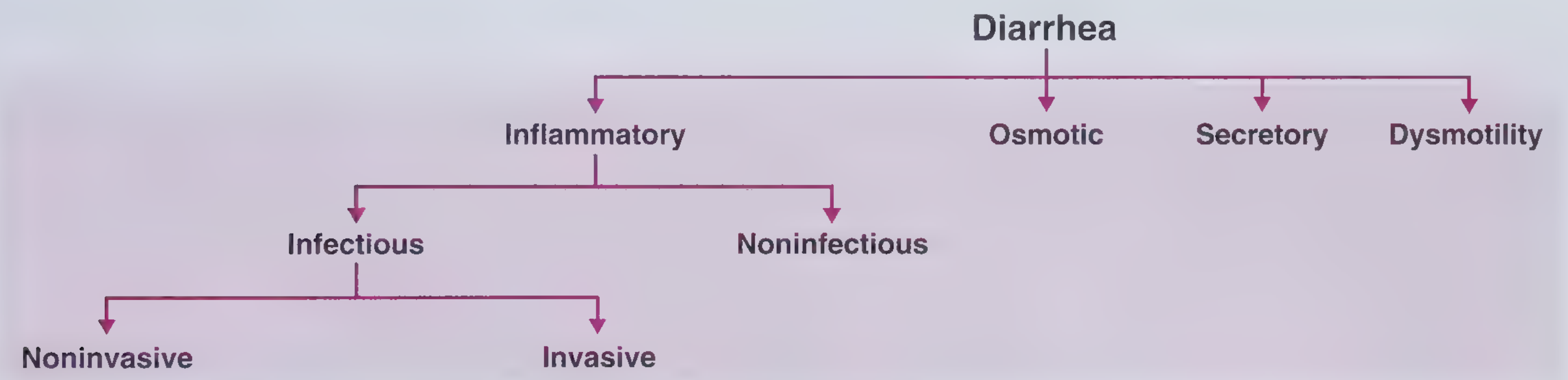
Frameworks for Internal Medicine
1. Osmotic Diarrhoea
Caused by non-absorbable solutes in the intestinal lumen that retain water osmotically.
- Classic example: lactase deficiency - undigested lactose stays in the lumen, retains water, and colonic bacteria degrade it into more osmotically active particles
- Other causes: osmotic laxatives (Mg²⁺, phosphate, sulphate), fructose/sorbitol ingestion, FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols), polyethylene glycol
- Key feature: resolves with fasting - stops when the offending substance is removed
- Stool electrolytes are low; there is a measurable fecal osmotic gap
2. Secretory Diarrhoea
Caused by net secretion of anions (Cl⁻ or HCO₃⁻), net secretion of K⁺, or net inhibition of Na⁺ absorption by the enterocolonic mucosa.
The diagram below shows the mechanism at crypt epithelial cells - cholera toxin activates adenylyl cyclase (AC) via a G-protein (Gs), raising intracellular cAMP, which opens CFTR Cl⁻ channels in the apical membrane. Na⁺ and water follow passively into the lumen:
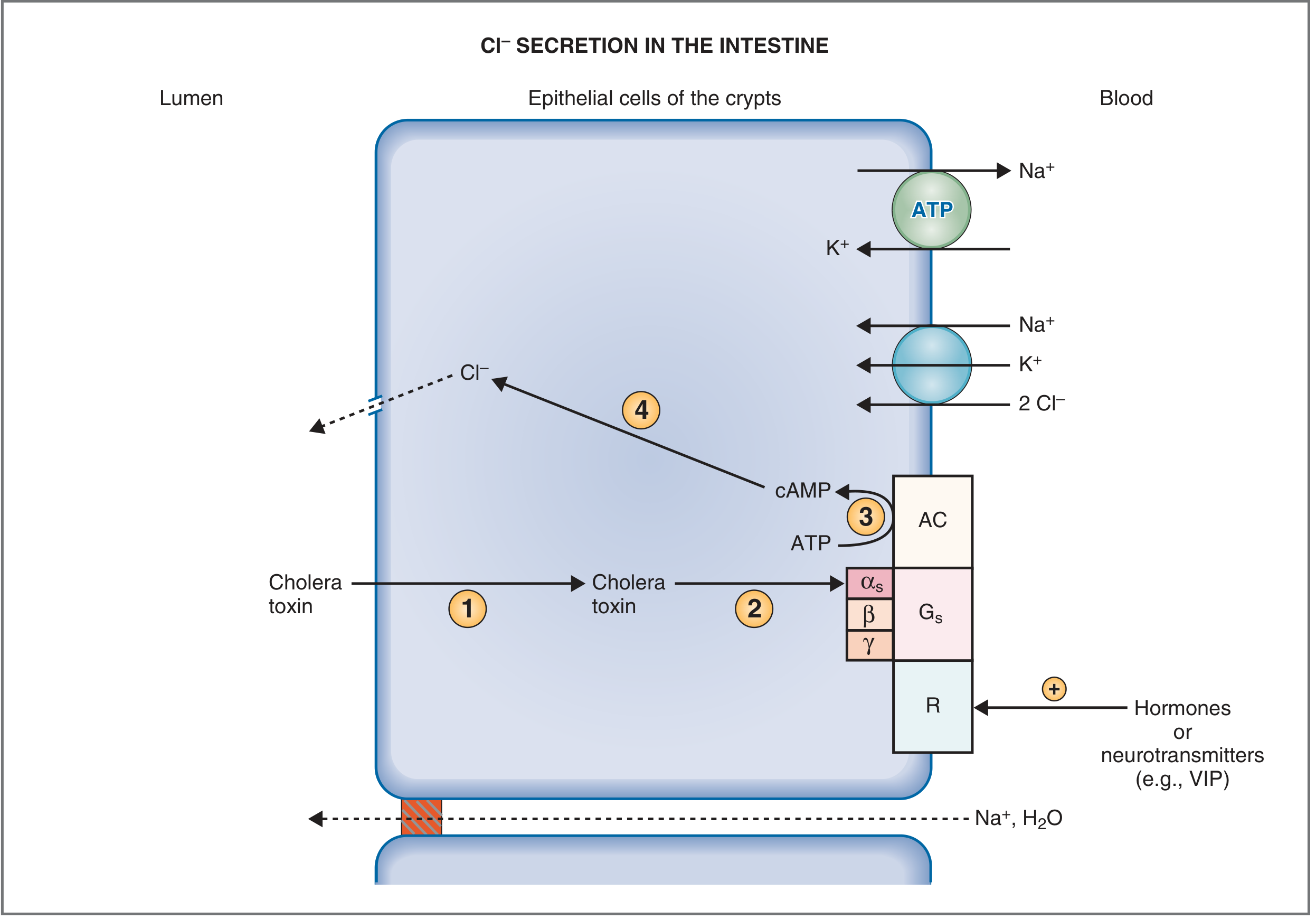
Costanzo Physiology, Fig. 8.36
Key features of secretory diarrhoea:
- Large volume, watery stools that are typically painless
- Persists with fasting (unlike osmotic)
- No fecal osmotic gap
- Caused by: bacterial enterotoxins (E. coli, V. cholerae), VIP-secreting tumours (VIPoma), carcinoid, gastrinoma, medullary thyroid cancer, bile acid malabsorption, drugs/laxatives, congenital transport defects
The most common cause is infection. E. coli heat-stable enterotoxin acts on guanylate cyclase C receptors, raising cGMP and stimulating Cl⁻ secretion via CFTR. Many enterotoxins also block Na⁺-H⁺ exchange, reducing absorption.
- Sleisenger and Fordtran's, p. 206
3. Inflammatory (Exudative) Diarrhoea
Mucosal disruption results in exudation of serum, blood, and mucus into the intestinal lumen; destruction of absorptive epithelium also causes malabsorption.
- Associated with: abdominal pain, fever, tenesmus, bloody/mucoid stools
- Stool shows polymorphonuclear leukocytes or inflammatory proteins (calprotectin, lactoferrin)
- Causes: invasive bacterial infections (Salmonella, Shigella, Campylobacter, C. difficile), IBD (Crohn's disease, ulcerative colitis), radiation injury, GI malignancies, ischaemic colitis
- Life-threatening complication: toxic megacolon (fever, tachycardia, abdominal distension, delirium)
4. Dysmotility Diarrhoea
Altered intestinal motility reduces contact time between luminal contents and the absorptive mucosa.
- Causes: irritable bowel syndrome (IBS), hyperthyroidism, prokinetic drugs, postvagotomy, visceral neuropathies
Electrolyte Consequences
Diarrhoeal fluid is rich in:
- HCO₃⁻ (from salivary, pancreatic, and intestinal secretions) → loss causes hyperchloremic normal anion-gap metabolic acidosis
- K⁺ (via flow-rate-dependent colonic K⁺ secretion) → loss causes hypokalaemia
- Water/Na⁺ → hypovolaemia, reduced intravascular volume, and circulatory collapse in severe cases
Baroreceptor and renin-angiotensin-aldosterone mechanisms attempt to restore blood pressure but are overwhelmed if losses are large or rapid.
- Costanzo Physiology, p. 392
Major Causes by Duration
Acute Diarrhoea (< 4 weeks)
| Category | Examples |
|---|---|
| Viral | Norovirus, rotavirus, adenovirus |
| Bacterial (non-invasive/toxin) | E. coli (ETEC), V. cholerae, S. aureus, Bacillus cereus |
| Bacterial (invasive) | Salmonella, Shigella, Campylobacter, C. difficile |
| Protozoal | Giardia, Cryptosporidium, Entamoeba histolytica |
| Drugs | Antibiotics, NSAIDs, antacids, laxatives |
| Dietetic | Excessive FODMAPs, alcohol |
Chronic Diarrhoea (≥ 4 weeks) by Mechanism
Secretory causes: stimulant laxatives, chronic ethanol, bile acid malabsorption (BAD - accounts for ~40% of unexplained chronic diarrhoea), hormone-producing tumours (VIPoma, carcinoid, gastrinoma), Addison's disease, congenital electrolyte transport defects
Osmotic causes: lactase/disaccharide deficiency, non-absorbable carbohydrates, FODMAPs, osmotic laxatives
Steatorrheal/malabsorptive: pancreatic exocrine insufficiency, celiac disease, Whipple's disease, bacterial overgrowth, short bowel syndrome
Inflammatory: IBD (Crohn's, ulcerative colitis), microscopic colitis, lymphocytic/collagenous colitis, eosinophilic gastroenteritis, radiation enteritis
Dysmotility: IBS, hyperthyroidism, postvagotomy, prokinetics
Iatrogenic: post-cholecystectomy, ileal resection, bariatric surgery
- Harrison's Principles of Internal Medicine 22E, Table 49-3
Clinical Evaluation
History
- Duration, frequency, volume, consistency, presence of blood/mucus
- Associated symptoms: fever, weight loss, abdominal pain, tenesmus
- Dietary history, travel history, medications, family history
- Epidemiologic context (immunosuppression, HIV, hospitalisation)
Physical Examination
- Signs of dehydration: tachycardia, hypotension, reduced skin turgor, dry mucous membranes
- Abdominal examination: distension, tenderness, bowel sounds
- Perianal inspection
Investigations
For acute diarrhoea:
- Most resolve without investigation
- Stool cultures + microscopy if: fever, bloody stool, immunosuppression, symptoms > 3-4 days
- Stool for C. difficile toxin in hospital-acquired or post-antibiotic diarrhoea
For chronic diarroea:
- Stool characterisation: watery vs. fatty vs. inflammatory
- Basic bloods: FBC, CRP, ESR, LFTs, TFTs, coeliac antibodies (anti-tTG)
- Stool osmotic gap = 290 - 2×(stool Na + stool K): gap >50 mOsm/kg = osmotic; gap <50 = secretory
- Faecal calprotectin (screens for organic vs. functional cause)
- Colonoscopy + biopsy for inflammatory or neoplastic causes
- CT/MRI enterography for small bowel disease
- SeHCAT scan or serum FGF-19 for bile acid malabsorption
Treatment
Acute Diarrhoea
- Oral rehydration therapy (ORT) is the cornerstone - glucose-coupled Na⁺ transport is preserved even in secretory diarrhoea
- Antimotility agents: loperamide (reduces stool frequency, does not use in bloody/febrile diarrhoea)
- Antibiotics only for specific organisms (Shigella, Campylobacter, C. difficile, cholera), traveller's diarrhoea, or immunocompromised patients
- Bismuth subsalicylate has antisecretory and antimicrobial effects
Chronic Diarrhoea
- Treatment directed at the underlying cause wherever possible
- Bile acid sequestrants (cholestyramine, colesevelam) for BAD
- Pancreatic enzyme replacement for exocrine insufficiency
- Gluten-free diet for coeliac disease
- 5-aminosalicylates, steroids, biologics for IBD
- Budesonide for microscopic colitis
- Somatostatin analogues (octreotide) for VIPoma/carcinoid diarrhoea
- Low-FODMAP diet for IBS-diarrhoea
Complications
| Complication | Mechanism |
|---|---|
| Dehydration | Volume loss (up to 9+ L/day in severe cases) |
| Metabolic acidosis | HCO₃⁻ loss in stool |
| Hypokalaemia | K⁺ loss in diarrhoeal fluid |
| Hypovolaemic shock | Circulatory collapse if losses are massive/rapid |
| Malnutrition | Chronic malabsorptive diarrhoea |
| Toxic megacolon | Inflammatory diarrhoea complication |
Special Populations
- HIV/AIDS: Diarrhoea occurred in up to 90% of patients pre-HAART. Common organisms: Cryptosporidium (most frequent protozoa), CMV, MAC, Microsporidium. Now more often HAART-induced or from unrelated disorders.
- Hospitalized patients: C. difficile toxin-mediated colitis, overflow diarrhoea from faecal impaction, ischaemic colitis, tube feeding
- Diabetics: Autonomic neuropathy (altered motility), associated coeliac disease, pancreatic exocrine insufficiency, metformin/acarbose side effects
- Children: Rotavirus is the leading cause worldwide; oral rehydration is the mainstay of management
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Harrison's Principles of Internal Medicine 22E; Costanzo Physiology 7th Ed.; Frameworks for Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.