Latest guidline of thyroid storm management
Reading File
Finding Sources
Searching PubMed
thyroid storm management guideline
Searching the Web
thyroid storm management guidelines 2024 2025
Reading File
Reading File
Searching PubMed
thyroid storm treatment PTU beta blocker iodine
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC9462913/
Reading File
Reading File
Searching PubMed
thyroid storm ICU outcomes treatment 2024
Loading Image
Here is a comprehensive, current summary of thyroid storm management based on Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, and the latest clinical reviews.
Thyroid Storm: Current Management Guidelines
Overview
Thyroid storm (thyrotoxic crisis) is a life-threatening extreme form of thyrotoxicosis with multiorgan dysfunction. Untreated mortality approaches 100%; with prompt treatment, mortality remains 10–30%. All confirmed or suspected cases require ICU admission.
Diagnosis
Thyroid storm is a clinical diagnosis — do not delay treatment waiting for labs.
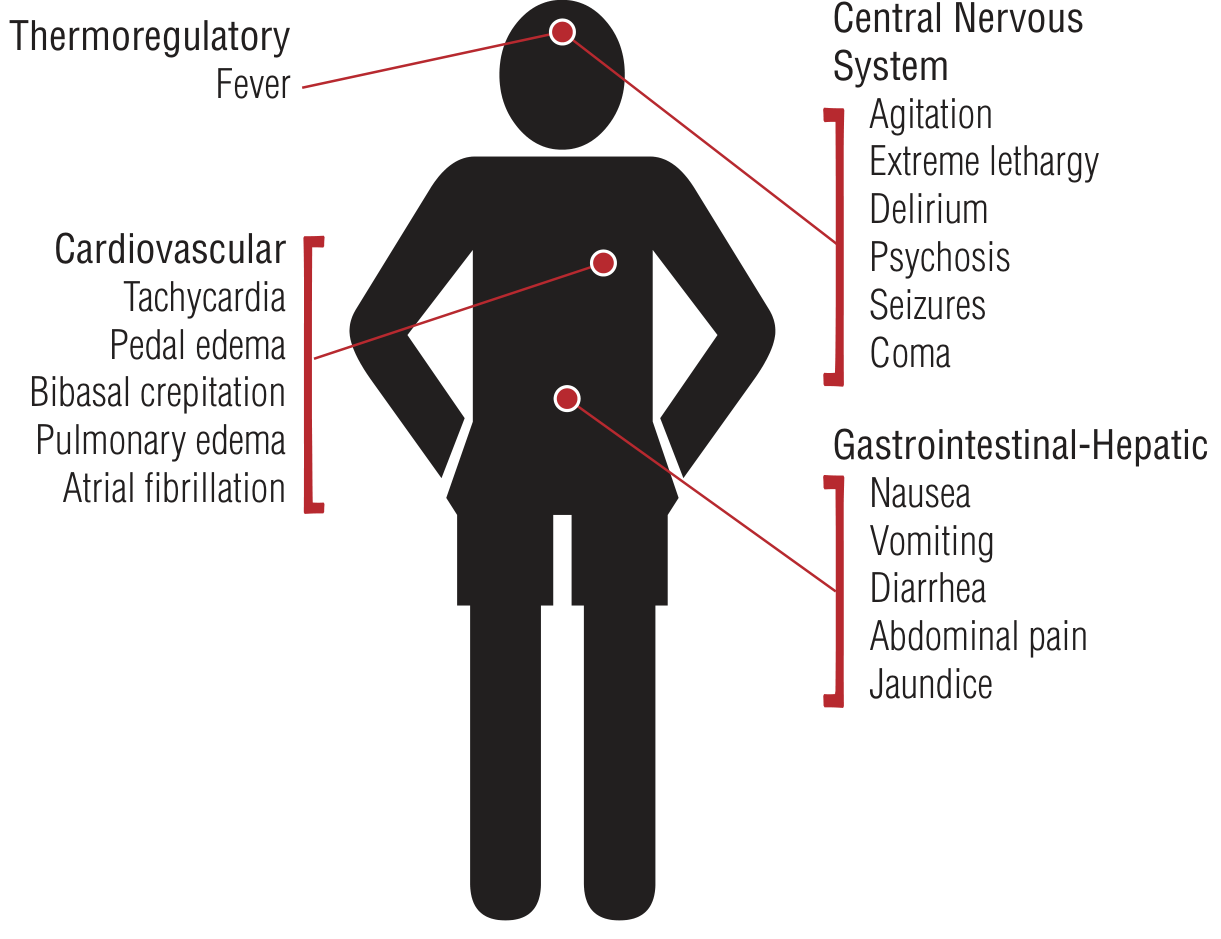
Burch-Wartofsky Point Scale (BWPS)
| Parameter | Points |
|---|---|
| Temperature | |
| 37.2–37.7°C (99–99.9°F) | 5 |
| 37.8–38.2°C (100–100.9°F) | 10 |
| 38.3–38.8°C (101–101.9°F) | 15 |
| 38.9–39.4°C (102–102.9°F) | 20 |
| 39.5–39.9°C (103–103.9°F) | 25 |
| ≥40°C (≥104°F) | 30 |
| Tachycardia (bpm) | |
| 90–109 | 5 |
| 110–119 | 10 |
| 120–129 | 15 |
| 130–139 | 20 |
| ≥140 | 25 |
| CNS Effects | |
| Absent | 0 |
| Mild agitation | 10 |
| Delirium/psychosis/extreme lethargy | 20 |
| Seizure/coma | 30 |
| GI-Hepatic Dysfunction | |
| Absent | 0 |
| Moderate (nausea/vomiting/diarrhea/abdominal pain) | 10 |
| Severe (jaundice) | 20 |
| Congestive heart failure | |
| Absent | 0 |
| Mild (pedal edema) | 5 |
| Moderate (bibasal crepitation) | 10 |
| Severe (pulmonary edema) | 15 |
| Atrial fibrillation | 10 |
| Precipitant identified | 0 |
| No precipitant identified | 10 |
- ≥45 points: Thyroid storm
- 25–44 points: Impending storm — treat aggressively
- <25 points: Storm unlikely
The Japanese Thyroid Association (JTA) criteria (TS1/TS2) also require lab evidence of elevated free thyroid hormones; BWPS ≥45 is considered more sensitive.
Treatment: Stepwise Approach
⚠️ Critical sequence: Give thionamide FIRST, then wait ≥1 hour before iodine. Iodine given before thionamide can worsen storm by providing substrate for hormone synthesis.
Step 1 — Block Adrenergic Symptoms (β-Blockers)
- Propranolol (preferred): 60–80 mg PO q4–6h, or IV 0.5–1 mg over 10 min; repeated q15min as needed
- Dual benefit: controls tachycardia AND blocks peripheral T4→T3 conversion
- Avoid if severe reactive airway disease or decompensated heart failure
- Esmolol: 50–100 mcg/kg/min IV infusion — for ICU use; advantage of rapid titration and short half-life
- Atenolol/Metoprolol (β1-selective): use if bronchospasm is a concern
- If β-blockers are contraindicated: reserpine 2.5–5 mg IM q4h or guanethidine
Step 2 — Reduce Thyroid Hormone Synthesis (Thionamides)
Give at least 1 hour before iodine.
- Propylthiouracil (PTU) (preferred by ATA): 500–1000 mg loading dose, then 250 mg PO/NG q4h
- Uniquely inhibits peripheral T4→T3 conversion (type-1 deiodinase inhibition)
- Preferred in first trimester of pregnancy
- Preferred choice in severe/acute storm
- Methimazole (MMI): 60–80 mg/day PO/NG in divided doses
- Preferred by JTA due to faster normalization of thyroid hormones and better safety profile
- Preferred in 2nd/3rd trimester and for long-term use
- Neither PTU nor MMI affects pre-formed thyroid hormone — hence iodine is needed as well
Step 3 — Block Thyroid Hormone Release (Iodine)
Give ≥1 hour after thionamide (Wolff-Chaikoff effect used therapeutically).
- Saturated Solution of Potassium Iodide (SSKI): 5 drops PO q6h (preferred)
- Lugol's solution: 8–10 drops PO q6–8h
- Sodium iodide: 500 mg IV q8–12h (if no oral access)
- Lithium carbonate: 300 mg PO q6h — alternative when iodine is contraindicated (Graves' disease with iodine allergy); inhibits hormone release
Step 4 — Block Peripheral T4→T3 Conversion (Corticosteroids)
- Dexamethasone: 2 mg IV q6h (also addresses relative adrenal insufficiency)
- Hydrocortisone: 100 mg IV q8h (alternative)
- Benefits: inhibits T4→T3 conversion, stabilizes vasomotor tone, addresses stress-related adrenal insufficiency
Step 5 — Cholestyramine (Adjunct for Refractory Cases)
- Cholestyramine: 1–4 g PO twice daily
- Blocks enterohepatic recirculation of thyroid hormones
- Used in severe or refractory thyrotoxicosis
Step 6 — Therapeutic Plasmapheresis
- Reserved for refractory cases not responding to maximal medical therapy
- Rapidly removes circulating thyroid hormones and autoantibodies
- Bridge to surgery or definitive therapy
Supportive Care
| Intervention | Details |
|---|---|
| Fever control | Cooling blankets, fans, ice packs; acetaminophen (avoid aspirin — displaces T4/T3 from binding proteins, worsening free hormone levels) |
| Fluid resuscitation | D5/0.9 NS — replenish glycogen stores; volume losses from fever, N/V/diarrhea |
| Agitation/CNS | Benzodiazepines (lorazepam, diazepam) |
| AF rate control | Refractory to rate control until antithyroid therapy takes effect; β-blockers are first line |
| Heart failure | Diuretics + ACE inhibitors; beta-blocker use requires caution in decompensated HF |
| Electrolytes | Replace guided by labs |
| Precipitant treatment | Empirical antibiotics if infection suspected; treat DKA, MI, PE as indicated |
| Positioning | ICU monitoring, continuous cardiac telemetry |
Common Precipitants
| Category | Examples |
|---|---|
| Systemic | Infection, trauma, surgery |
| Cardiovascular | MI, stroke, PE |
| Endocrine | DKA, hyperosmolar coma |
| Obstetric | Labor, eclampsia |
| Iatrogenic/Drug | Amiodarone, sorafenib, ipilimumab, RAI, iodine contrast, antithyroid drug withdrawal |
| Unknown | Up to 25% of cases |
Definitive Treatment
| Option | Indication |
|---|---|
| Total thyroidectomy | Severe storm, failure of medical therapy; requires euthyroid state first |
| Radioactive iodine (RAI) | Milder storm responsive to initial medical therapy; contraindicated in pregnancy |
Both ATA and JTA do not mandate a specific definitive strategy — choice is individualized based on severity and response to initial therapy. Bridging to a euthyroid state before either procedure is essential.
Special Populations
- Pregnancy: PTU preferred in 1st trimester (MMI is teratogenic — aplasia cutis, choanal atresia); MMI preferred in 2nd/3rd trimester; β-blockers used cautiously; RAI absolutely contraindicated; thyroidectomy (2nd trimester) is the definitive option if needed
- Asthma/COPD: Use β1-selective agents (esmolol, metoprolol) instead of propranolol
Summary Algorithm
Suspected Thyroid Storm
↓
ICU admission + Labs (TSH, fT4, fT3, CBC, LFTs, cultures)
↓
BWPS ≥45 (or ≥25 with high suspicion) → TREAT without waiting for labs
↓
1. β-Blocker (propranolol IV or PO)
2. PTU 500–1000 mg load, then 250 mg q4h (or MMI 60–80 mg/day)
[Wait ≥1 hour]
3. Iodine (SSKI 5 drops q6h or Lugol's 8–10 drops q6–8h)
4. Dexamethasone 2 mg IV q6h
5. Supportive: cooling, acetaminophen, fluids, benzodiazepines
6. Identify & treat precipitant
↓
Refractory → Cholestyramine, plasmapheresis
↓
Definitive: Total thyroidectomy or RAI (after euthyroid state)
Sources:
- Rosen's Emergency Medicine, 10th Ed., Chapter 117
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Chapter 229
- Braunwald's Heart Disease, 12th Ed.
- PMC review: Clinical Review and Update on the Management of Thyroid Storm (2022)
- Qatar National Clinical Guidelines: Thyrotoxicosis in Adults (2024)
This is a shared conversation. Sign in to Orris to start your own chat.