Explain the anatomy of anterior abdominal wall in full detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have everything I need for a comprehensive answer. Let me compile the full detailed response.
Anatomy of the Anterior Abdominal Wall
Sources: Gray's Anatomy for Students; General Anatomy and Musculoskeletal System (THIEME Atlas of Anatomy)
Boundaries
The anterior abdominal wall is bounded:
- Superiorly - xiphoid process and costal margins (ribs VII-XII)
- Posteriorly - vertebral column
- Inferiorly - upper parts of the pelvic bones (iliac crests, inguinal ligaments, pubic symphysis)
Layers of the Anterior Abdominal Wall (Superficial to Deep)
The wall is composed of the following layers from outside in:
- Skin
- Superficial fascia (subcutaneous tissue)
- Muscles and their aponeuroses
- Transversalis fascia
- Extraperitoneal (preperitoneal) fascia
- Parietal peritoneum
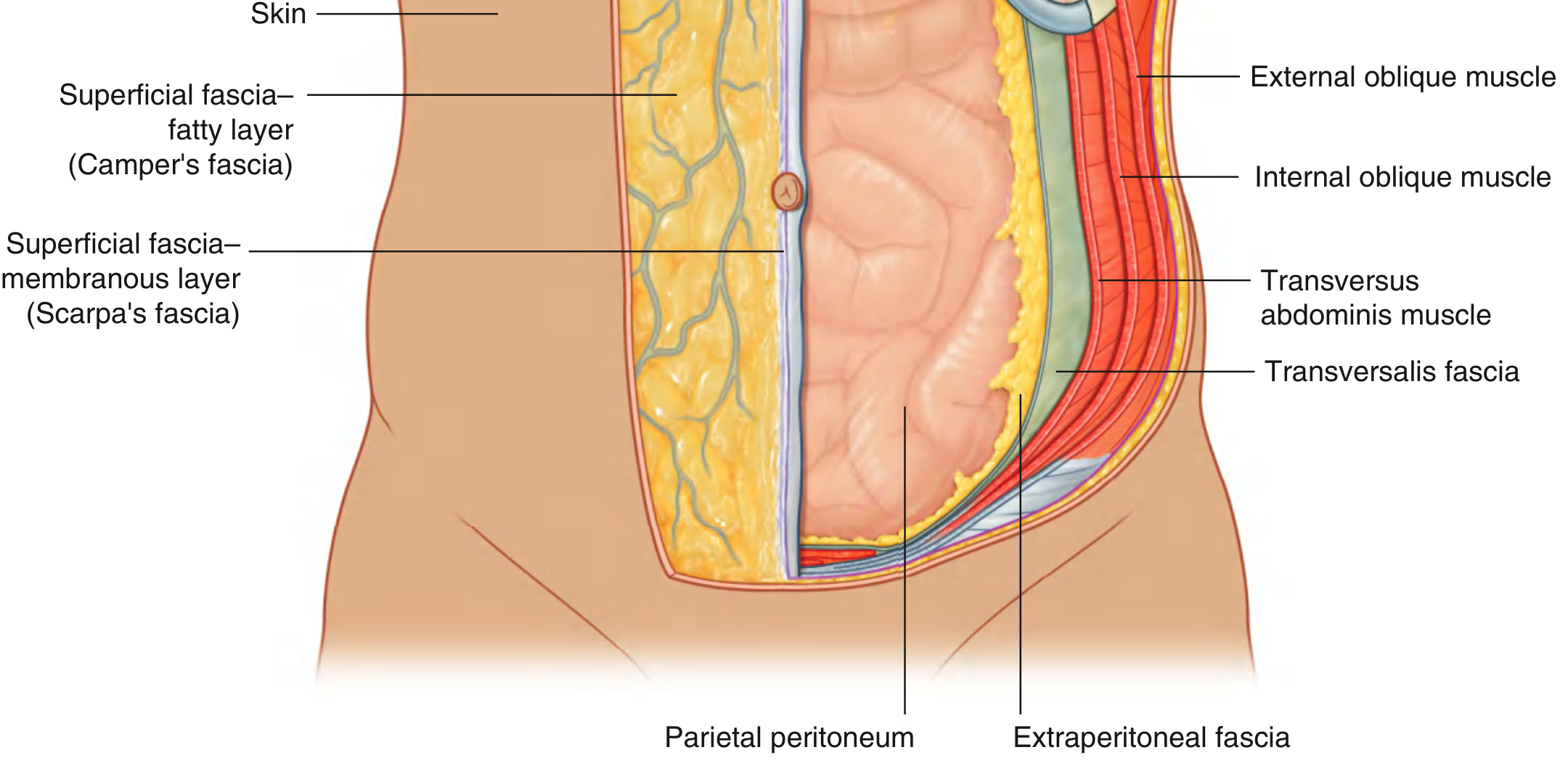
Fig. 4.24 - Layers of the abdominal wall showing all fascial and muscular layers
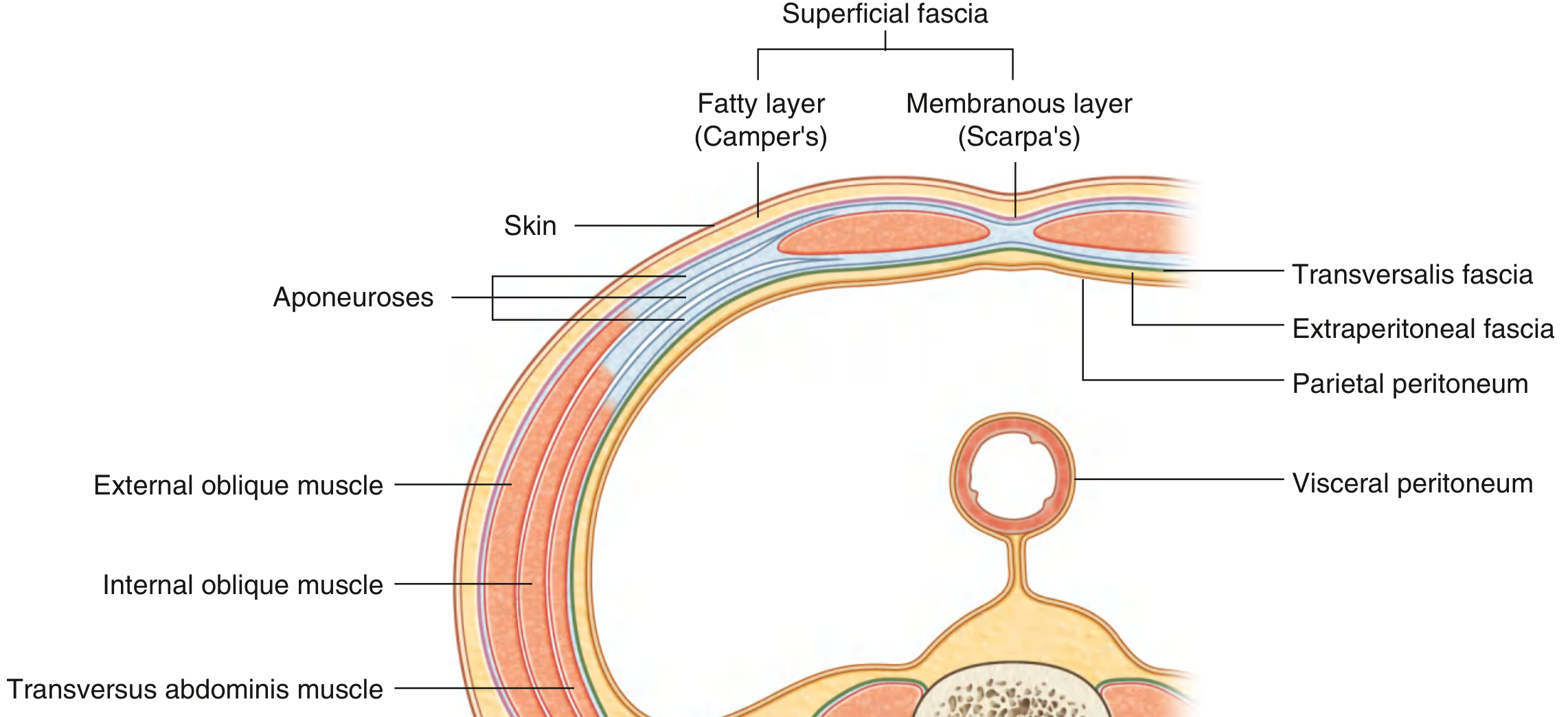
Fig. 4.34 - Transverse section showing Camper's fascia, Scarpa's fascia, muscle layers, transversalis fascia, extraperitoneal fascia, and parietal peritoneum
1. Skin
The skin over the abdominal wall is thin, mobile, and loosely attached except at the umbilicus, where it is firmly bound to the underlying scar tissue. The umbilicus is situated at approximately the level of the L3-L4 intervertebral disc (corresponding to the T10 dermatome).
2. Superficial Fascia (Subcutaneous Tissue)
The superficial fascia is generally a single fatty layer throughout most of the body. Below the umbilicus, however, it splits into two distinct layers:
Superficial Layer - Camper's Fascia
- Contains fat; thickness varies greatly with nutritional status
- Continuous over the inguinal ligament with the superficial fascia of the thigh
- In men: continues over the penis, losing fat, and continues into the scrotum where it becomes the dartos fascia (which contains smooth muscle)
- In women: retains fat and contributes to the labia majora
Deep Layer - Scarpa's Fascia
- Thin, membranous; contains little or no fat
- Inferiorly, fuses with the fascia lata of the thigh just below the inguinal ligament
- In the midline it is firmly attached to the linea alba and pubic symphysis
- Continues into the anterior perineum as Colles' fascia (superficial perineal fascia), firmly attached to the ischiopubic rami and the posterior edge of the perineal membrane
- In men: blends with the superficial layer over the penis; extensions form the fundiform ligament of the penis
Clinical relevance: Urine extravasating from a ruptured urethra (e.g., bulbar urethral rupture) tracks beneath Scarpa's fascia and Colles' fascia - it can spread onto the anterior abdominal wall and scrotum/labia, but NOT into the thighs (where Scarpa's fascia fuses with fascia lata) or the perineum posteriorly.
3. Muscles of the Anterolateral Abdominal Wall
There are five muscles in this group:
- Three flat muscles (external oblique, internal oblique, transversus abdominis)
- Two vertical muscles near the midline (rectus abdominis, pyramidalis)
Together, these muscles:
- Form a firm but flexible wall that contains the abdominal viscera
- Protect viscera from injury
- Maintain visceral position in the erect posture against gravity
- Assist forced expiration, coughing, vomiting, parturition, micturition, and defecation (all by raising intraabdominal pressure)
Muscle Summary Table
| Muscle | Origin | Insertion | Innervation | Function |
|---|---|---|---|---|
| External oblique | Outer surfaces of lower 8 ribs (V-XII) | Lateral lip of iliac crest; aponeurosis to linea alba | T7-T12 | Compress abdomen; flex trunk; rotate trunk to opposite side |
| Internal oblique | Thoracolumbar fascia; iliac crest; lateral 2/3 of inguinal ligament | Inferior border of lower 3-4 ribs; aponeurosis to linea alba; pubic crest | T7-T12, L1 | Compress abdomen; flex trunk; rotate trunk to same side |
| Transversus abdominis | Thoracolumbar fascia; medial lip of iliac crest; lateral 1/3 of inguinal ligament; costal cartilages of ribs VII-XII | Aponeurosis to linea alba; pubic crest | T7-T12, L1 | Compress abdominal contents |
| Rectus abdominis | Pubic crest, pubic tubercle, pubic symphysis | Costal cartilages of ribs V-VII; xiphoid process | T7-T12 | Compress abdomen; flex vertebral column; tense abdominal wall |
| Pyramidalis | Front of pubis and pubic symphysis | Into linea alba | T12 | Tenses the linea alba |
(Source: Gray's Anatomy for Students, Table 4.1)
External Oblique
- The most superficial of the three flat muscles
- Muscle fibers run in an inferomedial direction (like hands in pockets)
- Posterolaterally the muscle is fleshy; as it passes anteriorly it becomes an aponeurosis
- The inferior free border of the aponeurosis folds back on itself to form the inguinal ligament, running from the anterior superior iliac spine (ASIS) to the pubic tubercle
- A triangular gap in the aponeurosis just above and medial to the pubic tubercle forms the superficial inguinal ring (external inguinal ring)
- Additional specializations of the external oblique aponeurosis include the lacunar ligament (medial end, fans out to the pecten pubis) and the pectineal ligament (Cooper's ligament - the lateral extension of the lacunar ligament along the pecten pubis)
Internal Oblique
- Deep to the external oblique
- Muscle fibers run in a superomedial direction (perpendicular to external oblique, roughly at right angles)
- Arises from the thoracolumbar fascia, iliac crest, and lateral two-thirds of the inguinal ligament
- Its inferior free border arches over the spermatic cord (or round ligament in women) forming the roof of the inguinal canal
- Some of the lower fibers contribute to the cremaster muscle, which envelops the spermatic cord
Transversus Abdominis
- The deepest of the three flat muscles
- Muscle fibers run transversely (horizontally)
- The lower fibers parallel the internal oblique, and together their fused lower margins form the conjoint tendon (inguinal falx), which inserts onto the pubic crest and pectineal line, reinforcing the posterior wall of the inguinal canal medially
Rectus Abdominis
- A long, flat paired vertical muscle extending the full length of the anterior abdominal wall
- Separated from its contralateral counterpart by the linea alba in the midline
- Widens and thins as it ascends from the pubic symphysis to the costal margin
- Has 3-4 tendinous intersections (horizontal fibrous bands) crossing it - these are adherent to the anterior wall of the rectus sheath (not the posterior wall), and produce the visible "six-pack" in individuals with developed musculature
- Enclosed within the rectus sheath (see below)
Pyramidalis
- A small, triangular muscle, may be absent in up to 20% of people
- Anterior to the lower rectus abdominis
- Has its base on the pubis; apex inserts into the lower linea alba
- Function: tenses the linea alba
4. Rectus Sheath
The rectus abdominis is enclosed in a fibrous sheath formed by the interlocking aponeuroses of the three flat muscles. Its composition differs above and below the arcuate line (semicircular line of Douglas), located midway between the umbilicus and pubic symphysis.
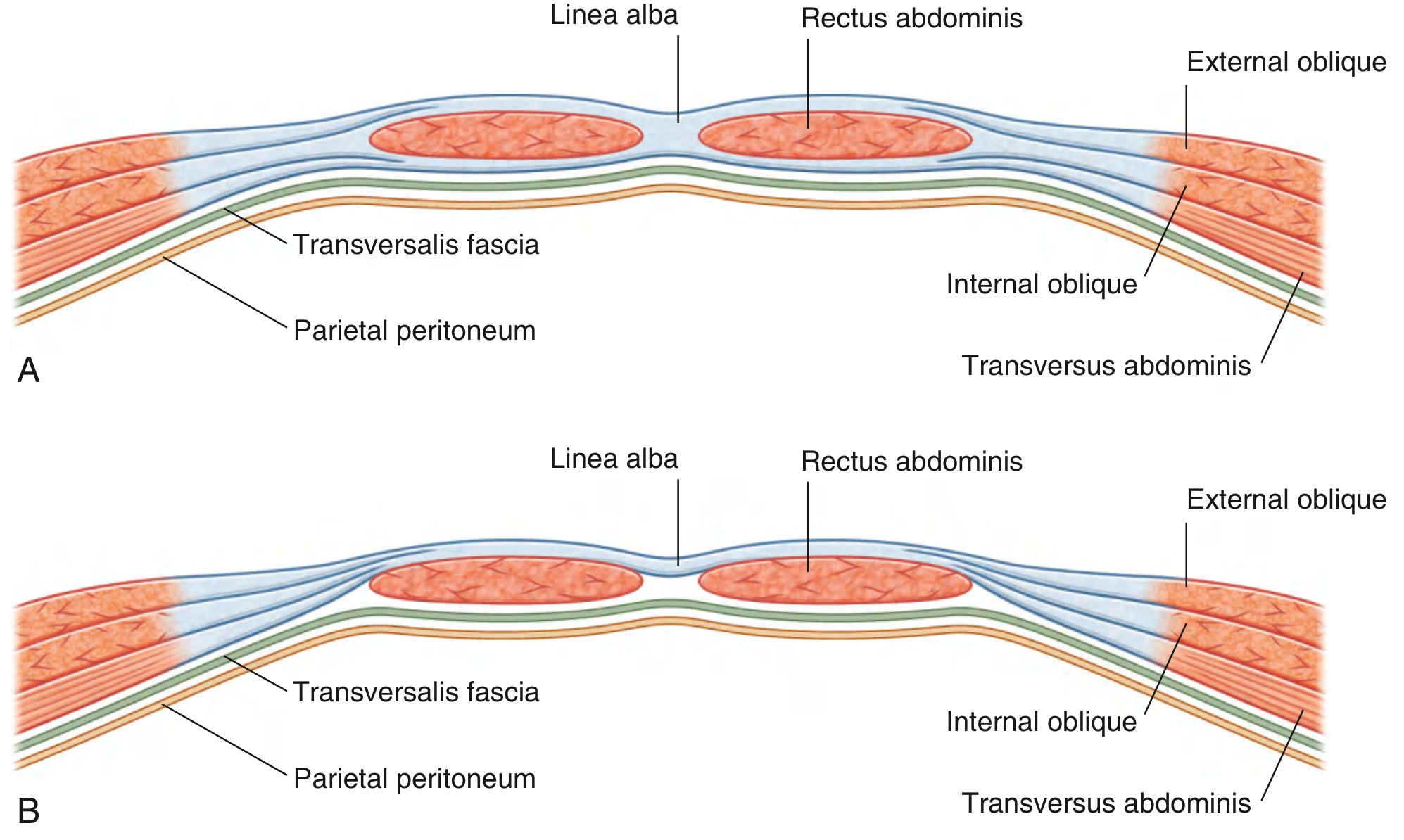
Fig. 4.33 - (A) Above the arcuate line; (B) Below the arcuate line
Above the Arcuate Line (upper 3/4 of rectus abdominis)
- Anterior wall: aponeurosis of external oblique + anterior lamina of internal oblique aponeurosis
- Posterior wall: posterior lamina of internal oblique aponeurosis + aponeurosis of transversus abdominis
Below the Arcuate Line (lower 1/4 of rectus abdominis)
- All three aponeuroses pass anterior to the rectus muscle
- There is no posterior wall of the rectus sheath
- The posterior surface of the rectus abdominis is in direct contact with the transversalis fascia
The arcuate line marks this abrupt transition and appears as a curved arch of fibers on the inner surface of the rectus sheath.
Contents of the rectus sheath: rectus abdominis, pyramidalis, superior and inferior epigastric vessels, lymphatics, and the terminal portions of the lower intercostal nerves (T7-T12).
5. Linea Alba
- A tendinous median raphe (band) formed by the decussating fibers of the three aponeuroses from both sides
- Extends from the xiphoid process to the pubic symphysis
- Above the umbilicus: about 2-3 cm wide (making it a site for midline surgical incisions)
- Below the umbilicus: narrow and almost cord-like
6. Linea Semilunaris
- The curved line along the lateral border of the rectus abdominis, visible on the surface as a slightly curved groove
- Represents the lateral edge of the rectus sheath
7. Transversalis Fascia
- A deep fascial layer lining the internal surface of the transversus abdominis
- Part of a continuous fascial lining of the entire abdominal cavity (also called the endoabdominal fascia)
- It is deficient posteriorly at the deep inguinal ring (a funnel-shaped evagination where it forms the innermost covering of the spermatic cord)
8. Extraperitoneal Fascia
- Lies between the transversalis fascia and the parietal peritoneum
- Contains variable amounts of fat
- The portion toward the anterior abdominal wall is termed preperitoneal fat (important in laparoscopic hernia repair)
- Posteriorly it is abundant around the kidneys (perirenal fat) and along the great vessels
9. Parietal Peritoneum
- The innermost layer - a thin serous membrane
- Lines the walls of the abdominal cavity
- Reflects onto viscera as visceral peritoneum
- On the inner surface of the anterior abdominal wall, the peritoneum raises five vertical folds (peritoneal folds) converging toward the umbilicus:
- Median umbilical fold (midline) - over the urachus remnant (median umbilical ligament)
- Medial umbilical folds (one on each side) - over the obliterated umbilical arteries
- Lateral umbilical folds (one on each side) - over the inferior epigastric vessels
These folds create recesses between them, which are relevant to hernia types (fossae).
Innervation of the Anterior Abdominal Wall
The skin, muscles, and parietal peritoneum are supplied by T7 to T12 and L1 spinal nerves (anterior rami).
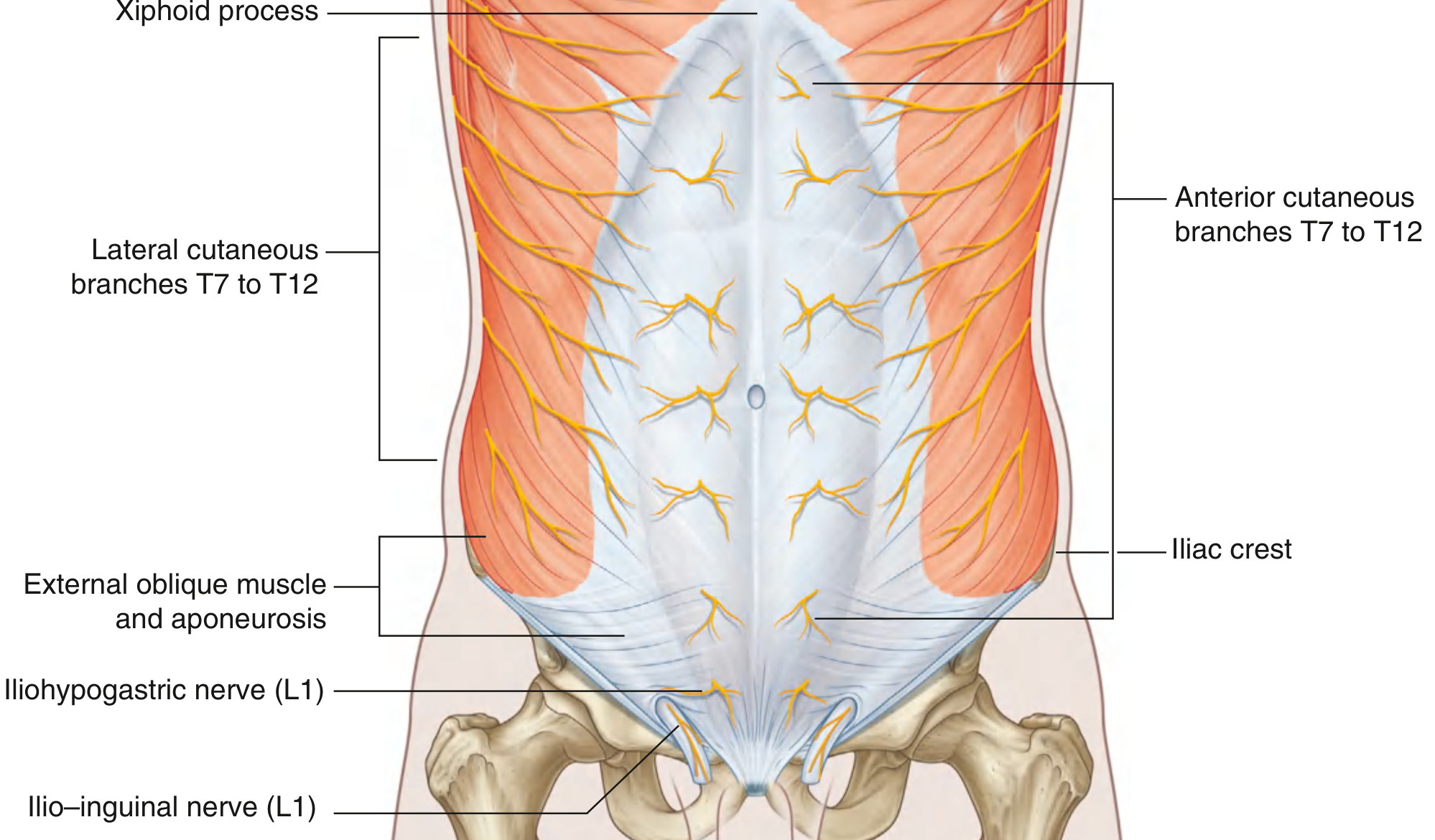
Fig. 4.36 - Innervation showing lateral and anterior cutaneous branches from T7-T12, with iliohypogastric and ilio-inguinal nerves (L1) inferiorly
- Intercostal nerves T7-T11 leave their intercostal spaces, cross the costal margin, enter the abdominal wall between the internal oblique and transversus abdominis, then pierce the rectus sheath to end as anterior cutaneous branches
- T12 (subcostal nerve) runs below rib XII
- L1 contributes two important nerves:
- Iliohypogastric nerve - supplies the skin of the hypogastric (suprapubic) region
- Ilio-inguinal nerve - passes through the inguinal canal and exits the superficial ring; supplies the anterior scrotum/labia majora and medial thigh
Dermatomes
| Level | Region supplied |
|---|---|
| T6 | Skin over xiphoid |
| T7-T9 | Skin from xiphoid to just above umbilicus |
| T10 | Skin around umbilicus |
| T11-T12 | Skin from just below umbilicus toward pubis |
| L1 | Inguinal and suprapubic regions, anterior scrotum/labia |
Blood Supply
Arterial Supply
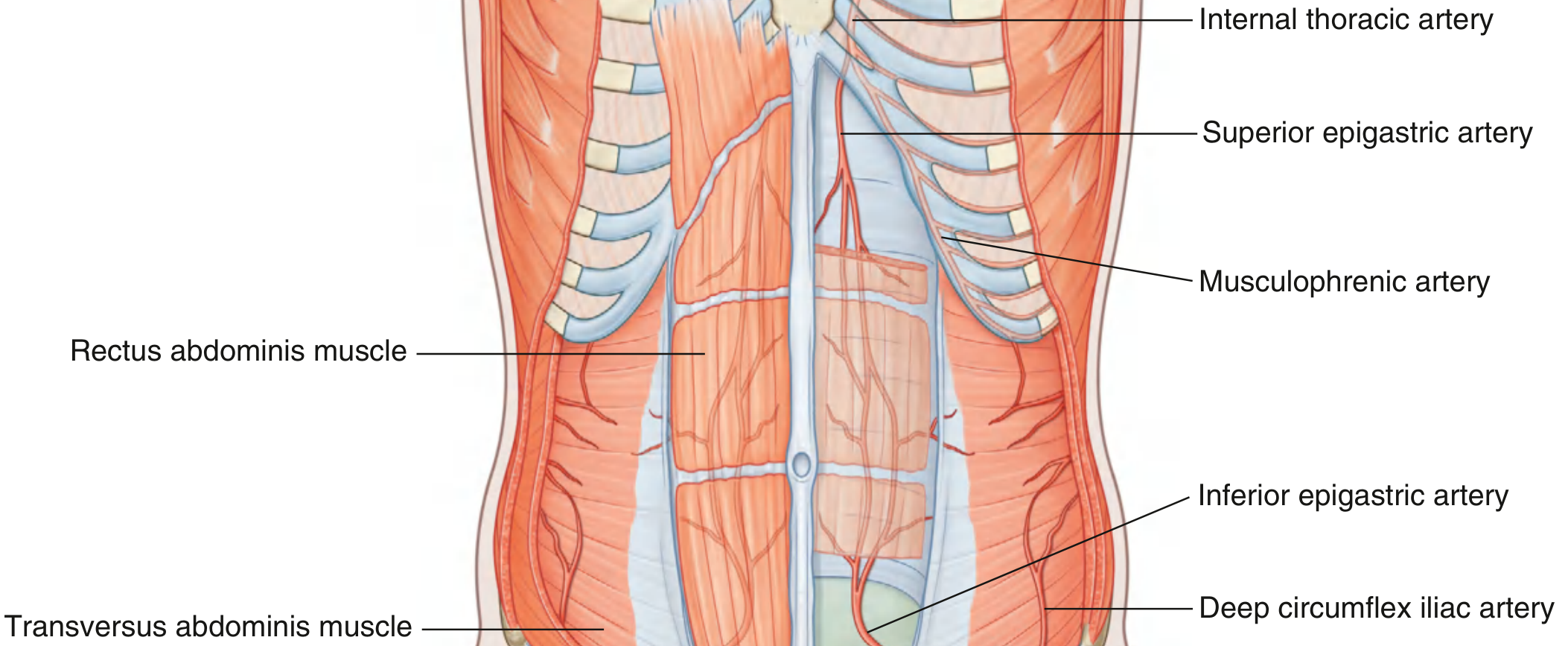
Fig. 4.40 - Superior and inferior epigastric arteries, musculophrenic artery, and deep circumflex iliac artery
Superficial arteries:
- Superior part: branches of musculophrenic artery (terminal branch of internal thoracic artery)
- Inferior part: superficial epigastric artery (medial) and superficial circumflex iliac artery (lateral) - both branches of the femoral artery
Deep arteries:
- Superior epigastric artery - terminal branch of the internal thoracic artery; enters the rectus sheath superiorly, runs posterior to the rectus abdominis
- Inferior epigastric artery - branch of the external iliac artery; enters the rectus sheath at the arcuate line, runs posterior to the rectus abdominis
- The superior and inferior epigastric arteries anastomose with each other within the rectus sheath, forming an important collateral pathway
- Lateral wall: branches of the 10th and 11th intercostal arteries and the subcostal artery
- Deep circumflex iliac artery - branch of the external iliac artery, supplies the lower lateral wall
Clinical note: The inferior epigastric artery is an important landmark during laparoscopic surgery. Lateral to it = direct hernia site; medial to it = indirect hernia site.
Venous Drainage
Veins follow the arteries and carry the same names. The thoracoepigastric veins (tributaries linking the axillary vein with the femoral vein via superficial abdominal veins) provide a collateral pathway between the superior and inferior vena caval systems. These veins become dilated in portal hypertension or inferior vena cava obstruction, producing the clinical sign of caput medusae (radiating around the umbilicus).
Lymphatic Drainage
- Above the umbilicus: superficial lymphatics drain upward to the axillary lymph nodes
- Below the umbilicus: superficial lymphatics drain downward to the superficial inguinal lymph nodes
- Deep lymphatics follow the deep arteries:
- Along the internal thoracic artery → parasternal nodes
- Along the abdominal aorta → lumbar (para-aortic) nodes
- Along the external iliac artery → external iliac nodes
The Inguinal Region (Groin)
The inguinal region is the junction between the anterior abdominal wall and the thigh. It represents a developmental weak point in the abdominal wall created during gonadal descent.
Inguinal Canal
A 4 cm long oblique passage through the lower anterior abdominal wall, running from the deep (internal) inguinal ring to the superficial (external) inguinal ring.
- Deep inguinal ring: a funnel-shaped opening in the transversalis fascia, located midway between the ASIS and pubic symphysis, just lateral to the inferior epigastric vessels. It is the entry point.
- Superficial inguinal ring: a triangular gap in the external oblique aponeurosis, just superolateral to the pubic tubercle. It is the exit point.
Walls of the Inguinal Canal
| Wall | Structure |
|---|---|
| Anterior wall | External oblique aponeurosis (plus internal oblique laterally) |
| Posterior wall | Transversalis fascia (plus conjoint tendon medially) |
| Roof (superior) | Arching fibers of internal oblique and transversus abdominis |
| Floor (inferior) | Inguinal ligament (infolded external oblique aponeurosis) |
Contents of the Inguinal Canal
- In males: spermatic cord (ductus deferens, testicular artery, pampiniform venous plexus, lymphatics, autonomic nerves, ilioinguinal nerve) + cremaster muscle
- In females: round ligament of the uterus + ilio-inguinal nerve
Coverings of the Spermatic Cord (from outside in)
These are derived from the layers of the abdominal wall as the processus vaginalis passed through:
- External spermatic fascia (from external oblique aponeurosis)
- Cremasteric fascia and cremaster muscle (from internal oblique)
- Internal spermatic fascia (from transversalis fascia)
Inguinal Triangles and Hernia Types
The Hesselbach's triangle (inguinal triangle) is bounded by:
- Medially: lateral border of rectus abdominis
- Laterally: inferior epigastric vessels
- Inferiorly: inguinal ligament
| Hernia Type | Relation to Inferior Epigastric Vessels | Passes Through |
|---|---|---|
| Indirect inguinal | Lateral | Deep inguinal ring → inguinal canal → superficial ring (congenital, via processus vaginalis remnant) |
| Direct inguinal | Medial (through Hesselbach's triangle) | Directly through posterior wall of inguinal canal (acquired weakness) |
| Femoral | Below inguinal ligament | Femoral canal (not the inguinal canal) |
Umbilicus
The umbilicus is a fibromuscular scar representing the former attachment of the umbilical cord. It is located in the linea alba at approximately the L3-L4 level (T10 dermatome). The underlying structures passing through the umbilicus in fetal life include:
- Umbilical vein (→ ligamentum teres hepatis)
- Two umbilical arteries (→ medial umbilical ligaments)
- Urachus (→ median umbilical ligament/fold)
- Vitellointestinal duct (normally obliterated; persistence → Meckel's diverticulum)
Summary of Surgical Significance
| Structure | Clinical Importance |
|---|---|
| Scarpa's fascia fusion with fascia lata | Limits spread of urine/blood in pelvic injuries |
| Arcuate line | No posterior rectus sheath below it - relevant in TAPP hernia repair |
| Inferior epigastric artery | Landmark for direct vs. indirect hernia; avoid during laparoscopy |
| Linea alba | Site of midline (median) laparotomy incision |
| T10 dermatome (umbilicus) | Referred pain from the appendix/small bowel |
| Hesselbach's triangle | Site of direct inguinal hernias |
| Deep inguinal ring | Entry of indirect inguinal hernias |
| Conjoint tendon | Reinforces posterior wall of inguinal canal medially; used in hernia repairs |
Gray's Anatomy for Students, pp. 337-350 | General Anatomy and Musculoskeletal System (THIEME Atlas of Anatomy), pp. 196-213
What are the types of abdominal wall hernias and their differences?
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the information needed. Let me compile the comprehensive answer.
Types of Abdominal Wall Hernias and Their Differences
Sources: Bailey and Love's Short Practice of Surgery, 28th Edition; Gray's Anatomy for Students; General Anatomy and Musculoskeletal System (THIEME Atlas)
Definition
A hernia is an abnormal protrusion of an organ or tissue through an opening in the layer that normally confines it. As abdominal hernias push from inside outward, they typically take with them all the coverings of the abdominal wall, though these may be thinned and attenuated. Not all hernias have a peritoneal sac - many epigastric hernias contain only extraperitoneal fat initially.
Classification Overview
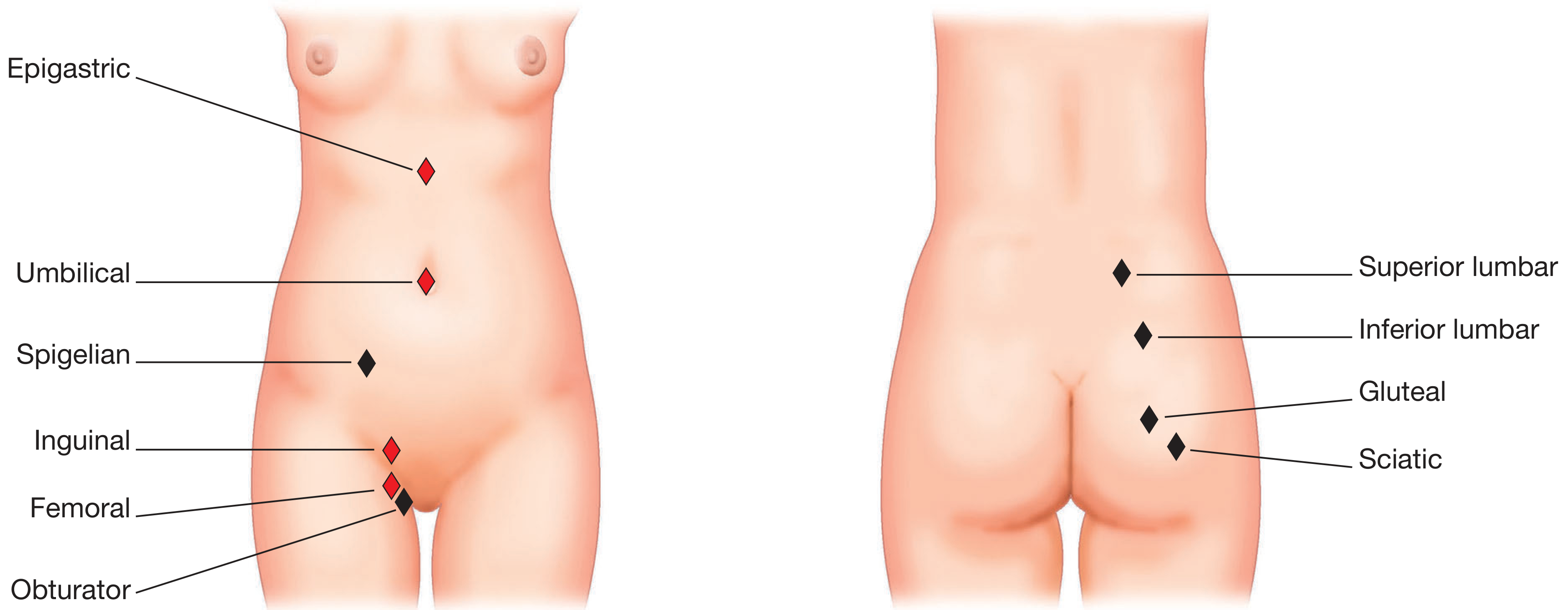
Fig. 64.9 - Sites of abdominal wall hernias: common (red), rare (black). Front: epigastric, umbilical, Spigelian, inguinal, femoral, obturator. Back: superior and inferior lumbar, gluteal, sciatic.
Hernias are broadly divided into:
| Category | Types |
|---|---|
| Groin hernias | Indirect inguinal, Direct inguinal, Femoral |
| Primary ventral hernias | Umbilical, Epigastric, Spigelian, Lumbar, Traumatic |
| Secondary ventral hernias | Incisional, Parastomal |
| Rare/pelvic hernias | Obturator, Sciatic, Gluteal, Perineal |
Anatomical Causes of Hernia Formation
Areas of weakness fall into four categories:
- Absence of muscle (natural muscular deficiency) - e.g., lumbar triangles, posterior inguinal canal
- Natural defects where structures enter/leave the abdomen - e.g., inguinal canal, femoral canal, umbilicus, esophageal hiatus
- Developmental abnormalities - e.g., patent processus vaginalis
- Disruption of the wall by injury or surgery - e.g., incisional hernia
1. INGUINAL HERNIAS
The most common hernia overall; about 10x more common in men than in women.

Fig. 64.10 - Showing the sacs of indirect inguinal, direct inguinal, and femoral hernias in close anatomical relationship to the inferior epigastric vessels and femoral vessels
Direct Inguinal Hernia ("Medial" Hernia)
| Feature | Detail |
|---|---|
| Mechanism | Acquired weakness in the posterior wall of the inguinal canal (Hesselbach's triangle) |
| Relation to inferior epigastric vessels | Medial to the inferior epigastric vessels |
| Defect site | Directly through the transversalis fascia within Hesselbach's triangle (NOT through the deep inguinal ring) |
| Hesselbach's triangle boundaries | Medially: rectus abdominis; laterally: inferior epigastric vessels; inferiorly: inguinal ligament |
| Age/sex | Older males; acquired, not congenital |
| Path | Bulges directly anteriorly through the posterior wall of the canal; usually does NOT enter the scrotum |
| Sac coverings | Transversalis fascia, external oblique aponeurosis (no internal spermatic fascia, as it does not pass through the deep ring) |
| Reduction by deep ring pressure | NOT controlled - hernia appears medially despite finger at deep ring |
| Risk of strangulation | Lower than indirect (wide neck) |
| Aetiology | Raised intraabdominal pressure, collagen disorders, heavy lifting, aging |
Indirect Inguinal Hernia ("Lateral" or "Oblique" Hernia)
| Feature | Detail |
|---|---|
| Mechanism | Passes through the deep (internal) inguinal ring - a defect in the transversalis fascia - and travels the full length of the inguinal canal |
| Relation to inferior epigastric vessels | Lateral to the inferior epigastric vessels |
| Defect site | Deep inguinal ring (midway between ASIS and pubic tubercle, approximately 2-3 cm above the femoral artery) |
| Origin | Patent or partially patent processus vaginalis - hence can be congenital or acquired |
| Age/sex | Any age; the only type seen in children and neonates (always congenital at that age); also the most common inguinal hernia in adults |
| Path | Follows the spermatic cord obliquely through the canal; can descend into the scrotum (complete hernia) |
| Sac coverings | Internal spermatic fascia (from transversalis fascia), cremasteric fascia (from internal oblique), external spermatic fascia (from external oblique) |
| Reduction by deep ring pressure | Controlled - hernia does not reappear when finger occludes the deep ring |
| Risk of strangulation | Higher than direct (narrow neck at deep ring) |
Direct vs. Indirect: Key Comparison Table
| Feature | Direct | Indirect |
|---|---|---|
| Age | Older | Any age |
| Origin | Acquired | Congenital / acquired |
| Path | Directly through Hesselbach's triangle | Through deep inguinal ring → along canal |
| Relation to inf. epigastric | Medial | Lateral |
| Enters scrotum? | Rarely | Commonly |
| Sac coverings | 2 (transversalis fascia, ext. oblique apon.) | 3 (internal + cremasteric + external spermatic fasciae) |
| Strangulation risk | Lower (wide neck) | Higher (narrow neck) |
| Deep ring pressure test | Not controlled | Controlled |
Pantaloon hernia: When both a direct and an indirect hernia coexist on the same side, straddling the inferior epigastric vessels - the appearance resembles a pair of trousers (pantaloon).
2. FEMORAL HERNIA
| Feature | Detail |
|---|---|
| Location | Through the femoral canal - below and lateral to the pubic tubercle, below the inguinal ligament |
| Boundaries of femoral canal | Laterally: femoral vein; anteriorly: inguinal ligament; posteriorly: iliopectineal (Cooper's) ligament; medially: lacunar (Gimbernat's) ligament |
| Sex | More common in women (wider female pelvis enlarges the femoral canal); overall 3rd most common hernia |
| Age | Thin, elderly women most commonly affected |
| Key danger | The lacunar ligament has a sharp, unyielding medial edge - this makes reduction difficult and strangulation rates extremely high (~50% present as emergency with strangulation) |
| Clinical appearance | Swelling below and lateral to the pubic tubercle (cf. inguinal hernia which is above and medial to pubic tubercle) |
| Nodes | Contains the node of Cloquet (lymph node) in normal anatomy |
| Diagnosis | Often missed; can be confused with a lipoma, enlarged lymph node, or femoral artery aneurysm |
| Management | Surgery is mandatory (cannot be safely watched due to strangulation risk) |
Key distinction from inguinal: Inguinal hernias emerge above and medial to the pubic tubercle. Femoral hernias emerge below and lateral to the pubic tubercle, below the inguinal ligament.
3. UMBILICAL HERNIA
Infantile / Congenital Umbilical Hernia
- Occurs in up to 10% of infants (higher in premature and Black infants)
- Due to delayed closure of the umbilical ring after cord separation
- Appears within weeks of birth; classic conical shape, enlarges on crying
- 95% resolve spontaneously by age 2 - watchful waiting is standard
- Surgery only if persists past 2 years or has a large defect
Adult Umbilical / Paraumbilical Hernia
- Defect is through (umbilical) or just adjacent to (paraumbilical) the umbilical scar in the linea alba
- Risk factors: obesity, multiple pregnancies, chronic ascites (e.g., liver cirrhosis), raised intraabdominal pressure
- More common in women; typically in overweight individuals
- Contents: extraperitoneal fat in small hernias; omentum, small/large bowel in larger ones
- Prone to incarceration (irreducibility), obstruction, and strangulation due to relatively narrow neck
- Surgery advised when bowel is present; open (Mayo repair) or laparoscopic with mesh
4. EPIGASTRIC HERNIA
| Feature | Detail |
|---|---|
| Location | Through the linea alba between the xiphoid process and umbilicus |
| Mechanism | Transverse split in the midline raphe; defect usually <1 cm and elliptical in shape |
| Contents | Almost always extraperitoneal fat only; rarely has a peritoneal sac; bowel very uncommon |
| Multiplicity | Multiple defects common along the linea alba; "recurrence" after repair often indicates a missed second hernia |
| Demographics | Often fit healthy men; also overweight men/women, especially after pregnancies |
| Symptoms | Disproportionately painful for their small size (fat becomes nipped in narrow neck - partial strangulation); may resemble a lipoma; may have cough impulse |
| Reducibility | Often irreducible due to narrow neck |
| Danger | Low risk of bowel strangulation; but chronic fat pain is common |
5. SPIGELIAN HERNIA
| Feature | Detail |
|---|---|
| Location | Through a defect in the Spigelian fascia (aponeurosis of transversus abdominis) at the Spigelian line (linea semilunaris - lateral border of rectus sheath) |
| Level | Most commonly just below the umbilicus, near the edge of the rectus sheath; most are ABOVE the arcuate line despite a common misconception |
| Path | Defect in transversus abdominis → spreads deep to the external oblique aponeurosis (hence called an interstitial or interparietal hernia - hidden between layers) |
| Demographics | Equal sex distribution; mostly elderly; rare but underdiagnosed |
| Contents | Young patients: extraperitoneal fat only; Older patients: peritoneal sac, can become large |
| Diagnosis | Often difficult to palpate because the hernia is hidden under intact external oblique; CT or upright ultrasound is needed |
| Risk | Narrow fibrous neck → high risk of strangulation; surgery recommended once diagnosed |
6. INCISIONAL HERNIA
| Feature | Detail |
|---|---|
| Definition | Hernia through a defect in the musculofascial layers at a postoperative scar |
| Incidence | 10-50% of laparotomy incisions; 1-5% of laparoscopic port sites |
| Risk factors | Obesity, malnutrition, immunosuppression, steroid therapy, chronic cough, wound infection, poor closure technique, collagen disorders, cancer |
| Pathology | Begins as disruption of the muscular/fascial repair; slowly enlarges as scar tissue gives way under intraabdominal pressure |
| Location | Anywhere along a previous surgical scar (midline most common) |
| Contents | Fat, omentum, or bowel |
| Symptoms | Expanding bulge along scar; pain on straining; episodes of obstruction |
| Risk | Can become very large; "loss of domain" when bowel habitually resides in the sac |
| Repair | Mesh reinforcement essential for most; open or laparoscopic (TAPP/TEP modified) |
7. LUMBAR HERNIA
Hernia through the lumbar (posterior) abdominal wall:
- Superior lumbar triangle (Grynfeltt's triangle): bounded by the 12th rib, quadratus lumborum, and internal oblique - larger and more common
- Inferior lumbar triangle (Petit's triangle): bounded by the iliac crest, latissimus dorsi, and external oblique
- Can be primary (spontaneous - rare) or secondary (post-surgical/traumatic, more common - e.g., after open nephrectomy causing denervation)
- Contains retroperitoneal fat; bowel herniation possible
- A "pseudohernia" (diffuse muscle bulge without true defect) can occur after denervation
8. TRAUMATIC HERNIA
Three subtypes:
- Through stab wound sites (effectively an incisional hernia)
- Through splits or tears in the abdominal muscles after blunt trauma
- Diffuse abdominal bulging (pseudohernia) from nerve injury/denervation after rib fractures or trauma
Diagnosis relies on the non-anatomical location and trauma history. CT defines the tissue layers damaged.
9. RARE HERNIAS
| Hernia | Location | Notes |
|---|---|---|
| Obturator hernia | Through the obturator foramen, below the inguinal ligament | Rare; thin elderly women; presents with bowel obstruction; Howship-Romberg sign (medial thigh pain on hip extension/internal rotation) |
| Sciatic hernia | Through the greater or lesser sciatic foramen | Very rare; can compress sciatic nerve |
| Gluteal hernia | Through the greater sciatic foramen above piriformis | Extremely rare |
| Perineal hernia | Through the pelvic floor | Post-abdominoperineal excision |
| Parastomal hernia | Around a stoma through the abdominal wall | Common complication after colostomy/ileostomy |
| Richter's hernia | Only one wall of the bowel is caught in the sac | Can strangulate without complete bowel obstruction |
| Littre's hernia | Contains a Meckel's diverticulum | High strangulation risk |
| Maydl's hernia | Two loops of bowel in sac (W-shaped) | Middle loop strangulates within abdomen |
Hernia Terminology
| Term | Definition |
|---|---|
| Reducible | Contents can be returned to the abdomen |
| Irreducible / Incarcerated | Contents cannot be reduced; not necessarily obstructed |
| Obstructed | Bowel in sac is obstructed but blood supply is intact |
| Strangulated | Blood supply to hernia contents is compromised; surgical emergency |
| Sliding hernia | Part of the wall of the sac is formed by a viscus (e.g., caecum, sigmoid colon, bladder) |
Summary Comparison: Groin Hernias at a Glance
| Feature | Indirect Inguinal | Direct Inguinal | Femoral |
|---|---|---|---|
| Sex | M >> F | M >> F | F > M |
| Age | Any (including children) | Elderly | Elderly women |
| Origin | Congenital/acquired | Acquired | Acquired |
| Location relative to inf. epigastric | Lateral | Medial | Below inguinal ligament |
| Location relative to pubic tubercle | Above & medial | Above & medial | Below & lateral |
| Passes through deep ring? | Yes | No | No |
| Enters scrotum? | Yes (if complete) | Rarely | Never |
| Strangulation risk | Moderate-high | Low | Very high |
| Most common overall | Most common | 2nd most common | 3rd most common |
Bailey and Love's Short Practice of Surgery, 28th Edition, pp. 1080-1100 | Gray's Anatomy for Students, pp. 349-358
This is a shared conversation. Sign in to Orris to start your own chat.