Heart failure basic to clinical
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching PubMed
"heart failure" AND "treatment guidelines"
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Heart Failure: Basic to Clinical
A complete, structured overview drawn from Robbins & Cotran Pathologic Basis of Disease, Lippincott Illustrated Reviews: Pharmacology, Katzung's Basic and Clinical Pharmacology, and Braunwald's Heart Disease.
1. Definition
Heart failure (HF) is a clinical syndrome in which the heart is unable to provide adequate perfusion to meet the metabolic requirements of peripheral tissues. The inadequate cardiac output is nearly always accompanied by increased congestion of the venous circulation - hence the old term "congestive heart failure" (CHF). Normal cardiac output is approximately 5 L/min (70 kg reference); HF typically represents a fall below this baseline.
- Robbins & Cotran Pathologic Basis of Disease, p. 498
- Katzung's Basic and Clinical Pharmacology, 16e, p. 334
2. Etiology and Classification
By Ejection Fraction
| Type | EF | Mechanism |
|---|---|---|
| HFrEF (reduced EF) | < 40% | Systolic dysfunction - impaired contraction |
| HFmrEF (mildly reduced) | 40-49% | Mixed |
| HFpEF (preserved EF) | ≥ 50% | Diastolic dysfunction - impaired relaxation/filling |
By Output
- Low-output failure (most common): IHD, cardiomyopathy, hypertension, valvular disease
- High-output failure (rare): Hyperthyroidism, beriberi, severe anemia, arteriovenous shunts - responds poorly to standard HF drugs; treat the underlying cause
By Side
- Left-sided HF: IHD, hypertension, aortic/mitral valve disease, primary cardiomyopathy
- Right-sided HF: Most often caused by left-sided HF; also pulmonary disease (cor pulmonale), pulmonary hypertension
In practice, biventricular HF is most common in chronic decompensation.
3. Basic Pathophysiology
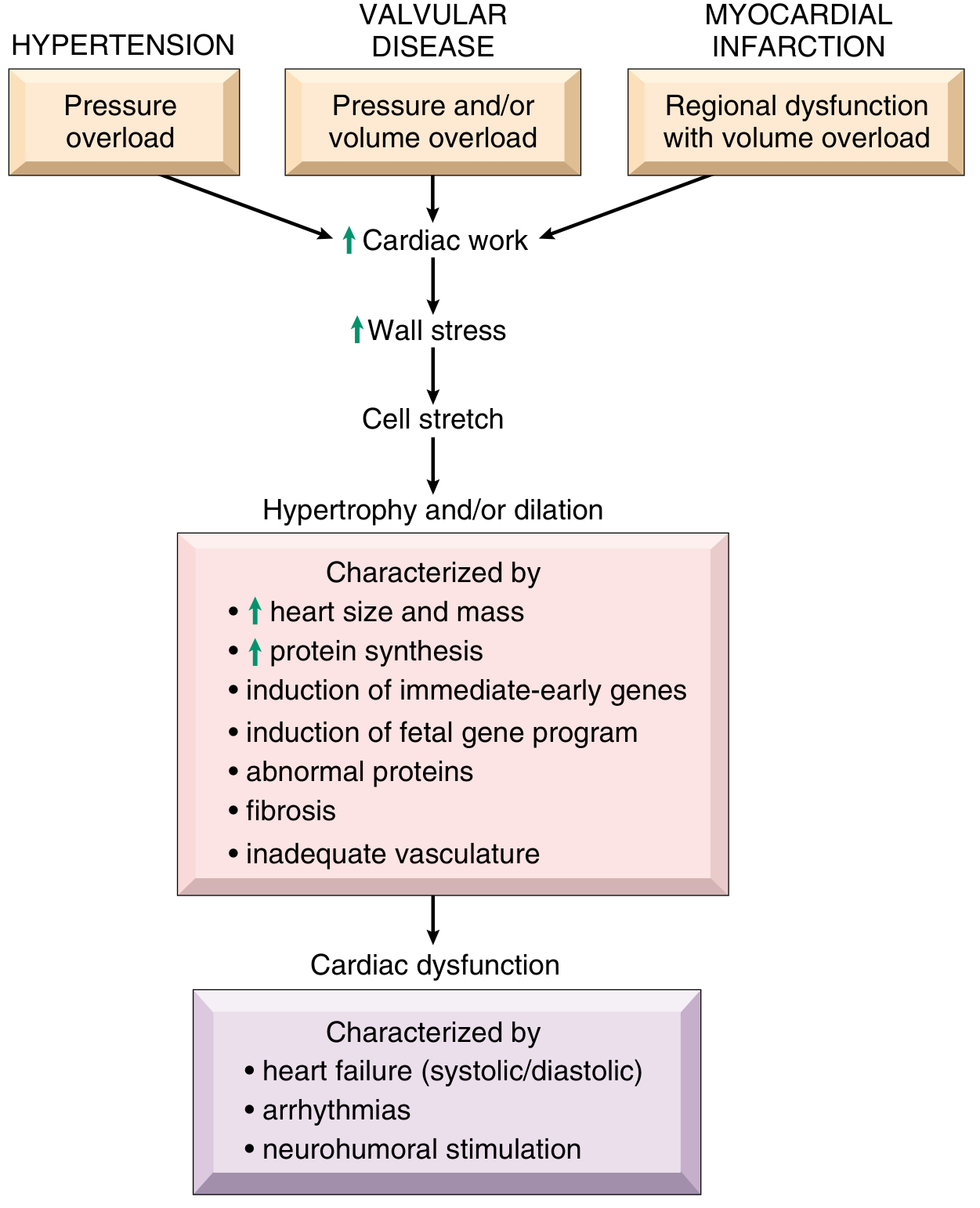
3a. Cardiac Hypertrophy - the Initial Response
A sustained increase in mechanical work causes myocytes to hypertrophy. The pattern depends on the stimulus:
- Pressure overload (hypertension, aortic stenosis): new sarcomeres assemble in parallel → concentric hypertrophy (increased wall thickness, normal cavity size)
- Volume overload (valvular regurgitation): new sarcomeres assemble in series → eccentric hypertrophy/dilation
Hypertrophied myocytes show enlarged nuclei, increased protein synthesis, and induction of a "fetal gene program." Critically, hypertrophy is not accompanied by a proportional increase in capillary density, creating relative ischemia. Over time, myocytes die by apoptosis at an accelerated rate.
3b. The Four Determinants of Cardiac Performance (Frank-Starling Framework)
- Preload: End-diastolic fiber length/filling pressure. The ascending limb of the Frank-Starling curve (<15 mmHg) shows increasing stroke work with filling; beyond ~20-25 mmHg, pulmonary congestion occurs. Preload is increased in HF due to volume/sodium retention.
- Afterload: Ventricular wall stress at the onset of ejection (largely arterial resistance). Increased in HF via sympathetic/RAAS-driven vasoconstriction - this further reduces ejection fraction.
- Contractility (inotropy): Intrinsic myocardial strength at a given preload/afterload. Force of contraction is directly proportional to free cytosolic Ca²⁺.
- Heart rate: Sympathetic-driven tachycardia initially compensates, but long-term chronic elevation is harmful.
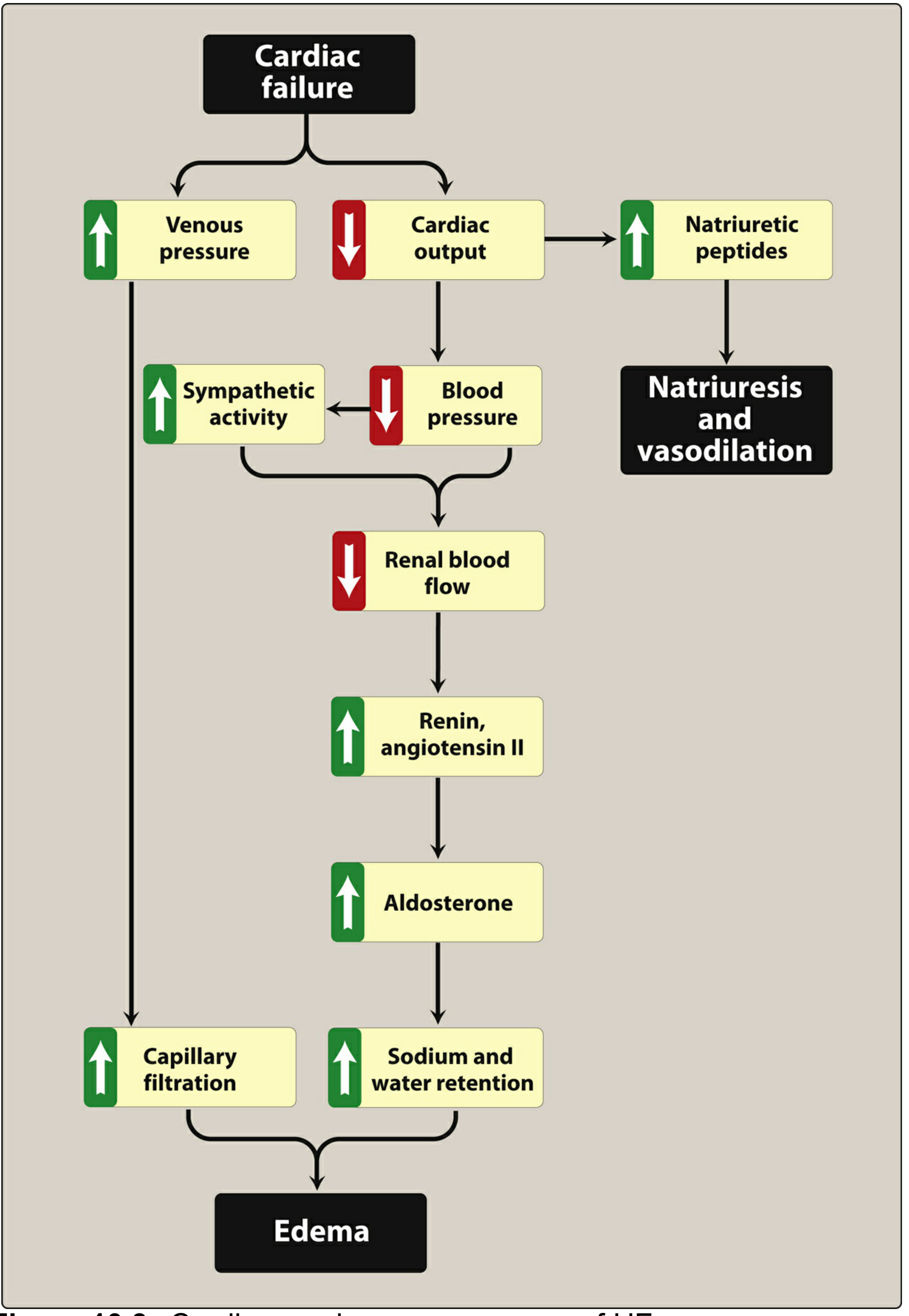
3c. Neurohumoral Compensatory Mechanisms
Six major compensatory responses are activated - three are ultimately detrimental:
| Mechanism | Initial Effect | Long-term Harm |
|---|---|---|
| 1. Sympathetic activation | ↑HR, ↑contractility, vasoconstriction | β-receptor downregulation, arrhythmias, apoptosis, RyR Ca²⁺ leak, ↑afterload |
| 2. RAAS activation | Na⁺/water retention (preload), vasoconstriction | Myocardial fibrosis, remodeling, pulmonary/peripheral edema |
| 3. Natriuretic peptides (ANP, BNP) | Vasodilation, natriuresis, inhibit renin/aldosterone | Resistance develops (pre-, receptor-, post-receptor mechanisms) |
| 4. Myocardial hypertrophy | Increased wall mass helps maintain output | Ischemia, arrhythmias, impaired diastolic filling, apoptosis |
| 5. Inflammation & oxidative stress | Tissue repair signals | Mitochondrial dysfunction, Ca²⁺ dysregulation, myocyte death |
| 6. Resistance to natriuretic peptides | - | Vasoconstriction, fibrosis, reduced renal blood flow |
The vicious cycle: Reduced CO → baroreceptor reset → ↑sympathetic/RAAS → vasoconstriction → ↑afterload → ↓EF → further ↓CO.
3d. Calcium Handling Abnormalities
In the failing heart:
- SERCA (SR Ca²⁺-ATPase) activity is impaired → Ca²⁺ reuptake into SR is reduced
- RyR channels are hyperphosphorylated (CaMKII, PKA) → SR Ca²⁺ leaks during diastole
- Phospholamban regulation is disrupted
- Net result: cytosolic Ca²⁺ overload during diastole (stiffness) and reduced Ca²⁺ transient during systole (reduced contractility)
These are targets for future drug development.
4. Morphology and Organ Effects
Left-Sided HF
Heart: LV hypertrophy and dilation; LA dilation; ↑risk of AF and atrial thrombus (especially in the appendage).
Lungs (backward failure): Perivascular/interstitial edema → alveolar edema. Extravasated RBCs are phagocytosed by macrophages → hemosiderin-laden "heart failure cells" - a pathognomonic sign on histology.
Pleural cavities: Serous pleural effusions (bilateral, typically right > left).
Clinical symptoms progression:
- Exertional dyspnea → orthopnea → paroxysmal nocturnal dyspnea (PND) → acute pulmonary edema
Forward failure effects: Decreased renal perfusion → pre-renal azotemia; cerebral hypoperfusion → confusion/cognitive changes.
Right-Sided HF
Liver: Congestive hepatomegaly; "nutmeg liver" grossly (red-brown centrilobular congestion alternating with tan periportal zones); centrilobular necrosis with severe combined HF; cardiac cirrhosis in chronic cases.
Spleen: Congestive splenomegaly with platelet sequestration.
Gut: Bowel wall edema - may impair nutrient and drug absorption.
Peripheral: Pedal/pretibial edema (dependent), sacral edema in bedridden patients; severe cases → anasarca; pleural, pericardial, and peritoneal effusions/ascites.
Kidney: Greater azotemia than left-sided HF; greater fluid retention; peripheral edema.
- Robbins & Cotran Pathologic Basis of Disease, pp. 498-502
5. Clinical Features and Diagnosis
Symptoms
- LHF: Dyspnea on exertion, orthopnea, PND, cough, fatigue, decreased exercise tolerance
- RHF: Peripheral edema, abdominal distension (ascites), anorexia, RUQ discomfort (liver congestion)
- Both: Fatigue, weakness, tachycardia, cardiomegaly
Signs
- S3 gallop (ventricular filling sound - hallmark of systolic HF)
- S4 gallop (atrial contraction against stiff ventricle - diastolic dysfunction)
- Displaced apical impulse (cardiomegaly)
- Elevated JVP, hepatojugular reflux
- Bilateral basal crackles (pulmonary edema)
- Peripheral pitting edema
Key Investigations
| Test | Relevance |
|---|---|
| BNP / NT-proBNP | Released by ventricular myocytes under wall stress; low value has high negative predictive value for HF; tracks severity and response to therapy |
| Echocardiography | Gold standard - EF, wall motion, valve function, diastolic parameters, mural thrombus |
| ECG | LVH, ischemia, arrhythmias (AF very common) |
| CXR | Cardiomegaly, Kerley B lines, pulmonary vascular congestion, pleural effusions |
| BMP/CMP | Renal function (pre-renal azotemia), electrolytes (hyponatremia = poor prognosis), liver function |
6. Pharmacological Treatment
Treatment targets the neurohumoral vicious cycle. The current "fantastic four" for HFrEF are: ARNI + β-blocker + MRA + SGLT2 inhibitor.
6a. ACE Inhibitors / ARBs
- Block RAAS at ACE or AT1 receptor
- Reduce afterload, preload, prevent remodeling and myocyte hypertrophy
- ACE inhibitors: first-line; ARBs: used when ACEi not tolerated (dry cough, angioedema)
6b. ARNI - Sacubitril/Valsartan
- Sacubitril inhibits neprilysin (which degrades BNP, ANP, bradykinin) → ↑natriuretic peptides → natriuresis, vasodilation, anti-fibrosis
- Valsartan blocks AT1 receptor (offsets RAAS activation; prevents angioedema from dual bradykinin buildup)
- Shown superior to ACEi in the PARADIGM-HF trial
- Indication: Replace ACEi/ARB in symptomatic HFrEF on optimized β-blocker + ACEi/ARB
- Key caution: Must washout ACEi ≥36 hours before starting to avoid angioedema
6c. β-Blockers (bisoprolol, carvedilol, metoprolol succinate)
- Counterintuitive but proven: reduce chronic sympathetic overdrive, prevent β1 downregulation, reverse cardiac remodeling, decrease apoptosis, reduce arrhythmias
- Carvedilol is non-selective (β1, β2, α1 blockade); bisoprolol and metoprolol are β1-selective
- Start low, titrate gradually; avoid in acute decompensation until stable
6d. Mineralocorticoid Receptor Antagonists (Spironolactone, Eplerenone)
- Block aldosterone → prevent Na⁺ retention, myocardial hypertrophy, hypokalemia
- Spironolactone has off-target effects (gynecomastia, dysmenorrhea); eplerenone is MR-selective
- Indicated in symptomatic HFrEF; also for HFrEF post-MI; reduces hospitalizations in HFpEF
6e. SGLT2 Inhibitors (Dapagliflozin, Empagliflozin)
- Block SGLT2 in proximal tubule → glucosuria + natriuresis
- Cardioprotective mechanism: may involve NHE inhibition → prevents Ca²⁺ overload; selectively reduces interstitial fluid (less neurohormonal reflex activation vs. loop diuretics)
- Evidence: DAPA-HF (dapagliflozin) and EMPEROR-Reduced (empagliflozin) showed mortality/hospitalization benefit in HFrEF; also effective in HFpEF
- Indicated: Symptomatic HFrEF on optimized GDMT; also HFpEF
6f. Diuretics (Loop diuretics: furosemide, bumetanide, torsemide)
- Reduce preload and symptoms of volume overload (dyspnea, edema, orthopnea)
- Do NOT improve survival - use only for symptom control
- Thiazides for mild HF; loop diuretics for moderate-severe or renal insufficiency
6g. Vasodilators
- Hydralazine + isosorbide dinitrate: For patients intolerant of ACEi/ARB; fixed-dose combination shown to improve survival in African-American patients with HFrEF on GDMT; hydralazine has antioxidant properties that prevent nitrate tolerance
- Nitrates alone: Venodilators → reduce preload; useful for acute dyspnea/pulmonary edema
6h. HCN Channel Blocker - Ivabradine
- Blocks the If ("funny") current in the SA node → reduces heart rate without affecting contractility or BP
- For patients with HFrEF, EF ≤35%, sinus rhythm, HR ≥70 bpm on maximally tolerated β-blocker
6i. Soluble Guanylate Cyclase Stimulator - Vericiguat
- Stimulates sGC → ↑cGMP → vasodilation and anti-fibrosis
- Corrects the NO deficit in HF (oxidative stress inactivates endogenous NO)
- For high-risk HFrEF patients with recent worsening; less hypotension than traditional NO donors
6j. Inotropes (Acute/Refractory HF)
- Digoxin (cardiac glycoside): Inhibits Na⁺/K⁺-ATPase → ↑intracellular Na⁺ → ↑Ca²⁺ via NCX → ↑contractility; also vagotonic → slows AV conduction (useful in AF with HF). Narrow therapeutic index (0.5-0.9 ng/mL target). Does not improve mortality.
- Dobutamine (β1 agonist): For acute decompensated HF; short-term bridge
- Milrinone (PDE3 inhibitor): Inodilator; ↑cAMP → ↑inotropy + vasodilation
Summary Drug Table for HFrEF (GDMT)
| Drug Class | Example | Mortality Benefit |
|---|---|---|
| ARNI | Sacubitril/valsartan | Yes (replaces ACEi/ARB) |
| ACEi / ARB | Lisinopril / Losartan | Yes |
| β-Blocker | Carvedilol, Bisoprolol, Metoprolol succinate | Yes |
| MRA | Spironolactone, Eplerenone | Yes |
| SGLT2i | Dapagliflozin, Empagliflozin | Yes |
| Loop diuretic | Furosemide | Symptom relief only |
| Ivabradine | Ivabradine | Modest (hospitalizations) |
| Vericiguat | Vericiguat | Reduces hospitalizations |
| Hydralazine/ISDN | Fixed-dose combo | Yes (African-American HFrEF) |
7. Non-Pharmacological and Device Therapy
- Salt/fluid restriction: Reduce preload; 2 g/day sodium restriction is standard
- Cardiac resynchronization therapy (CRT): Biventricular pacing for patients with EF ≤35%, LBBB, QRS ≥150 ms in sinus rhythm; resynchronizes LV wall motion, improves EF and symptoms
- ICD (implantable cardioverter-defibrillator): EF ≤35% despite ≥3 months GDMT; reduces sudden cardiac death
- Ventricular assist devices (VADs): LVAD as bridge to transplant or destination therapy in refractory HF
- Cardiac transplantation: Gold standard for end-stage HF
- Pulmonary artery pressure monitoring (CardioMEMS): Reduces 30-day readmissions by guiding outpatient diuresis
- Exercise rehabilitation: Aerobic exercise promotes physiologic (beneficial) hypertrophy; reduces symptoms and hospitalizations
8. HFpEF - Special Considerations
HFpEF accounts for ~50% of HF and has been notoriously difficult to treat. Key features:
- EF ≥50%, symptoms and signs of HF, elevated filling pressures
- Mechanism: Diastolic dysfunction (impaired relaxation and filling); myocardial stiffness due to hypertrophy, fibrosis, and inflammation
- Driven by comorbidities: obesity, diabetes, hypertension, CKD, atrial fibrillation
- The Paulus-Tschope paradigm: Systemic inflammation from comorbidities → coronary microvascular endothelial inflammation → reduced NO → reduced cGMP → PKG hypoactivity → titin hypophosphorylation → increased myocardial stiffness
- Treatment: Primarily symptom control with diuretics; SGLT2i (dapagliflozin, empagliflozin) now shown to reduce hospitalizations in HFpEF; MRAs reduce hospitalizations; ARBs may provide modest benefit; ACEi/ARNI/β-blockers not proven to reduce mortality in pure HFpEF
9. Prognosis and Biomarkers
- BNP/NT-proBNP: Primary biomarker; elevated with any increase in wall stress; low BNP has very high negative predictive value to rule out HF
- Hyponatremia: Independent marker of poor prognosis (reflects maximal neurohormonal activation)
- Troponin: Chronic low-level elevation indicates ongoing myocyte death; prognostic
- NYHA Functional Class: I (no symptoms) → IV (symptoms at rest); guides therapy intensity
- 5-year mortality of symptomatic HF remains ~50%, similar to many malignancies, though improving with GDMT
Key Sources
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, pp. 498-502
- Lippincott Illustrated Reviews: Pharmacology, pp. 353-371
- Katzung's Basic and Clinical Pharmacology, 16e, pp. 334-345
- Braunwald's Heart Disease, 2-Vol Set
Recent Evidence
- Pharmacotherapy network meta-analysis (Tang et al., 2025 - PMID 38811344): Confirms the four-pillar GDMT (ARNI + β-blocker + MRA + SGLT2i) provides the greatest mortality benefit in HFrEF
- SGLT2i systematic review (Li et al., 2025 - PMID 40672365): Long-term SGLT2 inhibition also reduces arrhythmia burden in HF
This is a shared conversation. Sign in to Orris to start your own chat.