Flail chest 6 marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is the complete 6-mark answer:
Flail Chest
Definition
Flail chest is defined as the fracture of three or more adjacent ribs, each broken in two or more places (segmental fractures), creating an isolated, free-floating segment of the chest wall that loses its bony continuity with the rest of the thoracic cage. Some sources define it as two or more adjacent ribs broken at two points, producing the same mechanical consequence.
Etiology / Causes
- Blunt chest trauma - most common cause; typically road traffic accidents and falls
- Aggressive cardiopulmonary resuscitation
- Pathologic rib fractures (e.g., metastatic disease, osteoporosis)
- In children it is uncommon because the chest wall is more compliant; its presence in a child indicates a much greater degree of trauma
Pathophysiology
The free segment is uncoupled from the chest wall and moves passively in response to pleural pressure changes - producing paradoxical respiration:
- Inspiration: decrease in pleural pressure pulls the flail segment inward, reducing effective tidal volume
- Expiration: increase in pleural pressure pushes the segment outward
Respiratory failure is multifactorial:
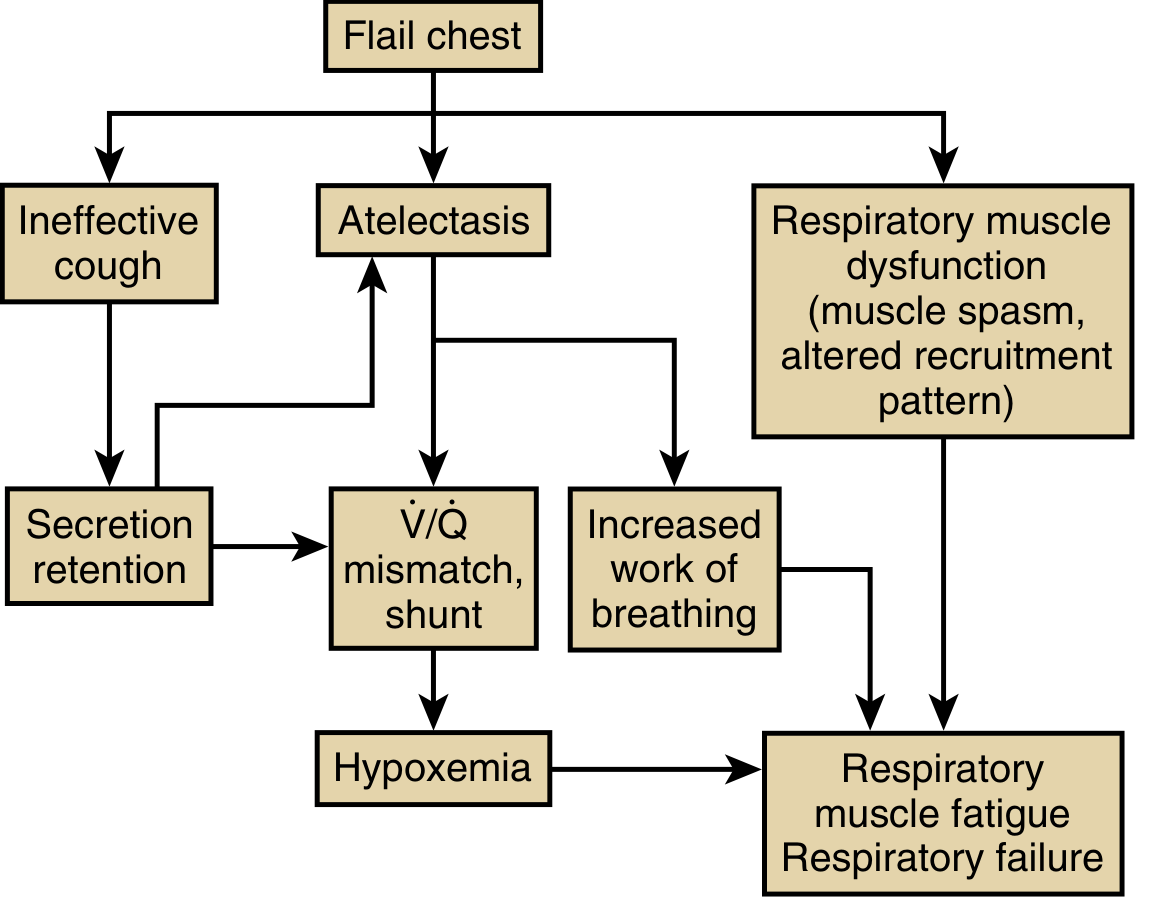
- Pain - promotes shallow breathing and suppresses cough
- Atelectasis - from splinting and secretion retention
- Respiratory muscle dysfunction - the flail segment increases the degree of muscle shortening required per breath, raising the oxygen cost of breathing
- Pulmonary contusion - almost always co-exists; reduces lung compliance and worsens V/Q mismatch and shunting
- Hypoxemia + increased work of breathing together lead to respiratory muscle fatigue and eventual failure
Note: "Pendelluft" (air shifting between injured and uninjured lung) was historically blamed but is now recognized as NOT playing a significant role.
Clinical Chest Wall Motion in Flail Chest vs Normal
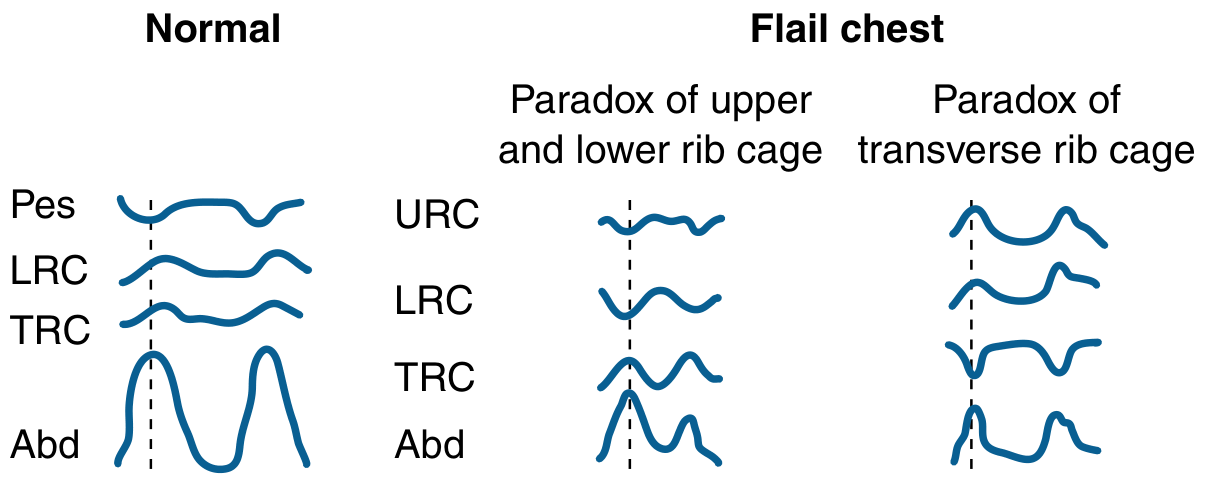
(URC = upper rib cage, LRC = lower rib cage, TRC = transverse rib cage, Abd = abdomen)
Clinical Features
- Paradoxical movement of the chest wall segment (visible or palpable)
- Pain and dyspnea
- Tachypnoea, tachycardia, hypoxia
- Crepitus over fractured ribs, may have surgical emphysema
- Associated injuries: pneumothorax, haemothorax, pulmonary contusion
Diagnosis is clinical - paradoxical wall motion on inspection/palpation. Detection may be delayed immediately post-injury due to tissue oedema or pain-induced voluntary splinting. CT chest (3D reconstruction) is the gold standard for identifying all rib fractures and associated lung injuries. The mechanically ventilated patient may not show paradoxical motion until sedation is withdrawn.
Management
Immediate / First Aid
- Immobilize the flail segment with a pressure dressing (stabilizes remaining lung ventilation)
- High-flow supplemental oxygen
Definitive Non-surgical (Mainstay)
| Component | Details |
|---|---|
| Analgesia | Multimodal: opioids, NSAIDs, intercostal nerve blocks, thoracic epidural analgesia (most effective for multiple rib fractures) |
| Oxygen | Supplemental O2 to maintain SpO2 |
| Physiotherapy | Chest physiotherapy, incentive spirometry, tracheobronchial toilet |
| Fluid management | Cautious fluid replacement (avoid over-hydration in pulmonary contusion) |
| NIV | Non-invasive positive pressure ventilation (CPAP/BiPAP) - stabilizes the flail segment pneumatically, improves gas exchange, avoids intubation complications |
Mechanical Ventilation (Invasive)
Acts as an "internal pneumatic splint" - positive pressure keeps pleural pressure positive, preventing paradoxical inward movement. Continued for 2-3 weeks until chest wall stabilizes.
Indications for early intubation and mechanical ventilation:
- Shock
- Severe head injury
- Comorbid pulmonary disease
- Fracture of 8 or more ribs
- Age > 65 years
- PaO2 < 80 mmHg despite supplemental O2
- Respiratory failure despite analgesia and O2
Early intubation reduces mortality compared with delayed intubation after onset of respiratory failure.
Surgical Fixation (Operative Rib Stabilization)
Using Judet struts, medullary wires/nails, or titanium plates. Indications:
- Inability to wean from mechanical ventilation due to chest wall instability
- Thoracotomy undertaken for concurrent injuries
- Persistent pain or progressive decline in pulmonary function
- Severe chest wall instability
Surgical fixation reduces ventilator days, ICU/hospital stay, and pneumonia rates compared to conservative management.
Complications
- Pneumonia (most common)
- Atelectasis
- ARDS (acute respiratory distress syndrome)
- Empyema
- Chest wall deformity
- Chronic pain
- Reduced lung function (fibrosis of contused area)
- Mortality: up to 33-40% (particularly when associated with pulmonary contusion; mortality as high as 56% with concurrent lung contusion)
Key Points for Exam
| Feature | Detail |
|---|---|
| Definition | ≥3 adjacent ribs, each broken in ≥2 places |
| Hallmark sign | Paradoxical respiration |
| Primary cause of hypoxia | Pulmonary contusion (not purely the mechanical flail) |
| "Pendelluft" | Historical concept, NOT relevant to pathophysiology |
| Best analgesia | Thoracic epidural |
| Internal splint method | Positive pressure ventilation |
| Gold standard imaging | CT chest (3D reconstruction) |
| Mortality | Up to 33-40% |
Sources: Bailey & Love's Short Practice of Surgery 28e; Murray & Nadel's Textbook of Respiratory Medicine; Tintinalli's Emergency Medicine; Pye's Surgical Handicraft 22e
This is a shared conversation. Sign in to Orris to start your own chat.