Explaine mi 15 commen heart disese with ecg chges and ecg imeges and their disease
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching Images
STEMI ST elevation myocardial infarction ECG
Searching Images
atrial fibrillation ECG electrocardiogram
Finding Sources
Searching Images
ventricular fibrillation ECG complete heart block third degree AV block
Searching Images
left bundle branch block right bundle branch block ECG WPW Wolff-Parkinson-White
Searching Images
hypertrophic cardiomyopathy pericarditis pulmonary embolism ECG hyperkalemia
Searching Images
ventricular tachycardia VT ECG wide complex tachycardia
Searching Images
left ventricular hypertrophy LVH ECG Sokolow voltage criteria
Searching Images
hyperkalemia peaked T waves ECG electrolyte
Searching Images
pulmonary embolism S1Q3T3 right heart strain ECG sinus tachycardia
Searching Images
long QT syndrome torsades de pointes ECG dilated cardiomyopathy
Here is a comprehensive guide to 15 Common Heart Diseases with ECG Changes and Images, drawn from Harrison's, Guyton & Hall, Tintinalli, and other authoritative sources.
15 Common Heart Diseases — ECG Changes & Images
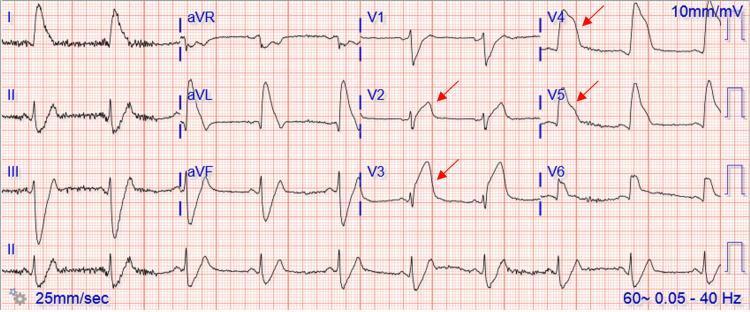
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
Disease: Acute occlusion of a coronary artery (most often LAD, RCA, or LCx) causing full-thickness myocardial infarction.
ECG Changes:
- Hyperacute T waves (earliest change — tall, broad, symmetric)
- ST-segment elevation (≥1 mm in ≥2 contiguous leads) — convex "tombstone" morphology
- Reciprocal ST depression in opposite leads
- Pathological Q waves (>40 ms wide, >25% of R wave height) — appear after hours/days, indicating necrosis
- T-wave inversion in recovery phase
- Loss of R wave progression (anterior MI)
Localization:
| Territory | Leads with ST elevation |
|---|---|
| Anterior | V1–V4 (LAD occlusion) |
| Inferior | II, III, aVF (RCA) |
| Lateral | I, aVL, V5–V6 (LCx) |
| Posterior | Tall R + ST depression V1–V2 |

2. 🫀 Non-ST Elevation MI / Unstable Angina (NSTEMI/UA)
Disease: Partial coronary occlusion or demand ischemia causing subendocardial injury without full-thickness infarction.
ECG Changes:
- ST-segment depression (≥0.5–1 mm, horizontal or downsloping) — most common
- T-wave inversion (deep, symmetric — "Wellens' pattern" in V2–V3 indicates proximal LAD disease)
- No ST elevation, no pathological Q waves
- May be normal at rest — dynamic changes during pain are diagnostic
- Transient ST elevation possible during vasospasm
Key concept: Diagnosis requires elevated troponin + symptoms; ECG alone cannot diagnose NSTEMI.
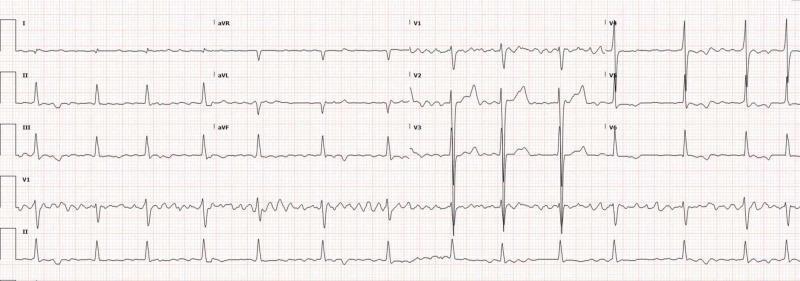
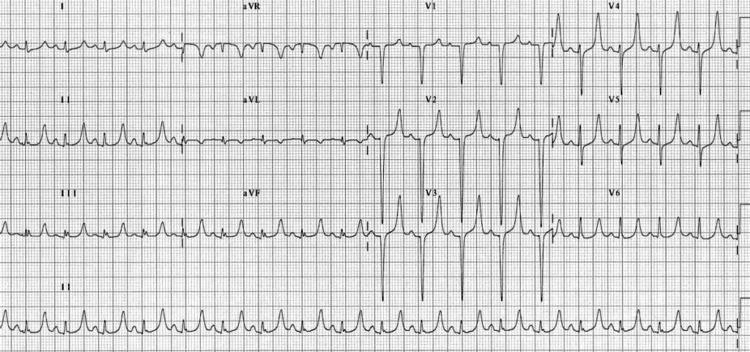
3. 🫀 Atrial Fibrillation (AF)
Disease: Chaotic, disorganized atrial electrical activity at 350–600 impulses/min, leading to irregular ventricular response. Most common sustained arrhythmia.
ECG Changes:
- Absent P waves — replaced by irregular fibrillatory (f) waves, best seen in V1 and lead II
- Irregularly irregular R-R intervals (hallmark)
- Narrow QRS (unless aberrant conduction or accessory pathway)
- Ventricular rate varies 100–180 bpm (uncontrolled) or 60–100 bpm (rate-controlled)

4. 🫀 Complete (Third-Degree) AV Heart Block
Disease: No conduction between atria and ventricles. Ventricles maintained by an escape rhythm (junctional or ventricular).
ECG Changes:
- Complete AV dissociation — P waves and QRS complexes are completely independent
- Atrial rate > ventricular rate (atria fire normally, ventricles slow)
- Escape rhythm: Narrow QRS if junctional (~40–60 bpm); wide QRS if ventricular (<40 bpm)
- Fixed, slow ventricular rate (bradycardia)
- No fixed PR relationship
5. 🫀 First & Second Degree AV Block
Disease: Delayed or intermittent AV conduction.
ECG Changes:
First-degree AV block:
- PR interval >200 ms (>5 small squares), consistent on every beat
- All P waves conduct; no dropped beats
Second-degree — Mobitz I (Wenckebach):
- Progressive PR lengthening → dropped QRS (non-conducted P wave)
- RR intervals progressively shorten before the dropped beat
- Benign; often vagal or inferior MI
Second-degree — Mobitz II:
- Constant PR interval → sudden dropped QRS (no warning)
- Often associated with LBBB/RBBB
- More serious; can progress to complete heart block
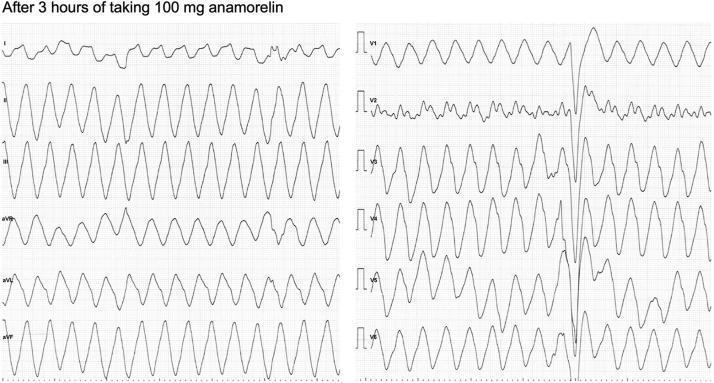
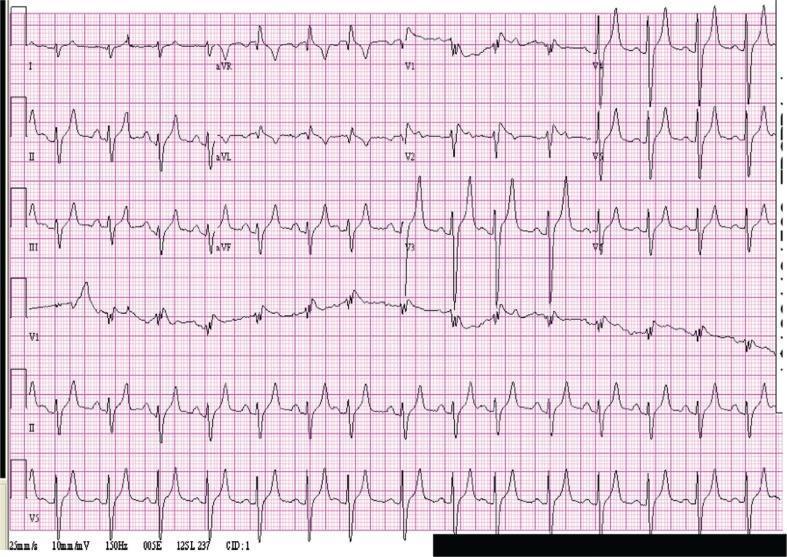
6. 🫀 Ventricular Tachycardia (VT)
Disease: Rapid, life-threatening rhythm originating in the ventricles. Rate usually 100–250 bpm. Often associated with ischemic heart disease or cardiomyopathy.
ECG Changes:
- Wide QRS (>120 ms) at rapid rate
- AV dissociation (P waves independent of QRS) — pathognomonic when visible
- Fusion beats and capture beats — confirm VT
- Concordance (all precordial leads same direction) strongly suggests VT
- Monomorphic (uniform QRS) vs. polymorphic (changing QRS — torsades de pointes)
- LBBB morphology with inferior axis = RVOT-VT
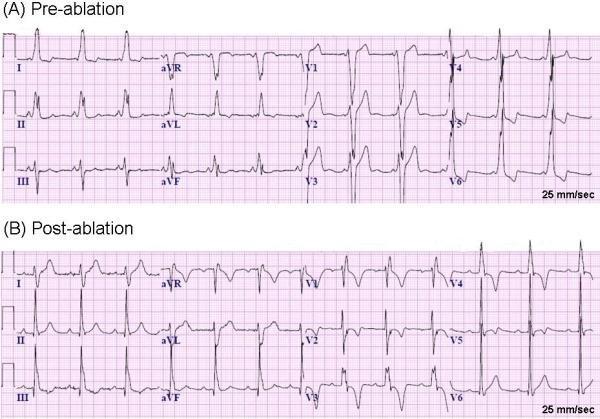
7. 🫀 Wolff-Parkinson-White (WPW) Syndrome
Disease: Accessory pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation. Risk of dangerous rapid conduction during AF.
ECG Changes (sinus rhythm):
- Short PR interval (<120 ms)
- Delta wave — slurred initial upstroke of QRS (pre-excitation)
- Wide QRS (>120 ms) due to fusion of conducted and pre-excited activation
- Pseudo-infarct patterns (mimics Q waves in inferior leads)
- During tachycardia: narrow-complex orthodromic SVT or wide-complex antidromic tachycardia
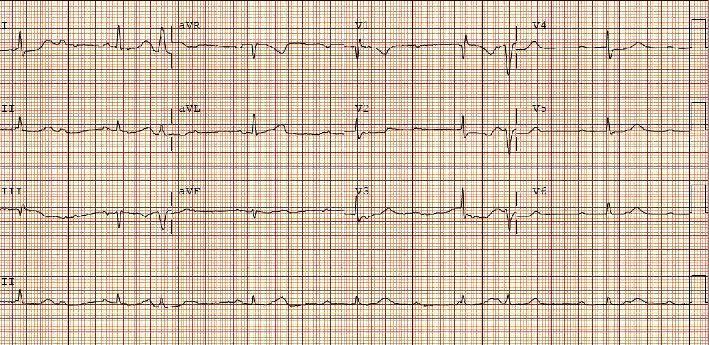
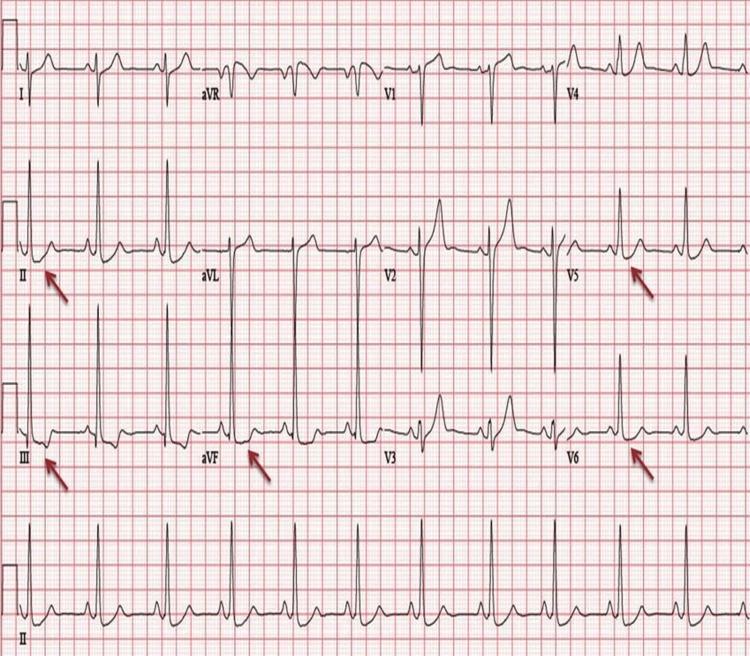
8. 🫀 Left Ventricular Hypertrophy (LVH)
Disease: Thickening of the LV wall due to chronic pressure overload (hypertension, aortic stenosis) or volume overload.
ECG Changes:
- High QRS voltage — the hallmark
- Sokolow-Lyon: S in V1 + R in V5 or V6 ≥ 35 mm
- Cornell: R in aVL + S in V3 ≥ 28 mm (men) / 20 mm (women)
- Left axis deviation
- LV strain pattern: ST depression + T-wave inversion in lateral leads (I, aVL, V5–V6)
- Prolonged QRS (partial LBBB pattern)
- Left atrial enlargement (broad, notched P wave in II; biphasic in V1)

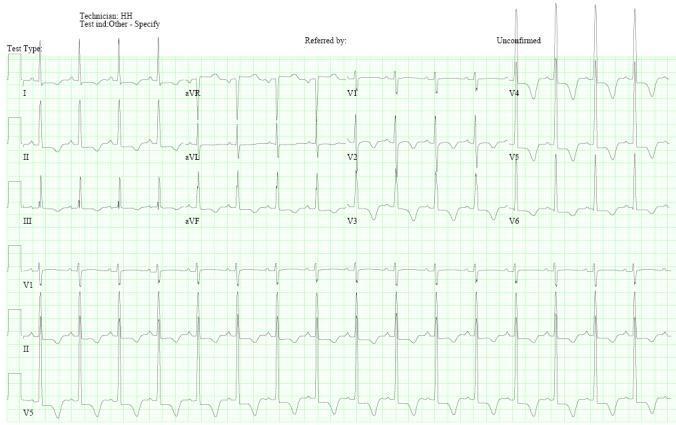
9. 🫀 Left & Right Bundle Branch Block (LBBB / RBBB)
Disease: Block in conduction through the left or right bundle branches, causing abnormal ventricular depolarization.
LBBB ECG Changes:
- Wide QRS ≥120 ms
- Broad, notched R wave in I, aVL, V5–V6 ("M-shaped")
- Deep S or QS in V1–V3
- ST and T waves opposite to QRS direction (discordant)
- Absence of normal septal Q in lateral leads
- New LBBB + chest pain = treat as STEMI equivalent (Sgarbossa criteria)
RBBB ECG Changes:
- Wide QRS ≥120 ms
- RSR' pattern in V1 ("rabbit ears")
- Broad S wave in I, aVL, V5–V6
- ST and T changes in V1–V3 (discordant)
10. 🫀 Acute Pericarditis
Disease: Inflammation of the pericardial sac; causes diffuse myocardial irritation.
ECG Changes (4 stages):
- Stage 1 (acute): Diffuse concave ("saddle-shaped") ST elevation in almost all leads (I, II, aVL, V2–V6) + PR-segment depression (most specific finding)
- Stage 2 (days): ST returns to baseline, T waves flatten
- Stage 3 (weeks): T-wave inversion
- Stage 4 (months): Normalization
Key differentiator from STEMI:
- ST elevation is diffuse (not regional)
- Concave (not convex) morphology
- PR depression present
- Reciprocal changes absent (except aVR, V1)
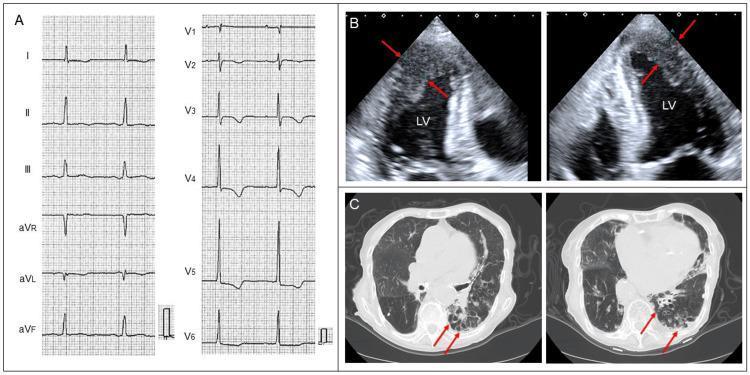
11. 🫀 Pulmonary Embolism (PE)
Disease: Occlusion of pulmonary arteries causing acute right ventricular pressure overload (acute cor pulmonale).
ECG Changes:
- Sinus tachycardia — most common (in ~40%)
- S1Q3T3 pattern (prominent S in I, Q wave in III, inverted T in III) — classic but in <20%
- Right axis deviation
- New RBBB (complete or incomplete)
- T-wave inversions in V1–V4 (right heart strain)
- P pulmonale (tall peaked P in II)
- Atrial fibrillation or flutter (less common)


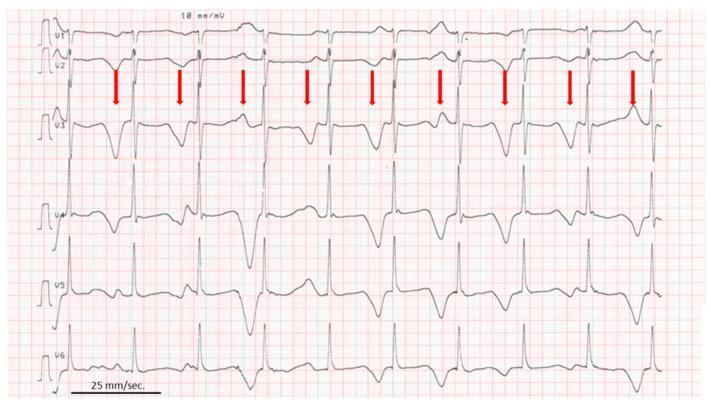
12. 🫀 Hypertrophic Cardiomyopathy (HCM)
Disease: Genetic sarcomere disorder causing asymmetric myocardial hypertrophy, especially the interventricular septum. Commonest cause of sudden death in young athletes.
ECG Changes:
- Voltage criteria for LVH (high QRS amplitude)
- Giant deep T-wave inversions in precordial leads (V3–V6) — especially in apical HCM (Maron/Yamaguchi type)
- Pathological Q waves in inferior/lateral leads (due to septal hypertrophy — mimics old MI)
- Left axis deviation
- ST depression with repolarization abnormalities
- May have WPW pattern (accessory pathway association)
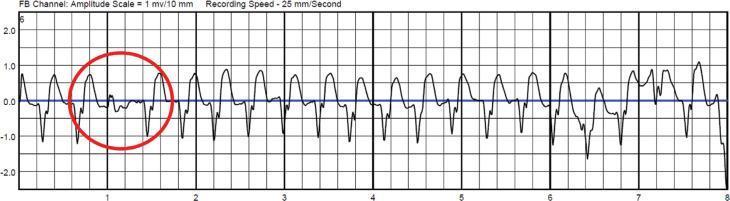
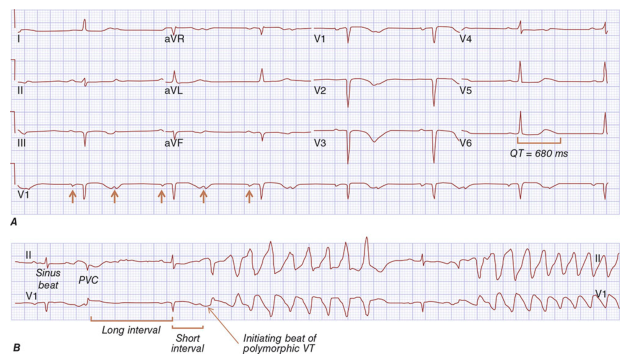
13. 🫀 Long QT Syndrome (LQTS)
Disease: Inherited or acquired (drugs, electrolytes) disorder of repolarization causing prolonged QT interval and risk of torsades de pointes → sudden death.
ECG Changes:
- Prolonged QTc (corrected for rate):
- Normal: <440 ms (men), <460 ms (women)
- Abnormal: >450 ms (men), >470 ms (women)
- Dangerous: >500 ms
- T-wave abnormalities: Broad, bifid, or biphasic T waves (LQT1–3 have distinct morphologies)
- Prominent U waves (best seen in V2–V3)
- T-wave alternans (beat-to-beat T wave variation = high risk)
- Torsades de pointes: Polymorphic VT with QRS "twisting" around baseline, initiated by short-long-short cycle
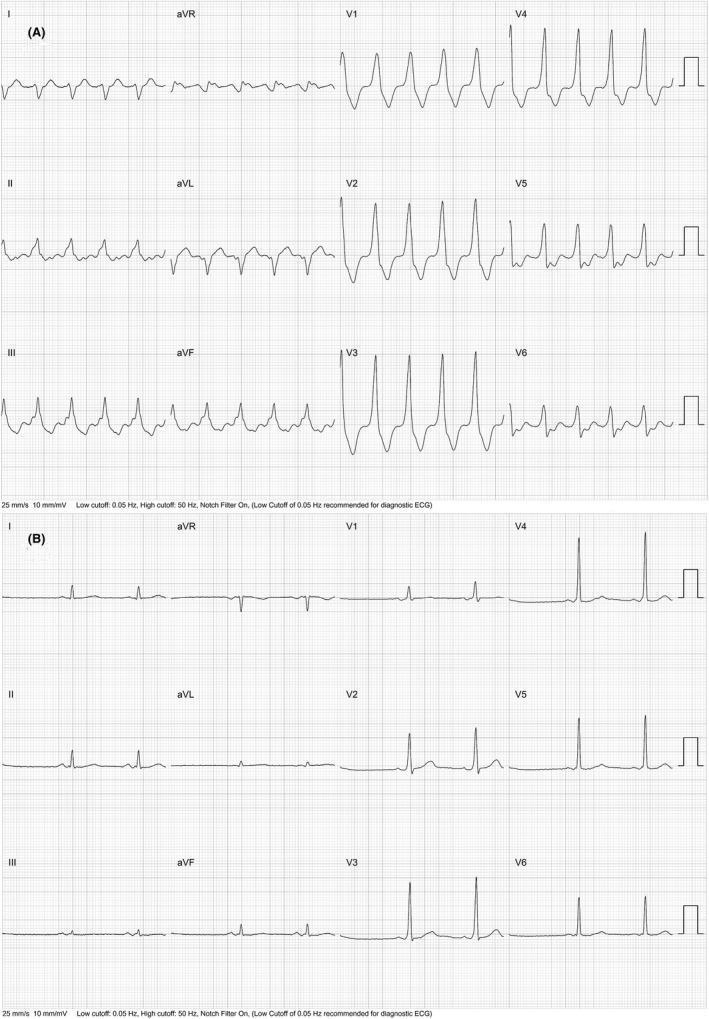
14. 🫀 Hyperkalemia
Disease: Elevated serum potassium (often renal failure, acidosis, drugs) causing progressive cardiac conduction toxicity.
ECG Changes (progressive with rising K⁺):
| K⁺ level | ECG finding |
|---|---|
| 5.5–6.5 mEq/L | Tall, peaked ("tented") T waves — narrow base, symmetric |
| 6.5–7.5 mEq/L | Flattened/absent P waves, prolonged PR interval |
| 7.0–8.0 mEq/L | Wide QRS (intraventricular conduction delay) |
| >8.0 mEq/L | Sine-wave pattern → VF → asystole |
💡 Peaked T waves + wide QRS + absent P = cardiac emergency
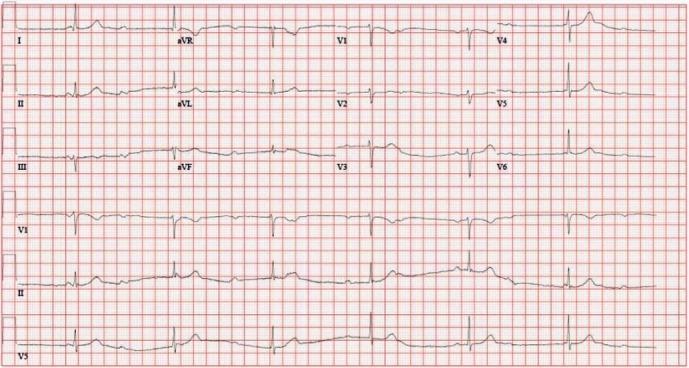
15. 🫀 Dilated Cardiomyopathy (DCM)
Disease: Enlarged, weakened ventricle with reduced ejection fraction. Causes include ischemia, viral myocarditis, alcohol, idiopathic.
ECG Changes:
- Left bundle branch block (LBBB) — very common (~25%)
- Low voltage (QRS <5 mm in limb leads; <10 mm in precordial leads)
- Sinus tachycardia (compensatory)
- Atrial fibrillation (due to atrial dilation)
- Pathological Q waves (mimicking old MI — "ischemic pattern")
- Non-specific ST-T wave changes throughout
- Left axis deviation
- First-degree AV block (PR prolongation)
- Ventricular ectopy / NSVT (risk of sudden death)
Quick Reference Summary Table
| # | Disease | Key ECG Finding |
|---|---|---|
| 1 | STEMI | ST elevation + Q waves, reciprocal depression |
| 2 | NSTEMI/UA | ST depression, T inversion, no Q waves |
| 3 | Atrial Fibrillation | Absent P waves, irregularly irregular |
| 4 | Complete Heart Block | AV dissociation, slow escape rhythm |
| 5 | 1st/2nd Degree AV Block | PR prolongation / dropped beats |
| 6 | Ventricular Tachycardia | Wide QRS tachycardia, AV dissociation |
| 7 | WPW Syndrome | Short PR, delta wave, wide QRS |
| 8 | LVH | High voltage QRS, strain pattern |
| 9 | BBB | Wide QRS, RSR' (RBBB) or notched R (LBBB) |
| 10 | Acute Pericarditis | Diffuse saddle ST elevation, PR depression |
| 11 | Pulmonary Embolism | S1Q3T3, sinus tachycardia, RBBB |
| 12 | Hypertrophic CM | Giant T inversions, LVH, septal Q waves |
| 13 | Long QT Syndrome | Prolonged QTc, torsades de pointes |
| 14 | Hyperkalemia | Peaked T waves → widened QRS → sine wave |
| 15 | Dilated CM | LBBB, low voltage, AF, non-specific ST changes |
Sources: Guyton & Hall Textbook of Medical Physiology; Harrison's Principles of Internal Medicine 22e; Tintinalli's Emergency Medicine; Goldman-Cecil Medicine — ECG section.
This is a shared conversation. Sign in to Orris to start your own chat.