Mechanism od action of dopamine in various cns disease and in grneral
Reading File
Finding Sources
Finding Sources
Searching PubMed
dopamine receptor CNS mechanism disease
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full response:
Dopamine: Mechanism of Action in the CNS and CNS Diseases
1. Dopamine Basics - Synthesis, Storage, Release
Dopamine (DA) is a catecholamine neurotransmitter synthesized from the amino acid L-tyrosine:
L-Tyrosine → L-DOPA (via tyrosine hydroxylase, the rate-limiting step) → Dopamine (via DOPA decarboxylase/aromatic amino acid decarboxylase)
Dopamine is then packaged into vesicles by VMAT2, released into the synapse on nerve impulse, and cleared primarily by:
- DAT (dopamine transporter) - reuptake back into the presynaptic terminal
- MAO-A/B (monoamine oxidase) - enzymatic degradation to HVA (homovanillic acid)
- COMT (catechol-O-methyltransferase) - methylation degradation
2. Dopamine Receptors - Subtypes and Signaling
All dopamine receptors are G-protein coupled receptors (GPCRs). They fall into two families:
| Family | Subtypes | G-protein | Effect on cAMP | Location |
|---|---|---|---|---|
| D1-like | D1, D5 | Gs | Increases cAMP (via adenylate cyclase activation) | Striatum, PFC, limbic |
| D2-like | D2, D3, D4 | Gi/Go | Decreases cAMP (adenylate cyclase inhibition) | Striatum, mesolimbic, pituitary |
Intracellular cascade:
- D1-like activation → Gs → ↑adenylate cyclase → ↑cAMP → activates PKA → phosphorylates CREB (transcription factor) → gene expression changes (including BDNF, dynorphin, enkephalin, tyrosine hydroxylase)
- D2-like activation → Gi → ↓cAMP → inhibition of PKA cascade; also opens K+ channels and closes Ca²+ channels → reduced neuronal excitability
Autoreceptors (D2 and D3 on presynaptic terminals and somatodendritic areas) provide negative feedback - when dopamine binds, they shut off further dopamine synthesis and release.
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, Gene Expression section
3. The Five Classic Dopamine Pathways
(a) Nigrostriatal Pathway
- Origin: Substantia nigra pars compacta (SNpc) → Striatum (caudate-putamen)
- Function: Motor control, movement initiation
- DA receptors: D1 (on direct/"GO" pathway GABAergic neurons) and D2 (on indirect/"STOP" pathway neurons)
- D1 stimulation activates the direct pathway → facilitates movement ("GO more")
- D2 stimulation inhibits the indirect pathway → also facilitates movement ("STOP less")
- Disease relevance: Parkinson's disease
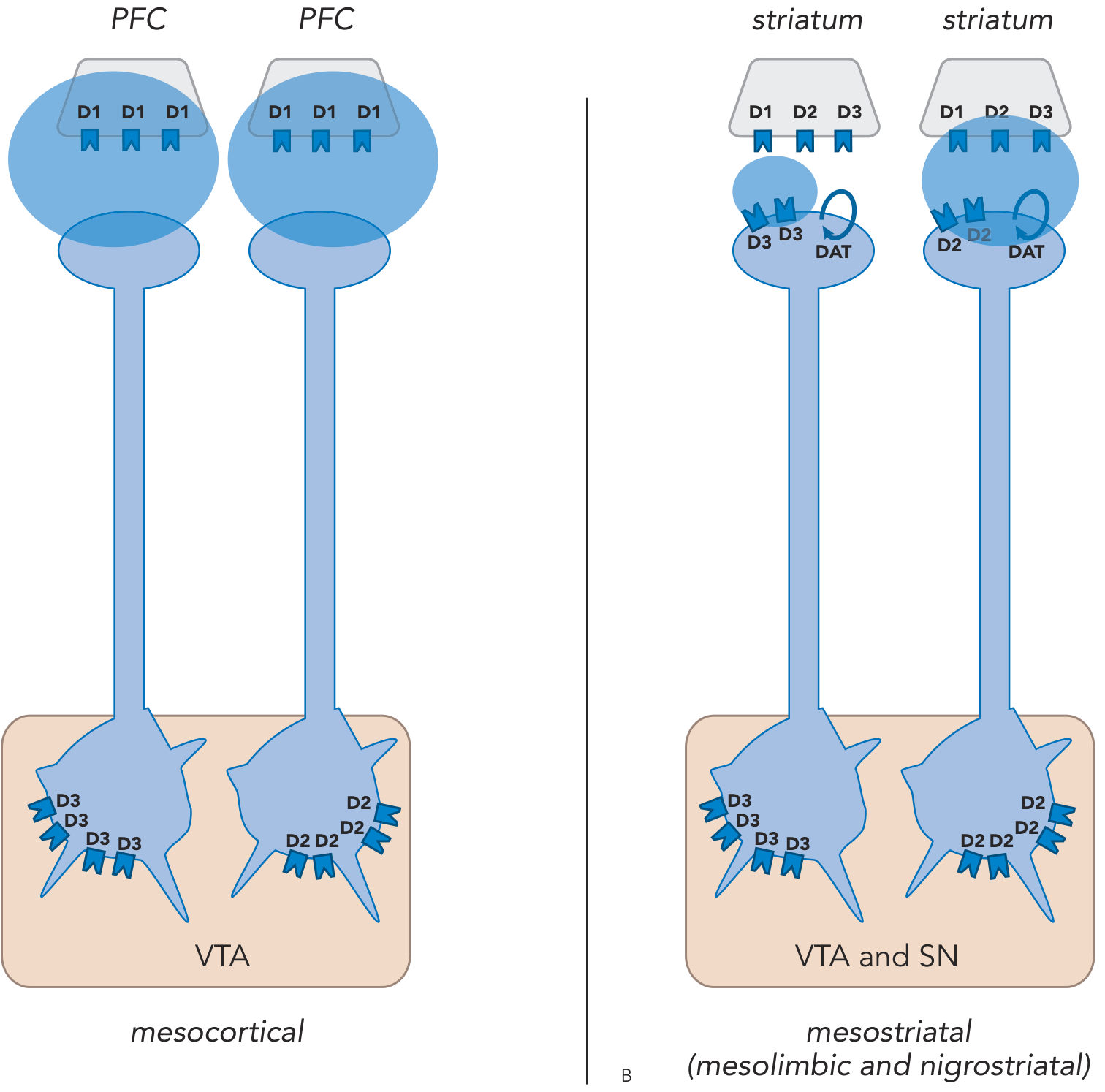
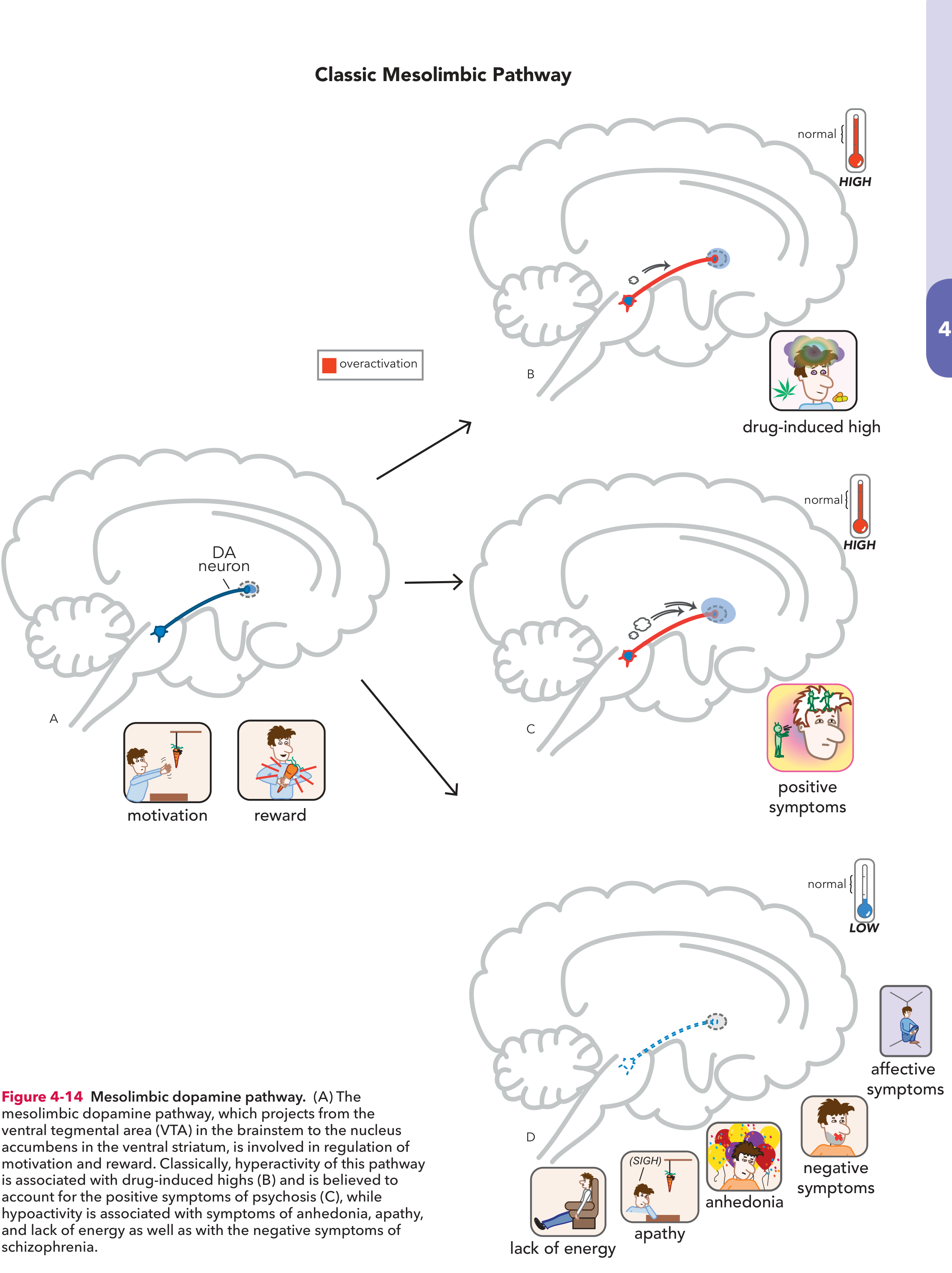
(b) Mesolimbic Pathway
- Origin: Ventral tegmental area (VTA) → Nucleus accumbens (ventral striatum) and other limbic structures
- Function: Reward, motivation, pleasure, reinforcement learning
- Regulated by: D3 autoreceptors at both VTA somatodendritic region and striatal terminals; few DATs = wider dopamine diffusion
- Disease relevance: Schizophrenia (positive symptoms), addiction, depression (anhedonia)
(c) Mesocortical Pathway
- Origin: VTA → Prefrontal cortex (PFC)
- Dorsolateral PFC (DLPFC) - cognition and executive function
- Ventromedial PFC (VMPFC) - emotions and affect
- Key feature: Very few presynaptic D2/D3 autoreceptors and few DATs in the PFC, so dopamine diffuses widely and is not tightly regulated
- Predominant postsynaptic receptor: D1 (excitatory)
- Disease relevance: Schizophrenia (negative and cognitive symptoms), ADHD, depression
(d) Tuberoinfundibular Pathway
- Origin: Hypothalamus → Anterior pituitary
- Function: Tonically inhibits prolactin release via D2 receptors
- Disease relevance: Blockade by antipsychotics → hyperprolactinemia (galactorrhea, amenorrhea, sexual dysfunction)
(e) Thalamic Pathway
- Less well-characterized; projects from multiple dopamine cell groups to thalamic nuclei; role in sensory gating and arousal
- Stahl's Essential Psychopharmacology, Classic Dopamine Pathways, p. 100-107
4. Dopamine in CNS Diseases
A. Parkinson's Disease
The core mechanism is degeneration of dopaminergic neurons in the SNpc, with >80% neuronal loss before symptoms appear. Lewy bodies (alpha-synuclein aggregates) are the pathological hallmark.
Consequence of dopamine depletion in the nigrostriatal pathway:
- The striatum loses dopamine input
- Without D1 activation on the direct pathway, the "GO" signal is lost (akinesia, bradykinesia)
- Without D2 inhibition of the indirect pathway, the "STOP" signal is overactive - excessive subthalamic nucleus (STN) output inhibits the thalamus → hypokinesia, rigidity, resting tremor
- The "funnel" of activity feeding the supplementary motor area (SMA) via the basal ganglia-thalamic circuit is effectively closed
Treatment logic: Levodopa (L-DOPA) + carbidopa restores dopamine; dopamine agonists (pramipexole, ropinirole) act at D2/D3 receptors; MAO-B inhibitors (selegiline, rasagiline) reduce degradation
- Neuroscience: Exploring the Brain, 5th Ed., Basal Ganglia Disorders, p. 1357
B. Schizophrenia
The dopamine hypothesis has two complementary components:
1. Mesolimbic HYPERdopaminergia → Positive symptoms
Excess dopamine in the mesolimbic pathway causes delusions, hallucinations, disorganization, agitation. Psychostimulants (cocaine, amphetamine) that flood this pathway can replicate positive psychosis in healthy individuals, and worsen schizophrenia. All effective antipsychotics block D2 receptors in this pathway.
2. Mesocortical HYPOdopaminergia → Negative and cognitive symptoms
Deficient DA activity in projections to the DLPFC causes cognitive symptoms (impaired working memory, executive dysfunction) and negative symptoms (blunted affect, avolition). Deficient DA in the VMPFC causes affective/emotional flattening.
The clinical dilemma: Blocking D2 in the mesolimbic pathway treats positive symptoms, but simultaneously blocking D2 in the mesocortical pathway worsens negative/cognitive symptoms. Atypical antipsychotics (clozapine, quetiapine) have lower D2 occupancy and add serotonin (5-HT2A) blockade to partially address this.
D2 receptor occupancy thresholds:
- Therapeutic antipsychotic effect: ~65-75% D2 occupancy
- EPS (extrapyramidal side effects): >80% D2 occupancy
- Hyperprolactinemia: even modest D2 blockade in tuberoinfundibular pathway
- Stahl's Essential Psychopharmacology, Ch. 4; Kaplan & Sadock's Comprehensive Textbook, p. 9211
C. ADHD
ADHD is hypothesized as inefficient "tuning" of prefrontal cortical circuits by DA and norepinephrine (NE).
- ADHD patients have insufficient tonic DA (and NE) firing in the PFC
- Low DA → inadequate D1 and D3 stimulation in the DLPFC → poor working memory, sustained attention, and executive function
- Low DA in the anterior cingulate cortex → poor selective attention
- Phasic DA bursts in the nucleus accumbens, when dysregulated, reinforce impulsive behaviors
The "inverted U" principle: DA has an optimal working range. Too little DA = poor PFC function; too much DA = also poor PFC function (recruits less-sensitive receptors, impairs signal-to-noise). Stimulants (methylphenidate, amphetamine) restore DA (and NE) to the "sweet spot" by blocking DAT/releasing catecholamines.
- Stahl's Essential Psychopharmacology, Ch. 11 (ADHD), p. 465-470
D. Depression
- Mesolimbic hypodopaminergia contributes to anhedonia (the inability to feel pleasure) and psychomotor slowing - cardinal features of depression
- Inflammation (proinflammatory cytokines) reduces dopamine synthesis, impairs dopamine release, and downregulates dopamine receptors
- Low dopamine in the nucleus accumbens = reduced motivation, loss of reward, apathy and lack of energy
- Antidepressants with dopaminergic action (bupropion - DAT/NET blocker; aripiprazole - partial D2 agonist) target this pathway
- Kaplan & Sadock's Comprehensive Textbook, Mechanisms by which Inflammation Promotes Depressive Symptoms
E. Addiction / Substance Use Disorders
All drugs of abuse share a common final mechanism: flood the mesolimbic pathway with dopamine at the nucleus accumbens.
Acute effect: Drug-induced DA surge → massive D1 receptor activation → cAMP/PKA → CREB phosphorylation → transcription factor activation → "high" (artificial reward signal)
Chronic/molecular adaptations:
- Repeated cocaine/amphetamine → compensatory ↑ CREB in nucleus accumbens → upregulates dynorphin (an endogenous kappa-opioid) → activates KOR on VTA DA neurons → reduces baseline dopamine tone (hypodopaminergic state)
- Reduced basal DA = anhedonia, craving, withdrawal dysphoria - drives compulsive drug-seeking
- ΔFosB accumulates (longer-lasting than CREB changes) → sustained gene expression changes underlying long-term addiction vulnerability
- Kaplan & Sadock's Comprehensive Textbook, Gene Expression/SUD section
F. Huntington's Disease
The reverse of Parkinson's: striatal dopamine D2-receptor-bearing neurons degenerate (GABA/enkephalin neurons of the indirect pathway die first).
- Loss of indirect "STOP" pathway → decreased basal ganglia inhibitory output → thalamus becomes disinhibited → excess thalamocortical drive → hyperkinesia, choreiform movements
- Over time, direct pathway neurons also die → late-stage rigidity and hypokinesia
G. Restless Legs Syndrome (RLS) and Periodic Limb Movement Disorder
Iron-dependent dopaminergic pathways in the spinal cord/A11 region are dysfunctional. Dopamine agonists (pramipexole, ropinirole) are first-line treatment.
H. Tourette Syndrome / Tics
Hyperactivity of dopaminergic circuits in the striatum underlies motor and vocal tics. Treatment includes D2 blockers (haloperidol, fluphenazine) or partial D2 agonists.
5. Summary Table
| Pathway | Normal Function | Disease (Too Little DA) | Disease (Too Much DA) |
|---|---|---|---|
| Nigrostriatal | Motor control | Parkinson's (rigidity, bradykinesia) | Tardive dyskinesia, Huntington-like (indirect) |
| Mesolimbic | Reward, motivation | Depression (anhedonia), negative symptoms of schizophrenia | Positive psychosis (schizophrenia), drug addiction |
| Mesocortical | Cognition, executive function, affect | ADHD, negative/cognitive symptoms of schizophrenia, depression | (Less common clinically) |
| Tuberoinfundibular | Inhibit prolactin | Hyperprolactinemia (D2 blockade side effect) | - |
Recent evidence note (PubMed 2025): A new review (PMID 40543805) highlights that dopamine signaling extends beyond neurons - astrocytes actively participate in dopamine signaling through D1/D2 receptors and dopamine reuptake, contributing to pathophysiology in conditions like Parkinson's disease and schizophrenia. This is an emerging refinement of the classical neuron-centric model.
Primary sources: Stahl's Essential Psychopharmacology (Neuroscientific Basis); Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Neuroscience: Exploring the Brain, 5th Ed.; Katzung's Basic and Clinical Pharmacology, 16th Ed.
Generate a comparison table of antipsychotics by D2 occupancy profiles
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have all the data needed for a thorough, textbook-grounded comparison table. Here it is:
Antipsychotics: D2 Receptor Occupancy Comparison
The Therapeutic Window - the Key Framework
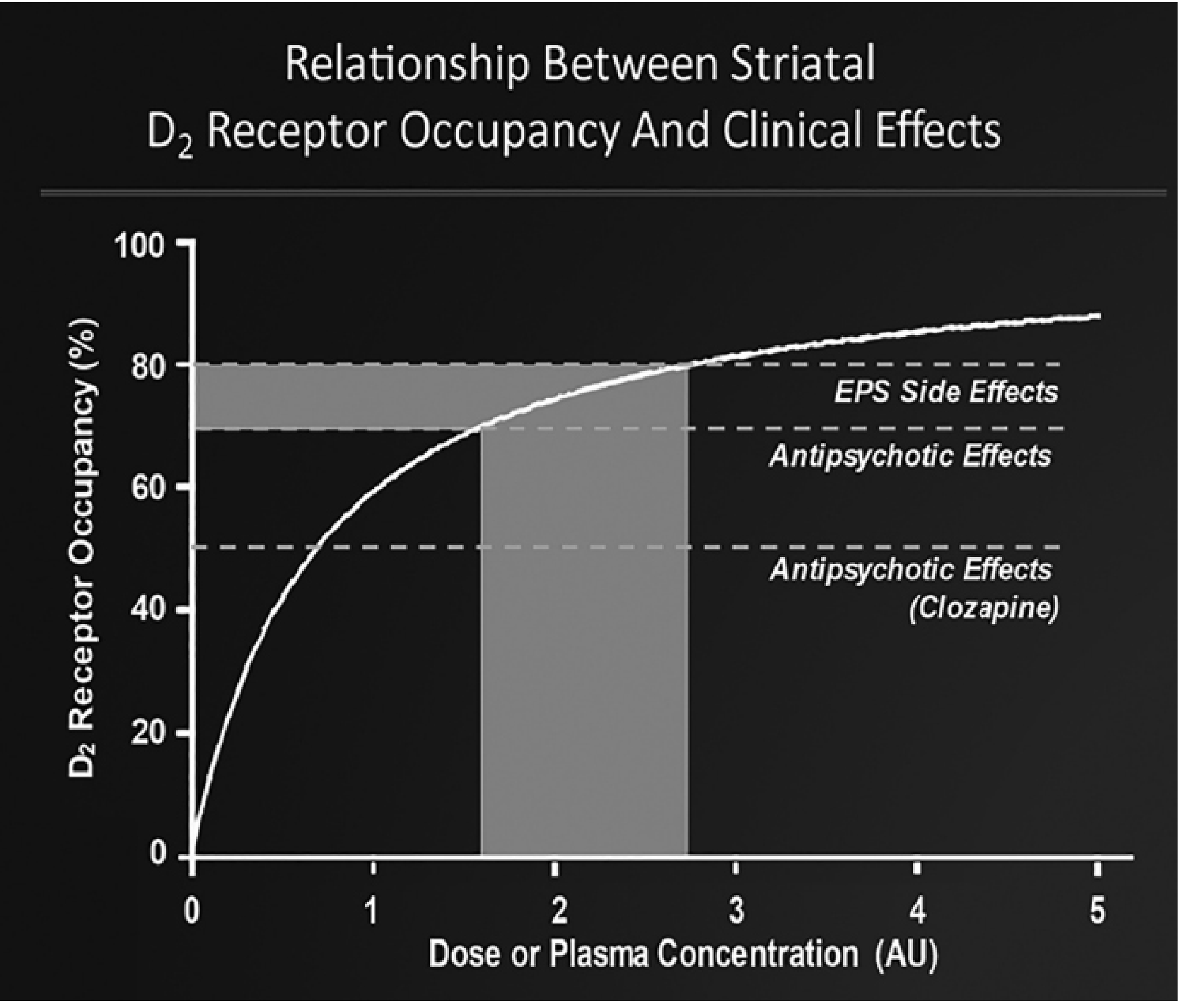
The PET-based framework established by Lars Farde and collaborators defines three critical thresholds:
- <60% D2 occupancy - sub-therapeutic (insufficient antipsychotic effect)
- 60-80% - therapeutic window (antipsychotic effect, minimal EPS)
- >80% - EPS threshold (parkinsonism, akathisia, dystonia, tardive dyskinesia risk)
- Clozapine exception: effective at only 40-50% due to preferential extrastriatal (temporal-limbic) binding and broad multi-receptor activity
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, D2 Receptor Occupancy section, p. 4645-4650
Comparison Table: Antipsychotics by D2 Occupancy Profile
| Drug | Generation | D2 Mechanism | Typical Striatal D2 Occupancy (therapeutic doses) | D2 Ceiling | 5-HT2A Occupancy | EPS Risk | Prolactin Effect | Key Notes |
|---|---|---|---|---|---|---|---|---|
| Haloperidol | FGA | Full antagonist | 75-90% | ~90% | Low | High | High ↑↑↑ | Gold standard comparator; narrow therapeutic window; >80% at doses >6 mg |
| Chlorpromazine | FGA | Full antagonist | 75-85% | ~85% | Moderate | High | High ↑↑↑ | Also strong alpha-1, H1, M1 blockade |
| Fluphenazine | FGA | Full antagonist | 75-90% | ~90% | Low | High | High ↑↑↑ | Available as decanoate LAI; long t½ |
| Perphenazine | FGA | Full antagonist | 75-85% | ~85% | Low-moderate | High | High ↑↑↑ | Mid-potency FGA |
| Pimozide | FGA | Full antagonist | 75-85% | ~85% | Low | High | High ↑↑↑ | Also D4, calcium channel block; QTc risk |
| Risperidone | SGA | Full antagonist | 70-80% | ~80% (EPS appears at >6 mg) | Very high (>80%) | Moderate (dose-dependent; "atypicality" lost >80%) | High ↑↑↑ | Most prolactin-raising SGA; plasma level 40 ng/mL ≈ EPS threshold |
| Paliperidone | SGA | Full antagonist | 70-80% | ~80% | Very high | Moderate-high | High ↑↑↑ | Active metabolite of risperidone; similar profile |
| Olanzapine | SGA | Full antagonist | 70-80% | ~80% (EPS appears >30 mg) | Very high | Low-moderate | Moderate ↑↑ | 5-HT2A/D2 ratio protects from EPS at low-moderate doses; metabolic side effects |
| Quetiapine | SGA | Full antagonist (fast dissociation) | 30-60% (striatal) | ~60-70% max even at high doses | High | Very low | None/minimal | "Hit-and-run" kinetics - very fast koff; occupancy undetectable 24h after dose; sedation from H1/alpha-1; preferential extrastriatal binding |
| Ziprasidone | SGA | Full antagonist | 45-75% | ~80% | Very high (5-HT2A:D2 ratio = 11) | Low | Minimal ↑ | Also 5-HT1A agonist, NE/5-HT reuptake inhibition; QTc prolongation risk |
| Clozapine | SGA | Full antagonist (fast dissociation + low affinity) | 40-50% (striatal) | ~60-70% even at very high doses | Very high | Virtually zero EPS | None/↓ (may lower prolactin) | Paradigm exception: efficacy from extrastriatal/temporal-limbic binding + M1, 5-HT2A, D4, alpha activity; agranulocytosis risk |
| Amisulpride | SGA | Full antagonist (selective D2/D3) | 70-80% | ~80% | Minimal (no 5-HT2A activity) | Moderate | Very high ↑↑↑ | Unique: no 5-HT2A block yet still "atypical" at low doses (presynaptic D2/D3 blockade → increased DA); highest prolactin elevation |
| Aripiprazole | SGA (3rd gen) | D2 partial agonist (18-25% intrinsic activity) | 80-95% (near-complete saturation) | Saturates at clinical doses | High 5-HT2A, but lower than antagonists | Very low despite high occupancy | None/↓ (may lower prolactin) | Partial agonism maintains residual D2 signal → prevents EPS; ceiling effect from agonist component |
| Brexpiprazole | SGA (3rd gen) | D2 partial agonist (lower intrinsic activity than aripiprazole) | 80-95% | Saturates at clinical doses | Very high | Very low | None/minimal | Slightly less activating than aripiprazole; also strong 5-HT1A partial agonist |
| Cariprazine | SGA (3rd gen) | D2/D3 partial agonist (preferential D3) | 80-95% | Saturates at clinical doses | High | Very low | None/minimal | Highest D3 affinity of approved antipsychotics; potential benefit in negative symptoms and depression |
| Lurasidone | SGA | Full antagonist | 65-80% | ~80% | Very high (5-HT2A) | Low-moderate | Moderate ↑ | Also 5-HT7 antagonist (may benefit cognition/depression); no QTc, metabolically neutral |
| Pimavanserin | Novel | No D2 activity | ~0% D2 | None | Very high 5-HT2A inverse agonist | None | None | Antipsychotic via pure 5-HT2A/2C mechanism; approved for Parkinson's psychosis only |
| Lumateperone | Novel | D2 partial agonist + 5-HT2A | Low-moderate D2 | Low | Very high | Very low | Minimal | Unique presynaptic D2 agonist/postsynaptic antagonist profile |
Key Principles Illustrated by the Table
1. The "Atypicality" Rule
5-HT2A blockade "buffers" D2 antagonism in the striatum by counteracting dopamine depletion effects. But this protection fails above ~80% D2 occupancy regardless of 5-HT2A binding. Olanzapine and risperidone become "typical" at high doses.
2. Fast Dissociation ("Hit-and-Run") Kinetics
Clozapine and quetiapine have rapid koff (fast off-rate) from D2 receptors. Endogenous dopamine can compete effectively and reclaim the receptor, which explains:
- Low EPS despite significant clinical efficacy
- Undetectable striatal D2 occupancy 24h post-quetiapine
- Clozapine's antipsychotic effect correlating more with extrastriatal (temporal-limbic cortex) than striatal D2 binding
3. Partial Agonists - Why High Occupancy Does Not Mean High EPS
Aripiprazole, brexpiprazole, and cariprazine achieve 80-95% D2 occupancy yet rarely cause EPS. The reason: their intrinsic activity (18-25% of dopamine's maximal effect) provides just enough postsynaptic D2 signal in the striatum to prevent EPS, while the near-complete occupancy blocks excess dopamine in the mesolimbic pathway. They can be thought of as "functional partial blockers" rather than complete silencers of the D2 receptor.
4. Prolactin - the Tuberoinfundibular Pathway Proxy
Prolactin elevation tracks D2 occupancy in the tuberoinfundibular pathway. Drugs with minimal prolactin elevation either:
- Have very fast dissociation (clozapine, quetiapine)
- Are partial agonists with residual D2 activity (aripiprazole → actually decreases prolactin in some patients)
- Have low affinity for pituitary D2 receptors
Amisulpride causes the highest prolactin elevation of all antipsychotics despite being "atypical," because it has no 5-HT2A activity to offset D2 blockade in the pituitary.
D2 Occupancy at a Glance (Visual Summary)
D2 Occupancy %:
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
|-----|-----|-----|-----|-----|-----|-----|-----|-----|-----|
[CLOZAPINE max striatal ~50%]
[QUETIAPINE max striatal ~60-70%]
[ZIPRASIDONE ~45-75%]
[OLANZAPINE 70-80%]
[RISPERIDONE 70-80%]
[LURASIDONE 65-80%]
[HALOPERIDOL 75-90%]
| |
Efficacy↑ EPS threshold
(>60%) (~80%)
[ARIPIPRAZOLE ~85-95%*]
[BREXPIPRAZOLE ~85-95%*]
[CARIPRAZINE ~85-95%*]
* partial agonists - high occupancy without EPS
Sources: Kaplan & Sadock's Comprehensive Textbook of Psychiatry (D2 Receptor Occupancy and Beneficial and Adverse Effects of Antipsychotics); Goodman & Gilman's The Pharmacological Basis of Therapeutics, Ch. 19; Stahl's Essential Psychopharmacology (Neuroscientific Basis), Ch. 5; Kaplan and Sadock's Synopsis of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.