coagulation pathway
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Coagulation Pathway
The coagulation pathway is a series of amplifying enzymatic reactions that deposit an insoluble fibrin clot at sites of vascular injury. The cascade is organized around three phases: initiation (extrinsic pathway), amplification (intrinsic pathway), and a common pathway that generates thrombin and fibrin.
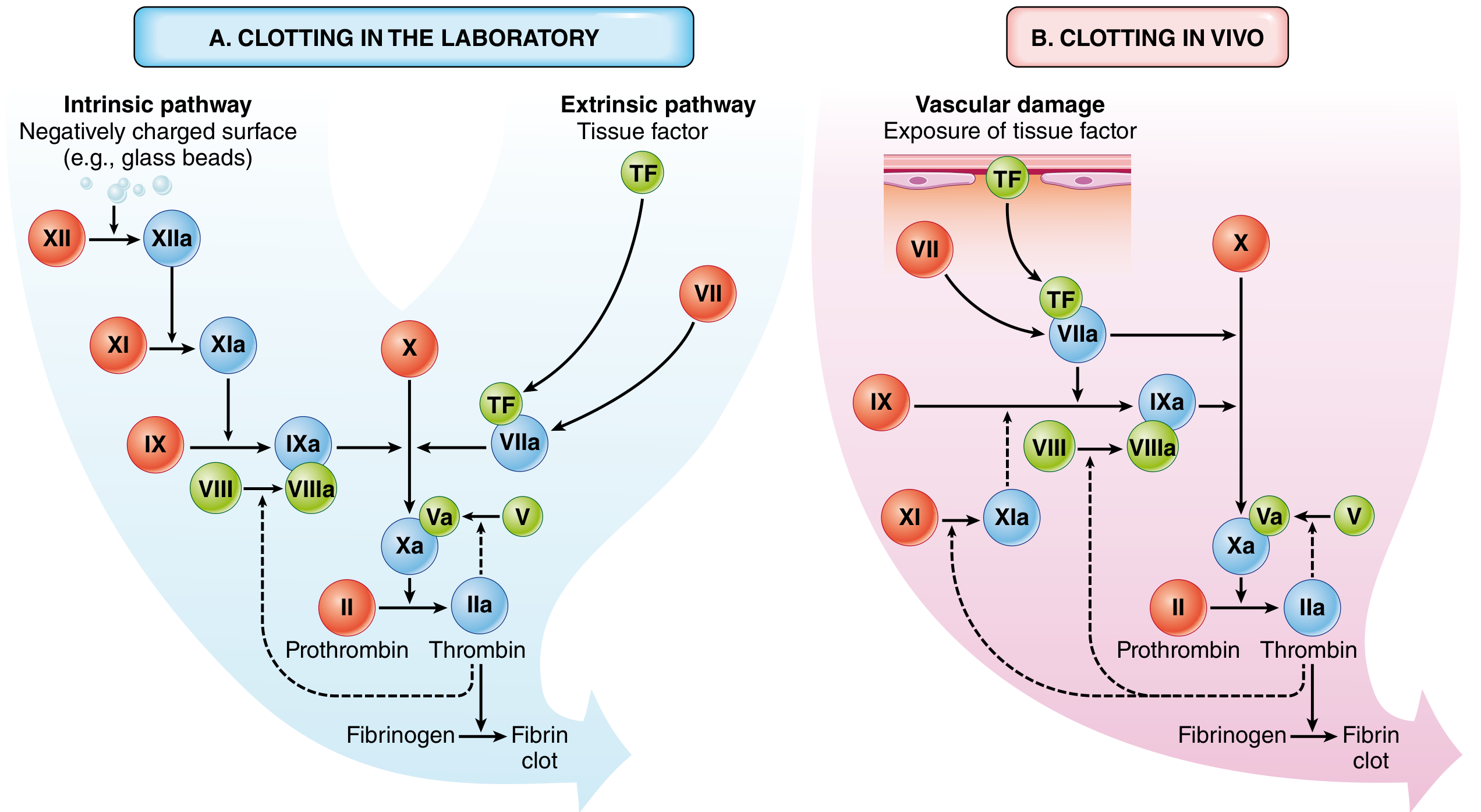
A: Laboratory model showing intrinsic and extrinsic arms. B: In vivo model where tissue factor is the dominant initiator and thrombin feedback loops (dashed lines) amplify the response. Red = inactive factors; Blue = active factors; Green = cofactors.
Core Principles
Every step of the cascade involves four components assembled on a phospholipid membrane surface (provided by activated platelets):
- An enzyme (activated coagulation factor - serine protease)
- A substrate (inactive zymogen)
- A cofactor (reaction accelerator)
- Calcium ions (bind to γ-carboxylated glutamic acid residues on factors II, VII, IX, X)
The γ-carboxylation of these Gla residues is vitamin K-dependent. Warfarin (coumadin) blocks this step, inhibiting factors II, VII, IX, and X. - Robbins & Cotran Pathologic Basis of Disease, p. 122
1. Extrinsic Pathway (Initiation)
Trigger: Vascular injury exposes subendothelial tissue factor (TF / Factor III)
Steps:
- TF is exposed on subendothelial cells and activated monocytes after injury
- Small amounts of circulating Factor VIIa bind to TF to form the extrinsic tenase complex (TF-VIIa-Ca²⁺) on phospholipid membranes
- This complex activates Factor X → Xa (directly)
- The same TF-VIIa complex also activates Factor IX → IXa (crossover activation - key bridge to the intrinsic pathway)
Lab test: Prothrombin Time (PT) - assesses factors VII, X, V, II, and fibrinogen
- Miller's Anesthesia 10e, p. 6715
2. Intrinsic Pathway (Amplification/Contact Activation)
Trigger (in vitro): Negatively charged surfaces (glass, kaolin) activate Factor XII (Hageman factor)
Trigger (in vivo): Thrombin generated by the extrinsic pathway feedback-activates Factor XI; the TF-VIIa complex also directly activates Factor IX
Trigger (in vivo): Thrombin generated by the extrinsic pathway feedback-activates Factor XI; the TF-VIIa complex also directly activates Factor IX
Steps:
- XII → XIIa (contact activation, aided by high-molecular-weight kininogen [HK] and prekallikrein [PK])
- XIIa → XI → XIa
- XIa → IX → IXa
- IXa + VIIIa (cofactor) + Ca²⁺ + phospholipid = Intrinsic tenase complex
- Intrinsic tenase: Factor X → Xa
Note: Factor XII deficiency does NOT cause clinical bleeding, confirming that the intrinsic pathway is primarily an amplification system in vivo, not the main initiator. Factor XI deficiency causes only mild bleeding. - Miller's Anesthesia 10e, p. 6716
Lab test: aPTT (Partial Thromboplastin Time) - assesses factors XII, XI, IX, VIII, X, V, II, and fibrinogen
3. Common Pathway
Both pathways converge on Factor Xa.
Prothrombinase complex:
- Factor Xa + Factor Va (cofactor) + Ca²⁺ + phospholipid membrane
- Converts prothrombin (Factor II) → Thrombin (Factor IIa) - the "surge" in thrombin generation
Thrombin actions (the master regulator):
| Action | Mechanism |
|---|---|
| Fibrin clot formation | Cleaves fibrinopeptides A and B from fibrinogen → fibrin monomers → fibrin polymer |
| Clot stabilization | Activates Factor XIII → XIIIa (transglutaminase) → covalently cross-links fibrin strands → insoluble clot |
| Amplification feedback | Activates Factors V, VIII, XI → amplifies its own production |
| Platelet activation | Activates PAR-1 receptors on platelets → potent platelet aggregation |
| Pro-inflammatory | PAR activation on endothelium/immune cells → angiogenesis, tissue repair |
- Robbins & Cotran, p. 123; Miller's Anesthesia 10e, p. 6717
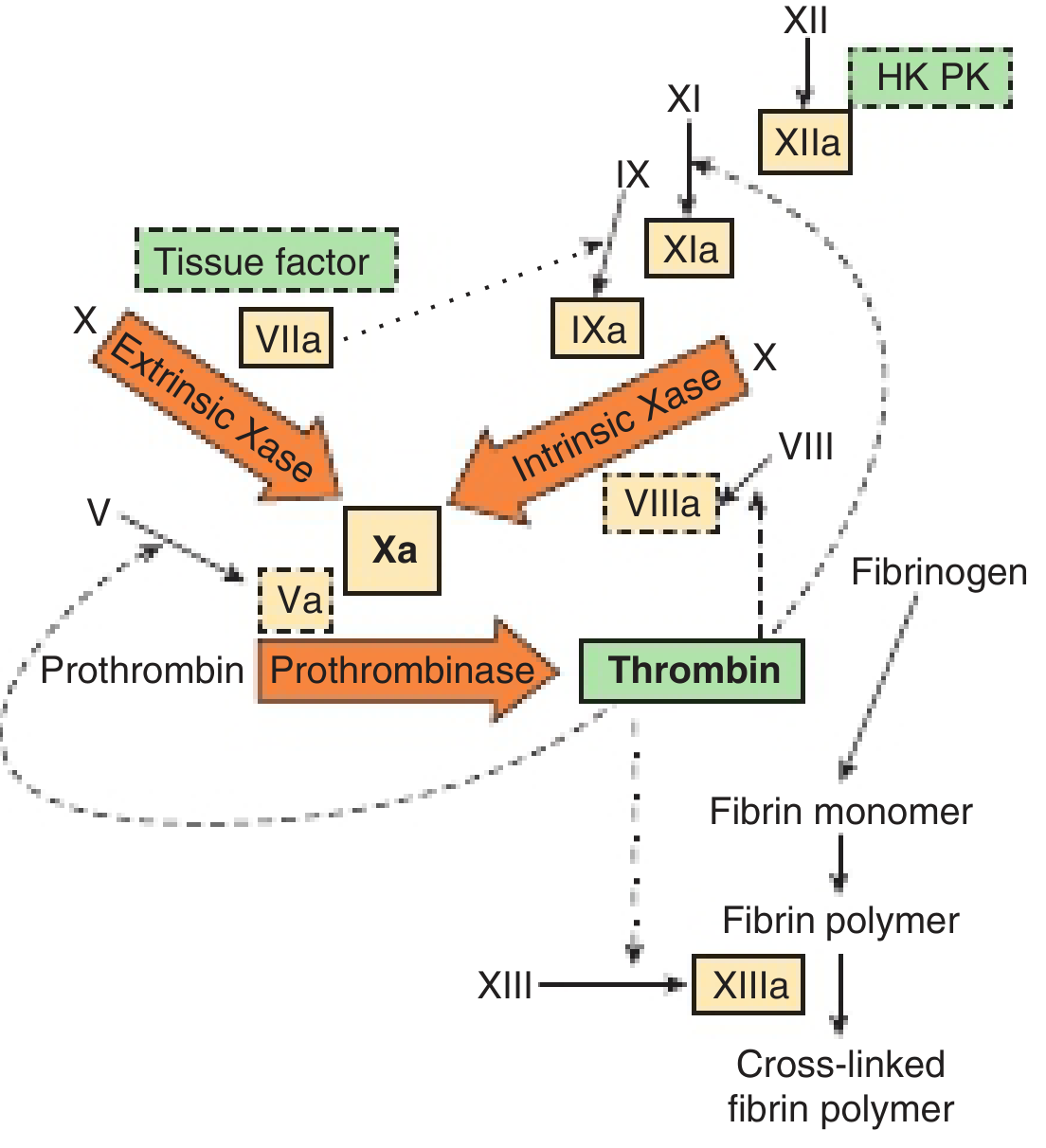
Extrinsic Xase (top left), Intrinsic Xase (top right), and Prothrombinase (center) converge on thrombin. Dashed arrows = thrombin feedback loops. HK = high-molecular-weight kininogen; PK = prekallikrein.
Factor Nomenclature Summary
| Factor | Name | Role |
|---|---|---|
| I | Fibrinogen | Clot substrate |
| II | Prothrombin | → Thrombin (IIa) |
| III | Tissue factor | Initiator cofactor |
| V | Labile factor | Cofactor in prothrombinase |
| VII | Proconvertin | Extrinsic pathway |
| VIII | Antihemophilic A | Cofactor in intrinsic tenase |
| IX | Christmas factor | Intrinsic pathway |
| X | Stuart-Prower factor | Common pathway convergence |
| XI | PTA | Intrinsic amplification |
| XII | Hageman factor | Contact activation |
| XIII | Fibrin-stabilizing factor | Cross-links fibrin |
4. Natural Anticoagulant Mechanisms
To prevent runaway clot formation, four major systems counterbalance the cascade:
-
Antithrombin III (ATIII): Inactivates thrombin and other activated serine proteases. Heparin binds ATIII and dramatically accelerates these reactions. Naturally enhanced by heparan sulfate on endothelial surfaces.
-
Protein C / Protein S system: Thrombin binds thrombomodulin on intact endothelium → activates Protein C. Activated Protein C + Protein S cofactor destroys Factors Va and VIIIa, cutting off the amplification loop.
-
Tissue Factor Pathway Inhibitor (TFPI): Directly inhibits Factor Xa; the TFPI-Xa complex then inhibits the TF-VIIa complex. This is why the extrinsic pathway is limited early and the intrinsic amplification becomes necessary.
-
Fibrinolytic system: Plasminogen activators (t-PA, u-PA) from endothelium convert plasminogen → plasmin, which digests fibrin. Regulated by PAI-1 (plasminogen activator inhibitor-1).
- Goldman-Cecil Medicine 22e, p. 1799
Clinical Correlations
| Deficiency / Drug | Effect | Test Affected |
|---|---|---|
| Factor VIII (Hemophilia A) | Severe bleeding | aPTT ↑, PT normal |
| Factor IX (Hemophilia B) | Severe bleeding | aPTT ↑, PT normal |
| Factor VII deficiency | Moderate bleeding | PT ↑, aPTT normal |
| Warfarin | Inhibits II, VII, IX, X, Prot C & S | PT/INR ↑ |
| Heparin | Potentiates ATIII | aPTT ↑ |
| Factor XII deficiency | No clinical bleeding | aPTT ↑ |
| Vitamin K deficiency | Affects II, VII, IX, X | PT ↑ > aPTT ↑ |
| DIC | Consumption of all factors | PT ↑, aPTT ↑, platelets ↓, fibrinogen ↓ |
This is a shared conversation. Sign in to Orris to start your own chat.