Development of lungs 5m answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from The Developing Human (Moore & Persaud). Here is the full 5-mark answer:
Development of Lungs
(The Developing Human - Clinically Oriented Embryology)
1. Origin and Initial Formation
The respiratory system arises from the endoderm of the foregut. A respiratory diverticulum (lung bud) appears at the caudal end of the laryngotracheal groove during the 4th week of development. This bud grows into the surrounding splanchnic mesenchyme and divides into two primary bronchial buds, which elongate laterally into the pericardioperitoneal canals (primordia of pleural cavities).
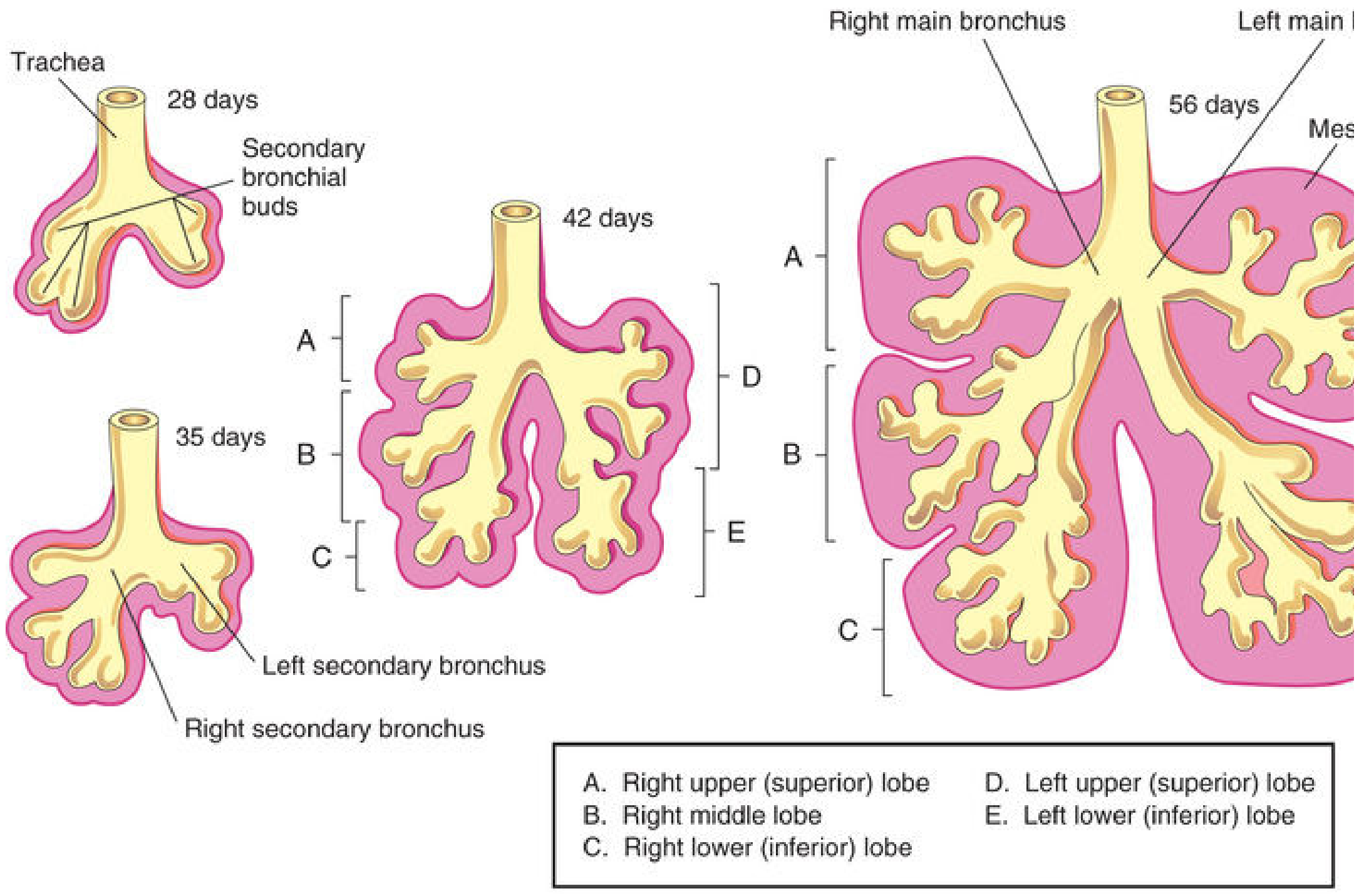
2. Bronchial Branching
- By the 5th week, primary bronchial buds enlarge to form the main (primary) bronchi.
- These subdivide into secondary (lobar) bronchi: 3 on the right (for upper, middle, and lower lobes) and 2 on the left (upper and lower lobes).
- Further branching produces segmental (tertiary) bronchi: 10 on the right, 8-9 on the left, beginning by the 7th week. Each segmental bronchus with surrounding mesenchyme forms a bronchopulmonary segment.
- By 24 weeks, approximately 17 orders of branches have formed, with respiratory bronchioles present. Seven additional orders develop postnatally.
Note: The right main bronchus is wider and more vertical than the left - hence aspirated foreign bodies preferentially enter the right lung.
3. Maturation Stages of the Lung (4 Overlapping Stages)
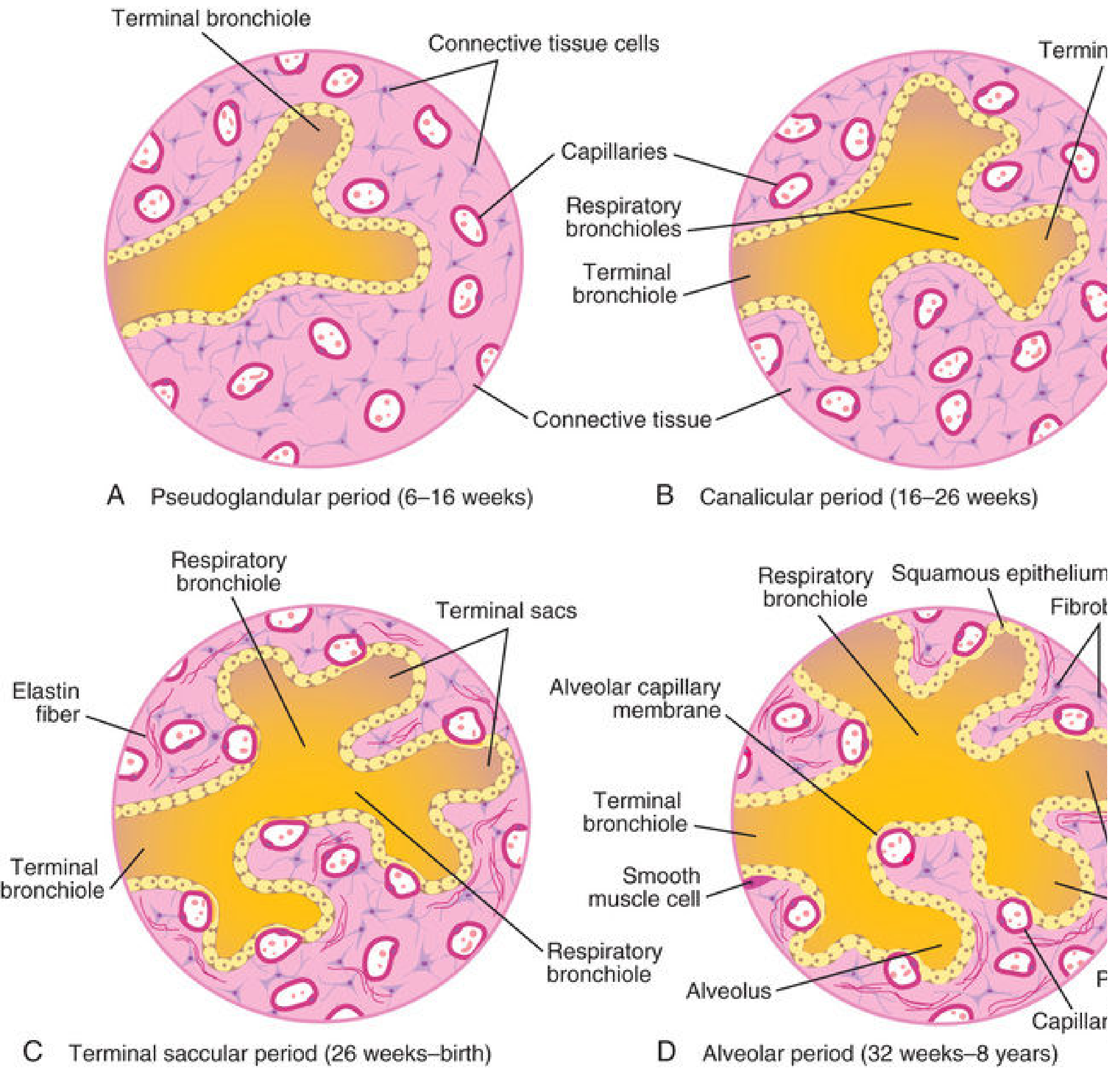
A. Pseudoglandular Stage (5-17 weeks)
- The developing lung resembles an exocrine gland histologically.
- All major elements form except those involved in gas exchange.
- Respiration is not possible; a fetus born at this stage cannot survive.
B. Canalicular Stage (16-25 weeks)
- Lumina of bronchi and terminal bronchioles enlarge; lung becomes highly vascular.
- By 24 weeks, terminal bronchioles branch into 2+ respiratory bronchioles, each forming 3-6 primordial alveolar ducts.
- By 26 weeks, limited respiration is possible due to thin-walled terminal sacs and vascularization - premature survival is possible with intensive care.
C. Terminal Sac (Saccular) Stage (24 weeks - late fetal period)
- Many terminal sacs (primordial alveoli) develop with very thin epithelium.
- Capillaries bulge into sacs, forming the blood-air barrier.
- The sacs are lined by two cell types (both of endodermal origin):
- Type I pneumocytes (squamous) - for gas exchange
- Type II pneumocytes (rounded/secretory) - produce pulmonary surfactant (phospholipids + proteins)
- Surfactant begins at ~20-22 weeks but reaches adequate levels only by the late fetal period.
- By 26-28 weeks (~1000 g fetus), sufficient alveoli and surfactant allow premature survival.
- Antenatal corticosteroids induce surfactant production; postnatal surfactant replacement therapy is used for deficiency.
D. Alveolar Stage (Late fetal period - 8 years)
- By 32 weeks, terminal sacs analogous to mature alveoli are present.
- Type I pneumocytes become extremely thin; capillaries bulge into alveolar sacs forming the alveolocapillary (respiratory) membrane.
- By 38 weeks (late fetal), gas exchange is fully possible.
- At birth: ~150 million primordial alveoli (half the adult number).
- By 3 years: alveolar development largely complete.
- By 8 years: adult complement of ~300 million alveoli achieved.
- 95% of mature alveoli develop postnatally.
4. Pleura Formation
- Visceral pleura derives from splanchnic (visceral) mesoderm surrounding the lung buds.
- Parietal pleura derives from somatic (parietal) mesoderm lining the body wall.
- The pleural cavity is the space between these two layers.
5. Molecular Regulation
- Transcription factors: TTF-1 (thyroid transcription factor-1), HNF-3β, GATA-6.
- FGF10 from splanchnic mesenchyme induces respiratory bud formation.
- Wnt signaling (including Wnt7b) drives epithelial-mesenchymal interaction for branching morphogenesis.
- Sonic hedgehog (Shh) modulates FGF10 and controls bronchial bud branching and smooth muscle differentiation.
- Retinoic acid regulates Hox genes (a5, b5, c4) in the developing lung.
6. Fetal Breathing Movements (FBMs)
Fetal breathing movements occur before birth (detectable by ultrasound), causing aspiration of small amounts of amniotic fluid. These movements are essential for normal lung development and occur ~30% of the time during REM sleep.
Key Clinical Points
| Event | Gestational Age |
|---|---|
| Respiratory bud appears | Week 4 |
| Primary bronchi form | Week 5 |
| Segmental bronchi begin | Week 7 |
| Surfactant production begins | 20-22 weeks |
| Viable premature birth possible | 24-26 weeks |
| Adequate surfactant + alveoli for survival | 26-28 weeks |
| Alveolocapillary membrane functional | 38 weeks |
| Adult alveolar number reached | ~8 years |
Respiratory Distress Syndrome (RDS/HMD) results from surfactant deficiency in premature infants - treated with antenatal steroids and postnatal surfactant replacement.
Source: The Developing Human - Clinically Oriented Embryology, Chapter 10
This is a shared conversation. Sign in to Orris to start your own chat.