hernia
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"hernia repair"[MeSH Terms] AND "herniorrhaphy"[MeSH Terms]
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of hernias, drawn from multiple surgical textbooks.
Hernia: Complete Overview
Definition
A hernia is the protrusion of a viscus (or part of a viscus) through a defect or weakness in the wall of the cavity in which it normally lies. The three components are:
- Sac - a peritoneal pouch
- Contents - bowel, omentum, or other abdominal viscera
- Coverings - layers of abdominal wall overlying the sac
Classification
By Reducibility
| Term | Meaning |
|---|---|
| Reducible | Contents can be returned to the abdominal cavity spontaneously or manually |
| Irreducible / Incarcerated | Contents cannot be reduced; not necessarily an emergency if blood supply is intact |
| Strangulated | Ischemia or obstruction from compression at the hernia neck - a surgical emergency |
By Location: Abdominal Wall (External) Hernias
Types of Hernia
1. Inguinal Hernia (most common overall)
The lifetime risk is 27-43% in males and 3-6% in females (Sabiston Textbook of Surgery).
The key anatomical landmark is Hesselbach's (inguinal) triangle, bounded by:
- Lateral border of the rectus sheath (medially)
- Inferior epigastric vessels (superolaterally)
- Inguinal ligament (inferiorly)
| Type | Exit point | Key feature |
|---|---|---|
| Direct | Medial to inferior epigastric vessels, through Hesselbach's triangle | Acquired; posterior wall weakness; outside spermatic cord |
| Indirect | Lateral to inferior epigastric vessels, through the deep inguinal ring | Due to patent processus vaginalis; hernia sac becomes part of spermatic cord |
| Pantaloon | Combination of direct + indirect | Difficult to diagnose/reduce in the ED; often found at surgery |
In children, 99% of inguinal hernias are indirect (congenital); direct hernias account for only 0.5% (Mulholland & Greenfield's Surgery).
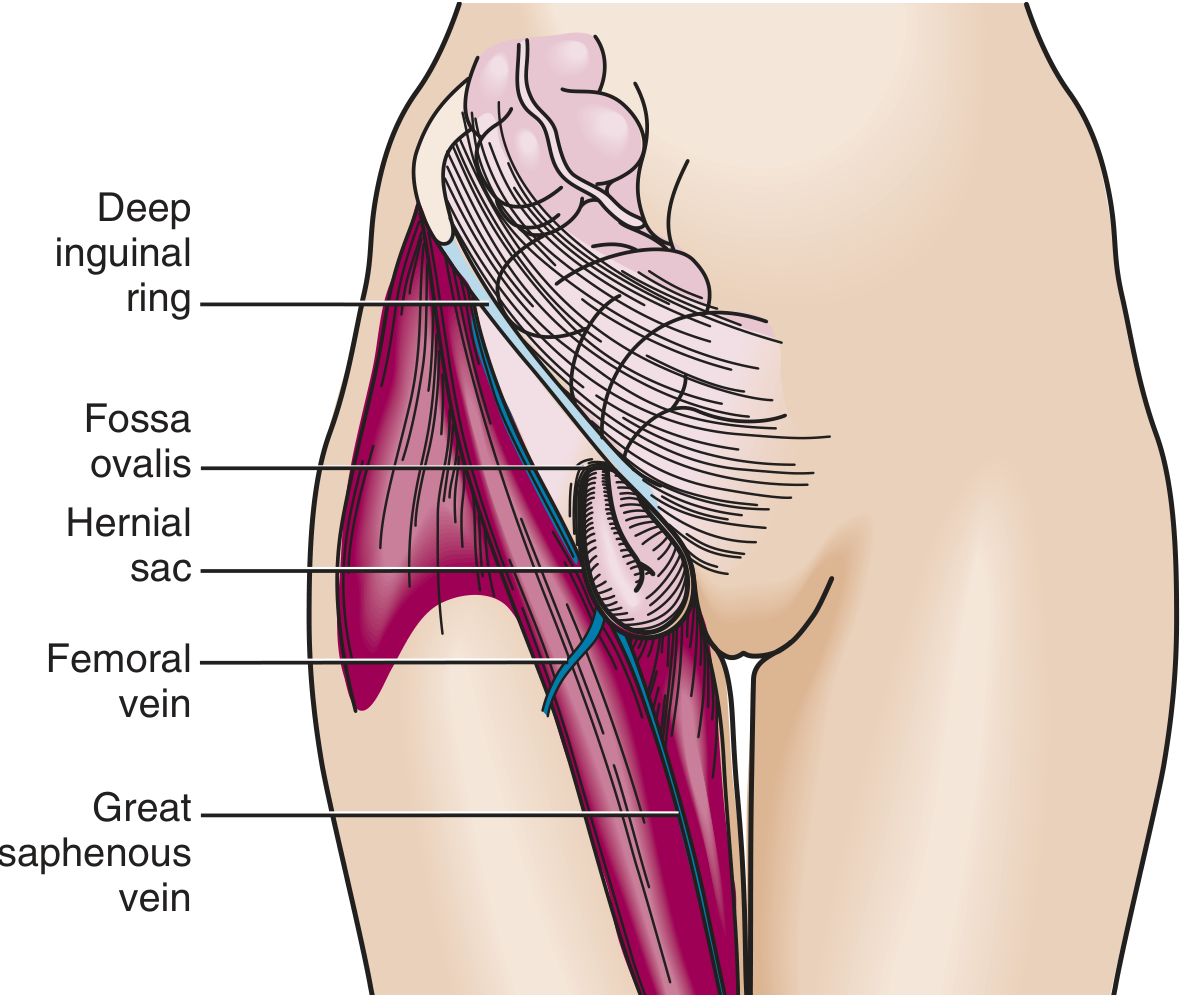
2. Femoral Hernia
- Exits inferior to the inguinal ligament through a defect in the transversalis fascia
- Contents enter the femoral canal: medial to the femoral vein, lateral to the lacunar ligament
- Appears as a mass in the medial thigh below the groin crease
- Relatively uncommon; more frequent in women
- High incarceration risk: up to 45% of cases (Roberts and Hedges' Emergency Medicine)
- Up to 40% are strangulated at initial presentation (Tintinalli's Emergency Medicine)
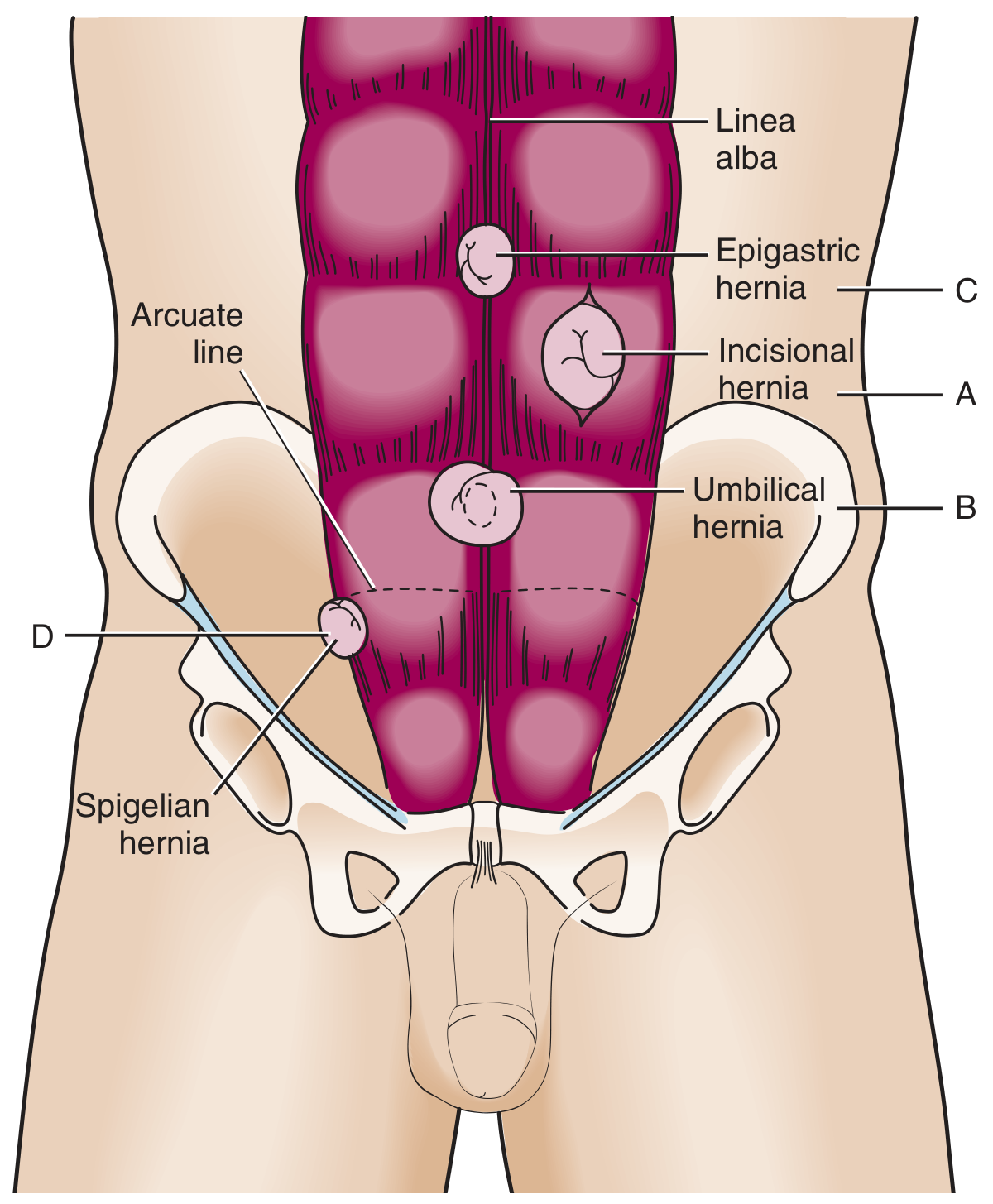
3. Umbilical Hernia
- Traverses the fibromuscular ring of the umbilicus
- Common in infants/children - congenital, often resolves by age 5 without treatment
- Surgical repair if: persists beyond age 5, size >2 cm, or if incarcerated/strangulated
- Adults: acquired; associated with obesity, ascites, pregnancy; more prone to strangulation than in children
- Accounts for ~15% of emergency hernia surgery; strangulation seen in up to 60% at operation (Sleisenger & Fordtran)
4. Incisional Hernia
- Occurs in up to 1 in 5 patients after abdominal surgery
- Poor wound healing (e.g., infection) increases risk
- Recurrence rate of 20-50% after repair
- Larger defects have a lower risk of strangulation (paradoxically, wider neck = less constriction)
5. Epigastric Hernia
- Midline, through the linea alba, between xiphoid and umbilicus
- Usually small and contains preperitoneal fat in adults
- Found in ~4% of pediatric patients evaluated for hernias
6. Spigelian Hernia
- Rare; through a defect at the lateral edge of the rectus muscle at the level of the arcuate (semilunar) line
- Often interparietal (between muscle layers), making it difficult to detect clinically
7. Hiatal Hernia
Classified into four types:
| Type | Description | Notes |
|---|---|---|
| Type I (sliding) | Gastroesophageal junction (GEJ) migrates above the diaphragm | 90-95% of hiatal hernias; mainly causes GERD |
| Type II (paraesophageal) | Gastric fundus herniates alongside esophagus; GEJ remains below diaphragm | True paraesophageal hernia |
| Type III (mixed) | Both GEJ and stomach herniate | Most common "paraesophageal" hernia seen clinically |
| Type IV | Other viscera (colon, spleen, omentum) also herniate | Diagnosed with CT |
Most sliding hernias are asymptomatic or cause heartburn/regurgitation. Paraesophageal hernias risk gastric volvulus and require surgical repair.
8. Internal Hernias
- Congenital types: mostly paraduodenal or through the foramen of Winslow
- Most common type is iatrogenic - after Roux-en-Y gastric bypass, colectomy, or pancreaticoduodenectomy (mesenteric defect)
- Also: obturator hernia and sciatic hernia (uncommon)
Pathophysiology
Hernia formation is multifactorial. Factors implicated include:
- Deficiency of elastic fibers in the transversalis fascia
- Decreased tropoelastin and lysyl oxidase-like 1 synthesis
- Overexpression of matrix metalloproteinases (MMPs) and elastase
- TGF-beta1 overexpression
- Raised intra-abdominal pressure (obesity, chronic cough, constipation, ascites)
Complications
Incarceration
- Hernia is irreducible but not necessarily ischemic
- Chronically incarcerated hernias (due to adhesions) may be painless with normal overlying skin
- An acutely incarcerated, painful hernia requires careful assessment
- Taxis (manual reduction technique): Trendelenburg position + gentle guiding pressure at the neck - NEVER forceful; contraindicated if strangulation is suspected
- "Reduction en masse" is a danger - the constricting ring comes in with the bowel
Strangulation
- Ischemia/obstruction from compression at the hernia neck
- Signs: severe tenderness, skin erythema, fever, peritonism
- A surgical emergency - prompt exploration required
- Strangulation risk is inversely proportional to the size of the defect (small neck = higher risk)
- Among patients undergoing surgery for hernia-related small bowel obstruction: ischemia in up to 75% and necrosis in more than 25% (Sleisenger & Fordtran)
Obstruction (Hernia Accident)
- Bowel obstruction from incarceration historically prompted prophylactic repair of all hernias
- However, randomized controlled trials have shown that watchful waiting is safe for asymptomatic inguinal hernias in men (Mulholland & Greenfield's Surgery)
Diagnosis
- Clinical: Visible/palpable lump; increases with coughing/straining; history of groin/abdominal swelling
- Hernia examination: Standing and supine; cough impulse; reducibility; transillumination (differentiates hydrocele - transilluminates; hernia - does not)
- Imaging:
- Ultrasound: useful for groin hernias, especially in obese patients
- CT: best for incisional hernias, internal hernias, and complex/obese cases; CT confirms incarceration and strangulation (pneumatosis, free fluid)
- Barium study: useful for hiatal hernias (though sliding hernias may reduce spontaneously)
Surgical Management
Inguinal Hernia Repair Options
Open repairs (tension-free mesh - preferred):
- Lichtenstein repair - gold standard open approach; flat polypropylene mesh; tension-free
Open suture repairs (higher recurrence, less used):
- Bassini, Shouldice, Desarda, Maloney darn
Laparoscopic/robotic approaches:
- TEP (Total Extraperitoneal) - preperitoneal dissection without entering the peritoneal cavity
- TAPP (Transabdominal Preperitoneal) - laparoscopic entry into the peritoneum then preperitoneal mesh
The European Hernia Society recommends either Lichtenstein open repair or total extraperitoneal (TEP) laparoscopic approach - results are comparable for both (Yamada's Gastroenterology).
Key principle: Mesh repairs have lower recurrence rates than suture repairs. There is no significant difference between the various mesh repairs, or between open and laparoscopic. Specialist hernia surgeons achieve lower recurrence and chronic pain rates regardless of technique (Bailey & Love's Surgery).
Emergency Hernia Surgery
- ~5% of inguinal hernias present as an emergency
- ~20% require bowel resection at emergency repair
- Synthetic mesh is still acceptable in most emergency cases if appropriate antibiotics are given (unless significant contamination)
Postoperative Complications
| Timing | Complications |
|---|---|
| Immediate | Hematoma, bleeding (subcutaneous, or rarely iliac vessels), urinary retention, femoral nerve blockade from local anesthetic |
| Early (1 week) | Pain, bruising, seroma (more common if peritoneal sac left in situ), wound infection |
| Late | Recurrence (<5% at 5 years in specialist centers), chronic pain (>3 months post-op; affects ~20%; less common with laparoscopic approach); neuralgic pain from nerve irritation by mesh or suture |
Key High-Yield Points
- Indirect inguinal hernia is the most common hernia in both sexes
- Femoral hernias are uncommon but have the highest risk of strangulation at presentation
- Incarceration ≠ strangulation; strangulation implies ischemia and is a surgical emergency
- The "smaller the neck, the greater the strangulation risk" - hence femoral hernias strangulate more than incisional hernias
- Watchful waiting is acceptable for asymptomatic inguinal hernias in men
- Lichtenstein repair (open tension-free mesh) and TEP/TAPP (laparoscopic) are equivalent in outcomes
- Chronic pain after groin hernia repair is a major concern, affecting up to 20% of patients
Sources: Bailey and Love's Short Practice of Surgery 28e; Fischer's Mastery of Surgery 8e; Mulholland & Greenfield's Surgery 7e; Sleisenger & Fordtran's GI and Liver Disease; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Sabiston Textbook of Surgery; Tintinalli's Emergency Medicine; Yamada's Textbook of Gastroenterology
approach to hernia
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.