Worsening of stroke pt on day 7
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ischemic stroke" AND "neurological deterioration" AND "day 7"
Finding Sources
Finding Sources
Searching PubMed
"ischemic stroke" AND "neurological deterioration" AND "cause"
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive textbook material. Let me compile the full answer.
Worsening of Stroke Patient on Day 7
Neurological or clinical deterioration at day 7 post-ischemic stroke is a critical concern. The causes span neurological and systemic/medical categories.
Neurological Causes
1. Cerebral Edema (Most common early cause)
- Brain edema begins within hours of ischemic stroke and peaks at 72–120 hours (3–5 days), but mass effect and herniation can manifest and extend into day 7, especially in large infarcts.
- Particularly dangerous in younger patients and those with large-artery occlusion (MCA territory, "malignant" infarction).
- Edema is initially cytotoxic (grey matter), then vasogenic (white matter).
- No pharmacological agent is proven effective; corticosteroids are not indicated for ischemic cerebral edema.
- Management: osmotherapy (mannitol/hypertonic saline), head elevation, ICP monitoring, and decompressive hemicraniectomy for malignant MCA infarction.
- — Bradley and Daroff's Neurology in Clinical Practice, p. 1406
2. Hemorrhagic Transformation (HT)
- Petechial or confluent hemorrhage into infarcted tissue, more common in large cardioembolic strokes and after tPA administration.
- Typically occurs 24–72 hours but can occur up to 1 week.
- Risk factors: large infarct size, anticoagulation, hypertension, thrombolysis.
- — Bradley and Daroff's Neurology in Clinical Practice; Robbins Pathologic Basis of Disease
3. Stroke Progression / Recurrent Stroke
- Propagation of thrombus, re-embolism, or hemodynamic failure in borderzone regions.
- Stuttering or stepwise worsening is characteristic of lacunar or large-vessel atherosclerotic strokes.
- Assess for: inadequate antiplatelet/anticoagulation, new cardioembolic source, carotid stenosis.
- DAPT (aspirin + clopidogrel) for 21 days is recommended in minor stroke or high-risk TIA to prevent early recurrence.
- — Goldman-Cecil Medicine
4. Cerebral Vasospasm
- Relevant primarily in subarachnoid hemorrhage (SAH), where vasospasm peaks at days 5–14 and causes delayed cerebral ischemia. In SAH, day 7 is squarely in the danger window.
- — Fuster and Hurst's The Heart
5. Seizures
- Occur in <5% of ischemic stroke patients, but early post-stroke seizures (within first week) can mimic or cause apparent neurological worsening.
- Antiseizure medications should be initiated if a seizure occurs.
- — Bradley and Daroff's Neurology
6. Hydrocephalus
- Especially with cerebellar infarction — swelling can compress the brainstem and cause hydrocephalus, manifesting as drowsiness, Babinski signs, gaze paresis.
- Can present days after the initial event; surgical decompression (suboccipital craniectomy + ventricular drainage) may be needed urgently.
- — Adams and Victor's Principles of Neurology
Systemic / Medical Causes (Particularly Day 5–14)
"In the second through the fourth weeks, pneumonia is the most common cause of non-neurological death." — Bradley and Daroff's Neurology, p. 1407
| Complication | Notes |
|---|---|
| Aspiration pneumonia | From dysphagia; formal swallowing assessment is mandatory before oral intake |
| Urinary tract infection / Urosepsis | From indwelling catheters; remove as early as possible |
| DVT / Pulmonary embolism | Hemiparetic limb is high-risk; use LMWH (enoxaparin 40 mg OD) or UFH 5000 units BID; IPC if heparin contraindicated |
| Fever | Worsens ischemic injury; reduce aggressively regardless of cause |
| Cardiac arrhythmia / MI | Stroke can cause neurogenic cardiac dysfunction; ECG changes may appear |
| Hypo/Hyperglycemia | Both worsen outcomes; target near-euglycemia but avoid intensive control (increased hypoglycemia risk) |
| Electrolyte disturbances | Hyponatremia, etc. can cause CNS worsening |
| Decubitus ulcers / Immobility | Secondary infections, systemic SIRS |
| Hypertension drops | Sudden BP reduction in acute stroke → neurological decline (impaired autoregulation); avoid aggressive BP lowering unless > threshold or tPA given |
Systematic Approach at Day 7
Urgent steps:
- Repeat brain imaging (CT/MRI) — rule out hemorrhagic transformation, new infarct, expanding edema, hydrocephalus
- Vitals + fever workup — blood cultures, urine culture, CXR
- Cardiac monitoring — ECG, troponin, look for arrhythmia (new AF?)
- Glucose, electrolytes, CBC
- NIHSS reassessment — quantify deficit change
- Review medications — BP drugs given inappropriately? Anticoagulation started/withheld?
- Swallowing assessment — aspiration risk
Summary Table
| Timeframe | Most Likely Cause |
|---|---|
| Hours–Day 3 | Hemorrhagic transformation, progressive edema |
| Day 3–7 | Peak edema + herniation, DVT, early infection |
| Day 7 | Recurrent stroke/embolism, aspiration pneumonia, UTI, seizure, DVT/PE, vasospasm (if SAH) |
| Week 2–4 | Pneumonia becomes dominant non-neurological cause |
Day 7 sits at the intersection of peak medical complications beginning (infection, DVT) while neurological dangers (edema, HT, recurrence) are still present — making systematic evaluation essential.
Ring enchancing lesion and open ring enhancing
Finding Sources
Finding Sources
Searching Images
ring enhancing lesion brain MRI
Reading File
Reading File
Reading File
Searching Images
open ring enhancing lesion demyelination multiple sclerosis MRI
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Now I have rich material from multiple authoritative sources. Here's the comprehensive answer:
Ring-Enhancing Lesions & Open-Ring Enhancing Lesions
What is Ring Enhancement?
Ring enhancement on contrast MRI (gadolinium) or contrast CT represents breakdown of the blood-brain barrier with passive leakage of contrast from the intravascular to the interstitial space in a peripheral rim, surrounding a central area that does not enhance (necrosis, pus, or demyelinated tissue).
Causes of Ring-Enhancing Lesions
Mnemonic: "MAGIC DR"
| Cause | Key Features |
|---|---|
| Metastasis | Most common in adults >45 yrs; multiple lesions at grey-white junction; thick irregular ring |
| Abscess (pyogenic) | Smooth, thin, uniform ring; DWI bright (restricted diffusion) — key distinguisher |
| Glioblastoma (GBM) | Thick, irregular, nodular ring; crosses corpus callosum ("butterfly"); no restricted diffusion |
| Infection — Toxoplasma | Multiple, bilateral; basal ganglia; in HIV (CD4 <100); empirically treated first |
| CNS Lymphoma | Periventricular; may be ring-enhancing (50%); solid enhancement more common; immunocompromised |
| Demyelination (MS) | Open-ring pattern — see below |
| Radionecrosis / Tuberculoma | Post-RT; tuberculoma at grey-white junction; solid or ring |
The Open-Ring (Incomplete Ring) Sign
This is the single most important distinguishing feature in ring-enhancing lesion radiology.
"Incomplete (open) ring enhancement differentiates MS from tumours/abscess. This open ring pattern reflects the less inflammatory reaction of the cortical component of the MS lesion, with less blood-brain barrier disruption and as consequence no contrast uptake." — Grainger & Allison's Diagnostic Radiology
Mechanism
- The open/incomplete side of the ring faces the cortical grey matter
- Grey matter side has less BBB disruption → no enhancement there
- White matter side has active inflammatory demyelination → enhances
Key facts about the open-ring sign:
- Highly specific for demyelinating disease (MS, tumefactive MS, acute disseminated encephalomyelitis — ADEM)
- ~50% of tumefactive MS lesions show this pattern
- Ring is open on the grey-matter side (cortical aspect)
- Rapid suppression by steroid treatment
- Enhancement duration: median 3.1 weeks; rarely beyond 2–3 months (if persistent → suspect neoplasm, sarcoidosis, vascular malformation)
- May evolve from nodular → ring pattern over time
Key Radiological Comparison Table
| Feature | Abscess | GBM/Metastasis | MS (Open Ring) |
|---|---|---|---|
| Ring completeness | Complete, thin, smooth | Complete, thick, irregular | Incomplete (open on grey matter side) |
| DWI | Bright (restricted ↑) | Iso/dark | Variable; may show restricted diffusion at margin |
| ADC | Low | Normal/High | Variable |
| Edema | Marked | Marked | Variable |
| Multiplicity | Single or multiple (satellite lesions) | Multiple (mets) / Single (GBM) | Multiple, bilateral |
| Location | White matter, cortex | Grey-white junction | Periventricular, juxtacortical, corpus callosum (Dawson fingers) |
| Perfusion (rCBV) | Low in rim | High in GBM rim | Lower |
| Daughter lesions | Yes (satellite abscess) | No | No |
| Corpus callosum crossing | No | Yes (GBM "butterfly") | Possible (inferior margin) |
Illustrated Comparison
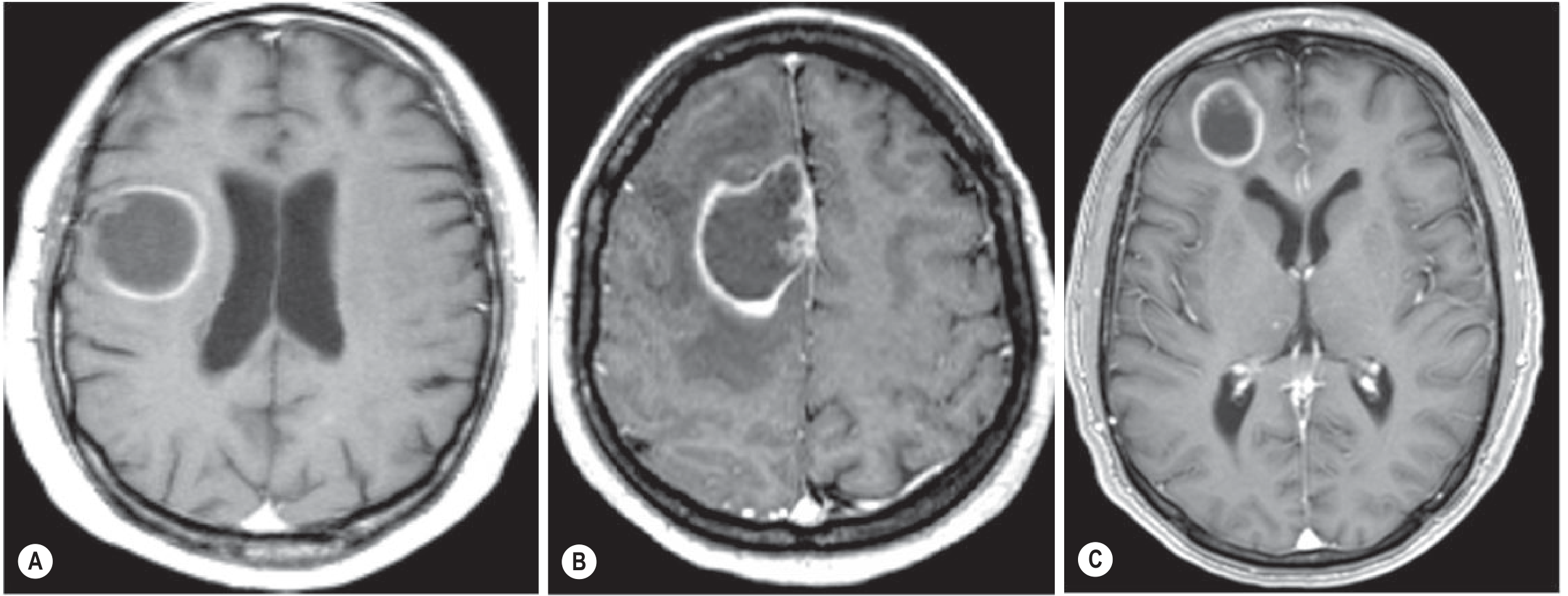
Fig. 58.12 from Grainger & Allison's Diagnostic Radiology — (A) MS pseudotumoral lesion with open/incomplete ring facing grey matter; (B) GBM with complete ring despite grey matter contact; (C) Brain metastasis with complete ring enhancement.
Brain Abscess — Specific Ring Features
The abscess capsule matures in stages (Harrison's Principles):
- Days 1–3: Early cerebritis — irregular enhancement, no ring yet
- Days 4–9: Late cerebritis — early ring formation
- Days 10–13: Ring-enhancing capsule appears (better developed on cortical side than ventricular side)
- Day 14+: Complete, well-formed ring with dense collagenous capsule
Radiological hallmarks:
- Smooth, thin, uniform ring (vs thick/nodular in tumour)
- DWI bright / ADC dark — restricted diffusion in the pus core is the best differentiator from tumour
- Surrounding vasogenic edema
- Satellite/daughter abscesses are characteristic
- Lower rCBV in enhancing rim vs GBM (perfusion MRI)
- A thick, irregular rim → favours tumour
"Though typical, the appearance of a brain abscess as a rim-enhancing mass is non-specific and may be mimicked by metastasis, glioblastoma and resolving haematoma. A thick, irregular rind of enhancement is more suggestive of tumour." — Grainger & Allison's Diagnostic Radiology
Clinical Approach to a Ring-Enhancing Lesion
- Immunocompromised (HIV, CD4 <100)? → Toxoplasma first (empirical treatment × 2 weeks, repeat imaging)
- If no response → CNS lymphoma (biopsy)
- DWI bright core? → Brain abscess → neurosurgery (aspiration) + antibiotics
- Open ring (incomplete), periventricular, young patient? → Demyelination (MS/ADEM) → steroids
- Thick irregular ring, old patient, known primary cancer? → Metastasis
- Butterfly across corpus callosum? → GBM
- Immunocompetent + single ring + positive tuberculin/endemic area? → Tuberculoma
Sources: Grainger & Allison's Diagnostic Radiology; Bradley and Daroff's Neurology in Clinical Practice; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Adams and Victor's Principles of Neurology
Clinically differentiate atonal vs demyelinating neuropathy on history examination
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.