in detail essay answer on orbital apex syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
"orbital apex syndrome" diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
orbital apex syndrome anatomy superior orbital fissure optic canal
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compose the detailed essay.
Orbital Apex Syndrome: A Detailed Essay
1. Introduction
Orbital apex syndrome (OAS) is a complex neuro-ophthalmologic emergency characterized by simultaneous dysfunction of multiple cranial nerves and the optic nerve due to a lesion at the posterior orbital apex. It represents the most severe and complete form of posterior orbital involvement, distinguishing itself from the closely related superior orbital fissure syndrome by the additional involvement of the optic nerve (CN II). Because of the density of critical neurovascular structures converging at this narrow anatomical corridor, even a small lesion at the orbital apex can produce a catastrophic clinical picture. Prompt recognition, accurate diagnosis, and aggressive management are imperative to prevent permanent blindness and life-threatening complications.
2. Surgical Anatomy of the Orbital Apex
The orbital apex is the posterior apex of the bony orbit, formed primarily by the lesser wing of the sphenoid bone and its junction with the greater wing and the sphenoid body. Two critical apertures define this region:
2.1 The Optic Canal
- Transmits CN II (optic nerve) and the ophthalmic artery
- Bounded superiorly and laterally by the lesser wing of the sphenoid
- Separated from the superior orbital fissure by the optic strut (a bony bridge of the sphenoid)
- Measures approximately 5–6 mm in length and 4–5 mm in diameter
2.2 The Superior Orbital Fissure (SOF)
- A cleft between the greater and lesser wings of the sphenoid
- Transmits: CN III (oculomotor), CN IV (trochlear), CN VI (abducens), CN V1 (ophthalmic division of trigeminal — specifically the lacrimal, frontal, nasociliary, and other branches), the superior and inferior ophthalmic veins, and sympathetic fibers
- CN V2 (maxillary division) exits via the foramen rotundum and is therefore NOT involved in orbital apex syndrome — a key differentiating feature from cavernous sinus syndrome, where V2 can be affected

Orbital apex anatomy: the optic canal (OC) lies superomedially, separated from the superior orbital fissure (SOF) by the optic strut. The lesser wing (LWS) and greater wing (GWS) of the sphenoid bound the SOF.
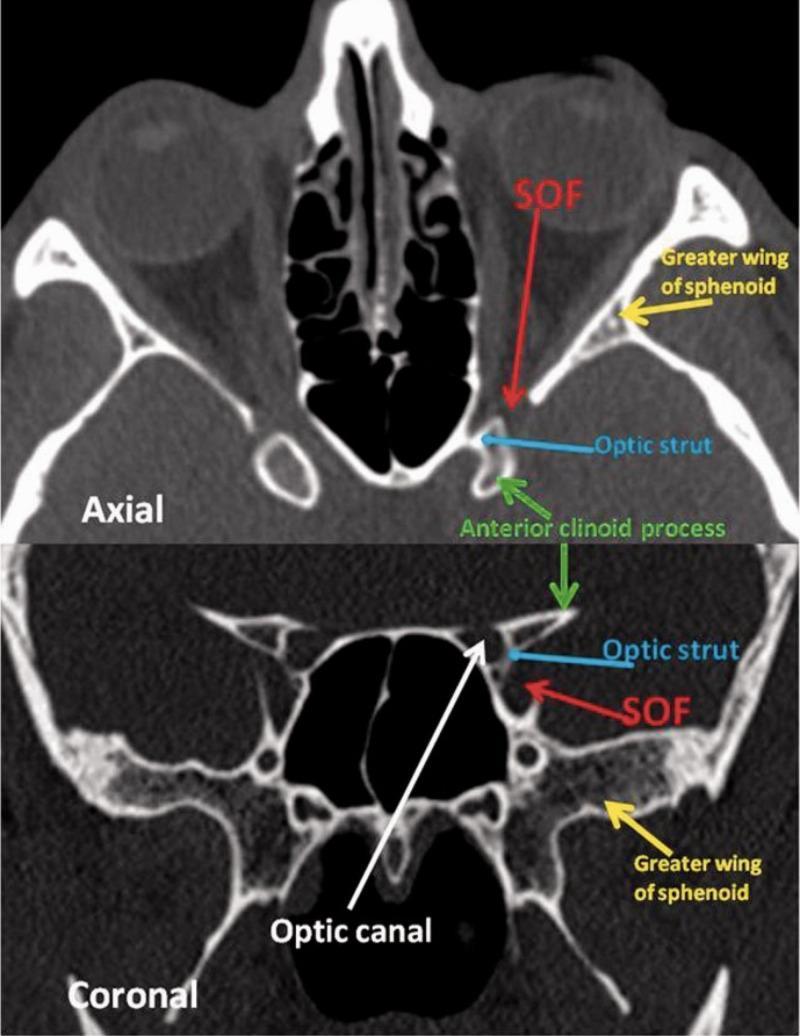
Axial and coronal CT (bone window) demonstrating the optic canal (white arrow), superior orbital fissure (red arrow), optic strut (blue arrow), anterior clinoid process (green), and greater wing of sphenoid (yellow).
The cavernous sinus lies contiguous with the orbital apex; thus, lesions can affect both structures simultaneously.
3. Cranial Nerve Involvement and Resulting Signs
Since OAS involves both the superior orbital fissure contents and the optic canal, the full syndrome encompasses:
| Structure Involved | Clinical Result |
|---|---|
| CN II (optic nerve) | Decreased visual acuity, visual field defects, afferent pupillary defect, optic atrophy |
| CN III (oculomotor) | Ptosis, internal ophthalmoplegia (fixed dilated pupil), medial/superior/inferior gaze palsy |
| CN IV (trochlear) | Weakness of downward and inward gaze |
| CN VI (abducens) | Lateral gaze palsy (most medially positioned in cavernous sinus near carotid) |
| CN V1 (ophthalmic) | Hypoesthesia/anesthesia of forehead, upper eyelid, cornea, conjunctiva; retrobulbar pain |
| Sympathetic fibers | Horner syndrome (may be masked by CN III palsy) |
| Ophthalmic veins | Proptosis, chemosis, conjunctival injection, orbital congestion |
The combination of complete external and internal ophthalmoplegia (paresis of CN III, IV, VI) with optic neuropathy (CN II) and ophthalmic sensory loss (CN V1) in the setting of proptosis defines the full syndrome. The key distinguishing feature from superior orbital fissure syndrome is the optic nerve involvement producing visual loss.
"Orbital apex syndrome occurs when the optic nerve is also involved, resulting in the preceding physical examination findings and diminished visual acuity." — Tintinalli's Emergency Medicine
"An orbital apex syndrome can be differentiated from cavernous sinus pathology by decreased visual acuity since the optic nerve passes through the orbital apex." — Rosen's Emergency Medicine
4. Etiology
OAS is a syndrome — a final common pathway — produced by diverse pathologies converging on the orbital apex. The major etiological categories are:
4.1 Infectious
- Fungal infections are among the most feared causes:
- Mucormycosis (Zygomycosis): Occurs predominantly in poorly controlled diabetics and immunosuppressed patients. The rhinocerebral form spreads from the nasal passages through the sphenoid sinus to the orbital apex, producing a rapidly fatal syndrome with ophthalmoplegia, facial numbness, visual loss, and characteristic violet/black discoloration of the nasal mucosa and eyelid tips. Requires emergency surgical debridement and amphotericin B; steroids are contraindicated.
- Aspergillosis: Can spread from nasal/sinus passages to the orbital apex. Also seen in immunosuppressed and diabetic patients. Biopsy is required for diagnosis; early antifungal therapy is essential.
- Bacterial orbital cellulitis: Direct spread from adjacent sinusitis (most often ethmoid or sphenoid sinusitis). Can progress to cavernous sinus thrombosis if untreated.
- Herpes Zoster Ophthalmicus (HZO): Reactivation of VZV in the ophthalmic division of the trigeminal nerve can produce OAS through direct neural inflammation, vasculitis, and perineural spread. Recent reviews (PMID 38108804; PMID 40998734) have highlighted this as an important and under-recognized cause, emphasizing the importance of antiviral therapy alongside corticosteroids.
- Tuberculosis, actinomycosis, and other granulomatous infections: Rare but well-documented.
4.2 Inflammatory / Idiopathic
- Orbital inflammatory pseudotumor (Idiopathic Orbital Inflammatory Syndrome): A pleomorphic inflammatory mass that can extend to the orbital apex. Associated with systemic rheumatologic disorders including Wegener's granulomatosis, giant cell arteritis, SLE, dermatomyositis, and rheumatoid arthritis.
- Tolosa-Hunt Syndrome: A granulomatous inflammation of the orbital apex and/or carotid siphon within the cavernous sinus. Presents with acute pain, cranial neuropathy, and sometimes proptosis. A diagnosis of exclusion requiring steroid responsiveness and exclusion of neoplasm.
- IgG4-Related Orbital Disease: Increasingly recognized as a cause of orbital apex involvement.
- Sarcoidosis: Can infiltrate the orbital apex producing a pseudotumor-like picture.
- Carotid-cavernous fistula: Produces venous congestion at the orbital apex.
4.3 Neoplastic
- Metastatic tumors: The orbital apex can be a site of haematogenous spread (breast, lung, prostate carcinoma).
- Direct extension: Nasopharyngeal carcinoma, sphenoid sinus tumors, meningioma, lymphoma can invade the orbital apex.
- Primary tumors: Lymphoma, perineural tumor spread, nerve sheath tumors.
- Note: Lymphoma and idiopathic pseudotumor may both be steroid-responsive, making lymphoma a diagnosis to actively consider before attributing response to idiopathic inflammation.
4.4 Traumatic
- Orbital fractures involving the orbital apex, particularly in high-energy trauma, can damage the optic nerve and nerves traversing the superior orbital fissure. Naso-orbito-ethmoid fractures require urgent neurosurgical and ophthalmological consultation.
4.5 Vascular
- Pituitary apoplexy: Hemorrhage within a pituitary tumor can extend into the cavernous sinus and orbital apex.
- Cavernous sinus thrombosis: May propagate to the orbital apex.
5. Clinical Presentation
The clinical picture depends on whether the syndrome is complete or partial (partial deficits are common with less severe lesions):
Core Features:
- Ophthalmoplegia: Total or partial (external + internal), due to CN III, IV, VI involvement. Diplopia is a common early symptom.
- Ptosis: Due to CN III paresis (levator palpebrae) and/or Horner syndrome (superior tarsal muscle).
- Fixed dilated pupil: Internal ophthalmoplegia from CN III involvement.
- Visual loss: Ranging from subtle visual field defects to complete blindness; afferent pupillary defect (Marcus Gunn pupil). This is the hallmark distinction from superior orbital fissure syndrome.
- Periorbital pain and hypoesthesia: From CN V1 involvement — hypesthesia/anesthesia of the forehead, upper eyelid, and cornea; retrobulbar neuralgia.
- Proptosis (exophthalmos): From impaired venous drainage via the superior and inferior ophthalmic veins and mass effect.
- Chemosis and conjunctival injection: Vascular engorgement from venous obstruction.
- Papilledema or optic atrophy: Depending on acuity and duration.
Systemic features provide etiological clues: fever and immunosuppression/diabetes in fungal infections; episodic pain with steroid responsiveness in Tolosa-Hunt; prior trauma; skin/systemic malignancy.
6. Differential Diagnosis
The most critical distinctions to make are:
| Syndrome | Structures Involved | Key Differentiator |
|---|---|---|
| Orbital Apex Syndrome | CN II, III, IV, VI, V1 | Visual loss (optic nerve) + proptosis |
| Superior Orbital Fissure Syndrome | CN III, IV, VI, V1 (NOT CN II) | No visual loss |
| Cavernous Sinus Syndrome | CN III, IV, VI, V1 ± V2 ± Horner | V2 may be involved; no proptosis typically; no optic nerve |
| Orbital Pseudotumor | Variable CN involvement | Response to steroids, no infection |
| Cavernous Sinus Thrombosis | Similar to cavernous sinus syndrome | Septic signs, bilateral involvement, hypercoagulable state |
7. Investigations
7.1 Imaging
- MRI orbit with gadolinium contrast is the investigation of choice: allows assessment for enhancement and enlargement of extraocular muscles, orbital structures, the optic nerve sheath, and the superior orbital fissure. Fat-suppressed sequences are critical.
- CT orbit with fine cuts (contrast-enhanced): More readily available, excellent for bony detail including fractures and sinus disease (particularly sphenoid sinusitis). Second-line to MRI.
- CT venography: If cavernous sinus thrombosis is suspected.
7.2 Microbiological and Pathological
- Biopsy: Mandatory when imaging and lumbar puncture do not yield a diagnosis and symptoms progress — emergency orbitotomy and biopsy are warranted in this scenario. Fungal infections can only be reliably diagnosed by biopsy.
- Blood cultures, ESR, CRP, CBC, HbA1c, serum glucose: Baseline workup.
- Immunological tests: ANA, ANCA, ACE level (sarcoidosis), serum IgG4.
- Lumbar puncture: CSF analysis for infection, malignancy.
7.3 Specific Tests
- VZV serology (PCR) if HZO suspected
- Fungal serology/cultures; tissue KOH preparation
- PET-CT or bone marrow biopsy if lymphoma suspected
8. Management
Management is directed entirely at the underlying etiology — there is no single treatment for OAS as a syndrome.
8.1 Infection
- Mucormycosis: Medical emergency. Urgent surgical debridement of necrotic tissue + IV amphotericin B (liposomal formulation preferred). Optimize glucose control. Steroids are contraindicated as they worsen fungal infections.
- Aspergillosis: Voriconazole is first-line; surgical debridement in severe cases.
- HZO: IV acyclovir (or valacyclovir) ± systemic corticosteroids. Recent evidence suggests corticosteroids combined with antivirals improve outcomes in HZO-associated OAS.
- Bacterial cellulitis/orbital abscess: IV antibiotics (cover gram-positive, gram-negative, and anaerobes); surgical drainage if abscess present.
8.2 Inflammatory / Idiopathic
- Orbital pseudotumor / Tolosa-Hunt: High-dose systemic corticosteroids are the mainstay — typically dramatic response confirms the diagnosis. Steroid-sparing immunosuppressives (methotrexate, azathioprine, mycophenolate) are used for relapsing or steroid-dependent cases. Antimetabolites and cytotoxic agents are increasingly used.
- IgG4-related: Rituximab may be considered for refractory disease.
8.3 Neoplastic
- Lymphoma: Chemotherapy ± radiotherapy (often steroid-responsive, which can confound diagnosis).
- Metastases: Radiation, systemic chemotherapy per primary tumor.
- Meningioma / direct invasion: Surgical resection ± adjuvant radiation.
8.4 Traumatic
- Optic nerve decompression may be considered in traumatic optic neuropathy. High-dose corticosteroids or surgical decompression depending on clinical trajectory.
8.5 Emergency Biopsy
When MRI with contrast and lumbar puncture do not yield a specific diagnosis and symptoms are progressing, emergency orbitotomy and biopsy are warranted.
9. Prognosis
Prognosis depends critically on:
- Speed of diagnosis and treatment: Fungal OAS carries a mortality of 50–80% if untreated or delayed; early surgical debridement and antifungal therapy dramatically improve outcomes.
- Underlying etiology: Inflammatory causes (pseudotumor, Tolosa-Hunt) have excellent responses to steroids. Metastatic disease carries the worst prognosis.
- Degree of optic nerve injury: Even with appropriate treatment, visual recovery may be incomplete if the optic nerve has sustained significant pressure injury or ischemia.
- Extraocular motility: CN III, IV, VI palsies may resolve partially or completely with treatment; aberrant regeneration can occur following CN III recovery.
10. Related Eponymous Syndromes
- Rollet Syndrome (Orbital Apex-Sphenoidal Syndrome): Lesions of the orbital apex causing CN III, IV, VI paresis with ptosis, diplopia, ophthalmoplegia, optic atrophy, hyperesthesia/anesthesia of the forehead and cornea, retrobulbar neuralgia, and possible exophthalmos and papilledema.
- Superior Orbital Fissure Syndrome (also sometimes called Orbital Apex Syndrome or Sphenoid Fissure Syndrome): Involvement of CN III, IV, V1, VI and the ophthalmic veins through the SOF but sparing CN II, without optic nerve involvement.
11. Summary
Orbital apex syndrome is a neurologic and ophthalmologic emergency caused by lesions compressing or infiltrating the orbital apex — the convergence zone of the optic canal and superior orbital fissure. The complete syndrome consists of optic neuropathy (CN II), ophthalmoplegia (CN III, IV, VI), sensory loss (CN V1), and proptosis. The key etiologies include fungal infections (especially mucormycosis and aspergillosis in diabetics/immunosuppressed), bacterial orbital cellulitis, neoplasms (metastases, lymphoma, direct extension), and idiopathic inflammatory conditions (pseudotumor, Tolosa-Hunt). Orbital MRI with gadolinium is the imaging modality of choice. Treatment targets the underlying cause: antifungals for fungi (never steroids), high-dose corticosteroids for idiopathic inflammation, and oncological therapy for neoplasia. Biopsy is mandatory when the cause remains uncertain and the condition progresses.
Sources:
- K.J. Lee's Essential Otolaryngology, 11th ed.
- Neuroanatomy Through Clinical Cases, 3rd ed. (Blumenfeld)
- Rosen's Emergency Medicine, 9th ed.
- Tintinalli's Emergency Medicine, 9th ed.
- Bradley and Daroff's Neurology in Clinical Practice, 8th ed.
- Grainger & Allison's Diagnostic Radiology, 7th ed.
- Li JXL et al. "Orbital apex syndrome in herpes zoster ophthalmicus." Orbit 2024; PMID 38108804
- Dupré R et al. "Orbital Apex Syndrome Secondary to Herpes Zoster Ophthalmicus." Semin Ophthalmol 2026; PMID 40998734
make a pdf of the whole information
Reading File
Running Command
ls /home/daytona/workspace/ 2>/dev/null && echo "---" && which weasyprint && whi…
Running Command
which pandoc && pandoc --version | head -1; python3 -c "from reportlab.lib.pages…
Running Command
mkdir -p /home/daytona/workspace/orbital-apex-essay
Writing File
~/orbital-apex-essay/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import ListFlowable, ListItem
OUTPUT = "/home/daytona/workspace/orbital-apex-essay/Orbital_Apex_Syndrome.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
rightMargin=2.2*cm,
leftMargin=2.2*cm,
topMargin=2.5*cm,
bottomMargin=2.5*cm,
title="Orbital Apex Syndrome",
author="Orris Medical AI",
subject="Neuro-Ophthalmology",
)
# ── Colour palette ──────────────────────────────────────────────────────────
NAVY = colors.HexColor("#0a2d6e")
TEAL = colors.HexColor("#1a7a7a")
LTBLUE = colors.HexColor("#ddeeff")
LTGREY = colors.HexColor("#f4f6f9")
DKGREY = colors.HexColor("#333333")
WHITE = colors.white
styles = getSampleStyleSheet()
# Custom styles
title_style = ParagraphStyle(
"Title", parent=styles["Title"],
fontSize=26, textColor=WHITE, alignment=TA_CENTER,
fontName="Helvetica-Bold", spaceAfter=4, leading=30,
)
subtitle_style = ParagraphStyle(
"Subtitle", parent=styles["Normal"],
fontSize=12, textColor=colors.HexColor("#cce0ff"),
alignment=TA_CENTER, fontName="Helvetica", spaceAfter=2,
)
h1_style = ParagraphStyle(
"H1", parent=styles["Heading1"],
fontSize=14, textColor=WHITE, fontName="Helvetica-Bold",
spaceAfter=6, spaceBefore=14, leading=18,
borderPad=(4, 6, 4, 6), backColor=NAVY,
leftIndent=0, rightIndent=0,
)
h2_style = ParagraphStyle(
"H2", parent=styles["Heading2"],
fontSize=12, textColor=NAVY, fontName="Helvetica-Bold",
spaceAfter=4, spaceBefore=10, leading=15,
borderWidth=0, leftIndent=0,
)
h3_style = ParagraphStyle(
"H3", parent=styles["Heading3"],
fontSize=11, textColor=TEAL, fontName="Helvetica-BoldOblique",
spaceAfter=3, spaceBefore=7, leading=14,
)
body_style = ParagraphStyle(
"Body", parent=styles["Normal"],
fontSize=10, textColor=DKGREY, fontName="Helvetica",
spaceAfter=6, leading=15, alignment=TA_JUSTIFY,
)
bullet_style = ParagraphStyle(
"Bullet", parent=body_style,
leftIndent=16, bulletIndent=6, spaceAfter=3,
)
source_style = ParagraphStyle(
"Source", parent=styles["Normal"],
fontSize=8.5, textColor=colors.HexColor("#555555"),
fontName="Helvetica-Oblique", spaceAfter=3, leading=12,
)
caption_style = ParagraphStyle(
"Caption", parent=styles["Normal"],
fontSize=8.5, textColor=colors.HexColor("#444444"),
fontName="Helvetica-Oblique", alignment=TA_CENTER,
spaceAfter=6, leading=11,
)
callout_style = ParagraphStyle(
"Callout", parent=styles["Normal"],
fontSize=10, textColor=NAVY, fontName="Helvetica-Oblique",
leftIndent=14, rightIndent=14, spaceAfter=8, spaceBefore=4,
leading=14, borderPad=8, borderWidth=1, borderColor=TEAL,
backColor=LTBLUE,
)
def h1(text):
return Paragraph(f" {text}", h1_style)
def h2(text):
return Paragraph(text, h2_style)
def h3(text):
return Paragraph(text, h3_style)
def p(text):
return Paragraph(text, body_style)
def b(items):
"""Return a list of bullet Paragraphs."""
return [Paragraph(f"• {item}", bullet_style) for item in items]
def callout(text):
return Paragraph(f'<i>"{text}"</i>', callout_style)
def sp(h=0.3):
return Spacer(1, h*cm)
def hr():
return HRFlowable(width="100%", thickness=0.5, color=colors.HexColor("#bbccdd"), spaceAfter=4)
def table(data, col_widths, header_row=True):
t = Table(data, colWidths=col_widths)
style_cmds = [
("FONTNAME", (0,0), (-1,-1), "Helvetica"),
("FONTSIZE", (0,0), (-1,-1), 9),
("VALIGN", (0,0), (-1,-1), "TOP"),
("ROWBACKGROUNDS", (0,1), (-1,-1), [WHITE, LTGREY]),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#cccccc")),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING",(0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING",(0,0), (-1,-1), 6),
("WORDWRAP", (0,0), (-1,-1), True),
]
if header_row:
style_cmds += [
("BACKGROUND", (0,0), (-1,0), NAVY),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 9.5),
]
t.setStyle(TableStyle(style_cmds))
return t
# ── Cover block builder ──────────────────────────────────────────────────────
def cover_table():
cover_data = [[
Paragraph("ORBITAL APEX SYNDROME", title_style),
]]
cover_sub = [[
Paragraph("A Comprehensive Medical Essay", subtitle_style),
]]
cover_meta = [[
Paragraph("Neuro-Ophthalmology | Emergency Medicine | Neurosurgery", subtitle_style),
]]
date_p = [[
Paragraph("Compiled: May 2026 | Orris Medical AI", subtitle_style),
]]
t = Table(
[cover_data[0], cover_sub[0], cover_meta[0], date_p[0]],
colWidths=[17*cm]
)
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), NAVY),
("TOPPADDING", (0,0), (-1,-1), 14),
("BOTTOMPADDING", (0,0), (-1,-1), 14),
("LEFTPADDING", (0,0), (-1,-1), 18),
("RIGHTPADDING", (0,0), (-1,-1), 18),
("ROWBACKGROUNDS",(0,0), (-1,-1), [NAVY]),
]))
return t
# ════════════════════════════════════════════════════════════════════════════
# DOCUMENT CONTENT
# ════════════════════════════════════════════════════════════════════════════
story = []
# ── Cover ──────────────────────────────────────────────────────────────────
story.append(sp(3))
story.append(cover_table())
story.append(sp(1.2))
story.append(hr())
story.append(sp(0.5))
story.append(p("Orbital apex syndrome (OAS) is a complex neuro-ophthalmologic emergency characterised by "
"simultaneous dysfunction of multiple cranial nerves and the optic nerve arising from a lesion "
"at the posterior orbital apex. It represents the most severe and complete form of posterior "
"orbital involvement, distinguishing itself from the closely related superior orbital fissure "
"syndrome by the additional involvement of the optic nerve (CN II). Because of the density of "
"critical neurovascular structures converging at this narrow anatomical corridor, even a small "
"lesion at the orbital apex can produce a catastrophic clinical picture. Prompt recognition, "
"accurate diagnosis, and aggressive management are imperative to prevent permanent blindness "
"and life-threatening complications."))
story.append(sp(0.4))
# ── 1. Anatomy ────────────────────────────────────────────────────────────
story.append(h1("1. Surgical Anatomy of the Orbital Apex"))
story.append(p("The orbital apex is the posterior apex of the bony orbit, formed primarily by the "
"<b>lesser wing of the sphenoid bone</b> and its junction with the greater wing and the "
"sphenoid body. Two critical apertures define this region:"))
story.append(sp())
story.append(h2("1.1 The Optic Canal"))
story += b([
"Transmits <b>CN II (optic nerve)</b> and the <b>ophthalmic artery</b>.",
"Bounded superiorly and laterally by the lesser wing of the sphenoid.",
"Separated from the superior orbital fissure by the <b>optic strut</b> — a bony bridge of the sphenoid.",
"Measures approximately 5–6 mm in length and 4–5 mm in diameter.",
])
story.append(sp())
story.append(h2("1.2 The Superior Orbital Fissure (SOF)"))
story.append(p("A cleft between the greater and lesser wings of the sphenoid, the SOF transmits:"))
story += b([
"<b>CN III</b> (oculomotor nerve)",
"<b>CN IV</b> (trochlear nerve)",
"<b>CN VI</b> (abducens nerve)",
"<b>CN V1</b> (ophthalmic division of trigeminal) — lacrimal, frontal, nasociliary, and other branches",
"<b>Superior and inferior ophthalmic veins</b>",
"<b>Sympathetic fibres</b> (from the cavernous sinus plexus)",
])
story.append(sp(0.3))
story.append(callout("CN V2 (maxillary division) exits via the foramen rotundum and is therefore NOT "
"involved in orbital apex syndrome — a key differentiating feature from cavernous "
"sinus syndrome, where V2 can be affected."))
story.append(p("The cavernous sinus lies contiguous with the orbital apex; thus, lesions can affect "
"both structures simultaneously, producing impaired venous drainage and vascular engorgement "
"of the orbital structures."))
story.append(sp(0.5))
# Anatomy table
story.append(h2("1.3 Structures at a Glance"))
anat_data = [
["Aperture", "Structures Transmitted", "Clinical Relevance"],
["Optic Canal", "CN II (optic nerve)\nOphthalmic artery", "Visual loss, afferent pupillary defect"],
["Superior Orbital\nFissure (SOF)", "CN III, CN IV, CN VI\nCN V1 (lacrimal, frontal, nasociliary)\nSup. & inf. ophthalmic veins\nSympathetics",
"Ophthalmoplegia, ptosis, pupil dilation,\nsensory loss, proptosis, Horner syndrome"],
["Foramen Rotundum\n(NOT involved in OAS)", "CN V2 (maxillary division)", "Spared in OAS; involved in cavernous sinus syndrome"],
]
story.append(table(anat_data, [3.5*cm, 6.5*cm, 6.0*cm]))
story.append(sp(0.5))
# ── 2. Cranial Nerve Involvement ──────────────────────────────────────────
story.append(h1("2. Cranial Nerve Involvement and Clinical Signs"))
story.append(p("Since OAS involves both the superior orbital fissure contents and the optic canal, "
"the full syndrome encompasses multiple cranial nerves simultaneously. Partial deficits "
"are common when the lesion is less severe or in an early phase."))
story.append(sp(0.3))
cn_data = [
["Structure", "Clinical Result"],
["CN II — Optic nerve", "Decreased visual acuity, visual field defects, afferent pupillary defect, optic atrophy"],
["CN III — Oculomotor", "Ptosis, internal ophthalmoplegia (fixed dilated pupil), paresis of medial/superior/inferior gaze"],
["CN IV — Trochlear", "Weakness of downward and inward gaze; oblique diplopia"],
["CN VI — Abducens", "Lateral gaze palsy; horizontal diplopia"],
["CN V1 — Ophthalmic", "Hypoaesthesia/anaesthesia of forehead, upper eyelid, cornea, conjunctiva; retrobulbar neuralgia"],
["Sympathetic fibres", "Horner syndrome (may be masked by CN III palsy): ptosis, miosis, anhidrosis"],
["Ophthalmic veins", "Proptosis (exophthalmos), chemosis, conjunctival injection, orbital congestion"],
]
story.append(table(cn_data, [4.5*cm, 12.0*cm]))
story.append(sp(0.4))
story.append(callout(
"The key distinguishing feature from superior orbital fissure syndrome is the optic nerve involvement "
"producing visual loss. "
"Orbital apex syndrome can be differentiated from cavernous sinus pathology by decreased visual acuity "
"since the optic nerve passes through the orbital apex. — Rosen's Emergency Medicine"
))
story.append(sp(0.5))
# ── 3. Etiology ───────────────────────────────────────────────────────────
story.append(h1("3. Aetiology"))
story.append(p("OAS is a syndrome — a final common pathway — produced by diverse pathologies converging "
"on the orbital apex. The major aetiological categories are:"))
story.append(h2("3.1 Infectious"))
story.append(h3("Fungal Infections (most feared)"))
story += b([
"<b>Mucormycosis (Zygomycosis):</b> Occurs predominantly in poorly controlled diabetics and "
"immunosuppressed patients. The rhinocerebral form spreads from the nasal passages through the "
"sphenoid sinus to the orbital apex. Produces rapidly fatal syndrome with ophthalmoplegia, facial "
"numbness, visual loss, and characteristic <b>violet/black discoloration</b> of nasal mucosa and "
"eyelid tips. Requires emergency surgical debridement and IV amphotericin B. "
"<b>Steroids are absolutely contraindicated.</b>",
"<b>Aspergillosis:</b> Can spread from nasal/sinus passages to the orbital apex. Seen in "
"immunosuppressed and diabetic patients. Biopsy is required for diagnosis.",
])
story.append(h3("Bacterial Infections"))
story += b([
"<b>Orbital cellulitis:</b> Direct spread from sinusitis (most often ethmoid or sphenoid). "
"Can progress to cavernous sinus thrombosis if untreated.",
"<b>Herpes Zoster Ophthalmicus (HZO):</b> VZV reactivation in CN V1 produces OAS through "
"direct neural inflammation, vasculitis, and perineural spread. Recent reviews (2024–2026) "
"highlight this as an important under-recognised cause.",
"<b>Other:</b> Tuberculosis, actinomycosis, and other granulomatous infections (rare).",
])
story.append(sp(0.2))
story.append(h2("3.2 Inflammatory / Idiopathic"))
story += b([
"<b>Orbital inflammatory pseudotumor (IOIS):</b> A pleomorphic inflammatory mass that can "
"extend to the orbital apex. Associated with systemic rheumatologic disorders (Wegener's "
"granulomatosis, GCA, SLE, dermatomyositis, rheumatoid arthritis).",
"<b>Tolosa-Hunt Syndrome:</b> Granulomatous inflammation of the orbital apex and/or carotid "
"siphon within the cavernous sinus. Presents with acute pain, cranial neuropathy, and "
"proptosis. Diagnosis of exclusion requiring steroid responsiveness.",
"<b>IgG4-Related Orbital Disease:</b> Increasingly recognised cause of orbital apex involvement.",
"<b>Sarcoidosis:</b> Infiltrative granulomatous involvement of the orbital apex.",
"<b>Carotid-cavernous fistula:</b> Venous congestion at the orbital apex.",
])
story.append(sp(0.2))
story.append(h2("3.3 Neoplastic"))
story += b([
"<b>Metastatic tumours:</b> Haematogenous spread from breast, lung, prostate carcinoma.",
"<b>Direct extension:</b> Nasopharyngeal carcinoma, sphenoid sinus tumours, meningioma, lymphoma.",
"<b>Primary tumours:</b> Lymphoma, perineural tumour spread, nerve sheath tumours.",
"<i>Important note:</i> Lymphoma and idiopathic pseudotumor may both be steroid-responsive — "
"lymphoma must be actively excluded before attributing response to idiopathic inflammation, "
"especially when pain is absent or disease recurs on steroid taper.",
])
story.append(sp(0.2))
story.append(h2("3.4 Traumatic"))
story += b([
"Orbital fractures involving the orbital apex, particularly in high-energy trauma (naso-orbito-ethmoid fractures).",
"Orbital fissure syndrome results from fracture of the orbit involving the SOF with injury to CN III and CN V1.",
"OAS occurs when the optic nerve is also involved, resulting in additional diminished visual acuity.",
"Retrobulbar haematoma causing compartment syndrome can compress the optic nerve acutely.",
])
story.append(sp(0.2))
story.append(h2("3.5 Vascular"))
story += b([
"<b>Pituitary apoplexy:</b> Haemorrhage within a pituitary tumour extending into the cavernous sinus and orbital apex.",
"<b>Cavernous sinus thrombosis:</b> May propagate to involve the orbital apex.",
"<b>Cavernous carotid aneurysm:</b> CN VI is typically involved first as it lies closest to the carotid artery.",
])
story.append(sp(0.5))
# Summary etiology table
story.append(h2("3.6 Aetiology Summary"))
etio_data = [
["Category", "Key Examples", "Special Features"],
["Fungal", "Mucormycosis, Aspergillosis", "Diabetic/immunosuppressed; biopsy required; no steroids"],
["Bacterial", "Orbital cellulitis, HZO", "Sinusitis origin; HZO — antiviral ± steroid"],
["Inflammatory", "Pseudotumor, Tolosa-Hunt, IgG4, Sarcoidosis", "Steroid-responsive; diagnose by exclusion"],
["Neoplastic", "Metastases, Lymphoma, Meningioma", "May mimic inflammation; biopsy essential"],
["Traumatic", "Orbital fracture, retrobulbar haematoma", "Urgent decompression may be needed"],
["Vascular", "Pituitary apoplexy, CC fistula", "Imaging/angiography required"],
]
story.append(table(etio_data, [3.2*cm, 5.5*cm, 7.8*cm]))
story.append(sp(0.5))
# ── 4. Clinical Presentation ─────────────────────────────────────────────
story.append(h1("4. Clinical Presentation"))
story.append(p("The clinical picture depends on whether the syndrome is <b>complete</b> or <b>partial</b>. "
"Partial deficits are common with less severe lesions or in the early phase. The following "
"constitute the core clinical features:"))
story.append(h2("Core Features"))
story += b([
"<b>Ophthalmoplegia (external ± internal):</b> Total or partial paralysis of extraocular movements "
"due to CN III, IV, VI paresis. Diplopia is often the earliest symptom.",
"<b>Ptosis:</b> Due to CN III paresis (levator palpebrae) and/or Horner syndrome (superior tarsal "
"muscle). Contributes to periorbital swelling.",
"<b>Fixed dilated pupil:</b> Internal ophthalmoplegia from CN III involvement. Pupil does not react "
"to light or convergence.",
"<b>Visual loss:</b> The hallmark distinguishing OAS from superior orbital fissure syndrome. Ranges "
"from subtle visual field defects to complete blindness. Afferent pupillary defect (Marcus Gunn "
"pupil) is present on swinging flashlight test.",
"<b>Periorbital pain and hypoaesthesia:</b> CN V1 involvement — hypesthesia/anaesthesia of the "
"forehead, upper eyelid, and cornea; retrobulbar neuralgia; photophobia.",
"<b>Proptosis (exophthalmos):</b> From impaired venous drainage and/or mass effect in the orbit.",
"<b>Chemosis and conjunctival injection:</b> Vascular engorgement from venous obstruction.",
"<b>Papilloedema or optic atrophy:</b> Depending on acuity and duration of compression.",
"<b>Horner syndrome:</b> From disruption of sympathetic fibres (ptosis, miosis, anhidrosis) — "
"may be difficult to appreciate if a CN III lesion is also present.",
])
story.append(sp(0.3))
story.append(callout(
"Both orbital inflammatory pseudotumor and orbital apex syndrome may result in proptosis, "
"chemosis, and/or conjunctival injection. With orbital apex syndrome, there may be dysfunction "
"of CNs II, III, IV, V, and VI. — Rosen's Emergency Medicine"
))
story.append(h2("Systemic Clues to Aetiology"))
story += b([
"Fever + immunosuppression/poorly controlled diabetes → fungal infection (mucormycosis)",
"Violet-black nasal/eyelid discolouration → mucormycosis",
"Episodic orbital pain + steroid response → Tolosa-Hunt syndrome",
"Known malignancy → metastatic disease",
"Recent facial trauma → traumatic OAS / orbital fracture",
"Vesicular periorbital rash → Herpes Zoster Ophthalmicus",
"Bilateral involvement + thyroid disease → Graves orbitopathy (consider differential)",
])
story.append(sp(0.5))
# ── 5. Differential Diagnosis ─────────────────────────────────────────────
story.append(h1("5. Differential Diagnosis"))
story.append(p("The most critical clinical distinctions are among posterior orbital and cavernous sinus "
"syndromes:"))
story.append(sp(0.2))
diff_data = [
["Syndrome", "CN Involved", "Key Differentiator"],
["Orbital Apex Syndrome", "II, III, IV, VI, V1", "Visual loss (optic nerve) + proptosis; V2 spared"],
["Superior Orbital Fissure Syndrome", "III, IV, VI, V1 (NOT II)", "No visual loss; V2 spared"],
["Cavernous Sinus Syndrome", "III, IV, VI, V1 ± V2 ± Horner", "V2 may be involved; no proptosis typically"],
["Orbital Pseudotumor", "Variable CN involvement", "Steroid-responsive; systemic rheumatologic association"],
["Cavernous Sinus Thrombosis", "Similar to cavernous sinus syndrome", "Septic signs; bilateral; hypercoagulable state"],
["Pituitary Apoplexy", "III, IV, VI ± II", "Sudden severe headache; visual field defect; MRI pituitary"],
]
story.append(table(diff_data, [4.5*cm, 4.2*cm, 7.8*cm]))
story.append(sp(0.5))
# ── 6. Investigations ─────────────────────────────────────────────────────
story.append(h1("6. Investigations"))
story.append(h2("6.1 Imaging"))
story += b([
"<b>MRI orbit with gadolinium contrast (investigation of choice):</b> Allows assessment for "
"enhancement and enlargement of extraocular muscles, orbital structures, the optic nerve sheath, "
"and the superior orbital fissure. Fat-suppressed (STIR/fat-sat) sequences are critical for "
"detecting orbital fat infiltration at the apex. Provides superior soft-tissue characterisation "
"compared with CT.",
"<b>CT orbit with fine cuts (contrast-enhanced):</b> More readily available; excellent for bony "
"detail including fractures and sinus disease (particularly sphenoid sinusitis). Second-line to "
"MRI. Useful in the emergency setting.",
"<b>CT venography:</b> If cavernous sinus thrombosis is suspected.",
"<b>MR angiography / digital subtraction angiography:</b> If carotid-cavernous fistula or "
"aneurysm is suspected.",
])
story.append(sp(0.2))
story.append(h2("6.2 Microbiological and Pathological"))
story += b([
"<b>Biopsy (emergency orbitotomy):</b> Mandatory when imaging and lumbar puncture do not yield "
"a diagnosis and symptoms are progressing. Fungal infections and lymphoma can only be reliably "
"diagnosed by tissue.",
"Blood cultures, ESR, CRP, CBC, HbA1c, serum glucose — baseline workup.",
"Immunological panel: ANA, ANCA, ACE level (sarcoidosis), serum IgG4, serum protein electrophoresis.",
"Fungal serology/cultures; tissue KOH preparation; culture on Sabouraud's medium.",
])
story.append(sp(0.2))
story.append(h2("6.3 Other Investigations"))
story += b([
"Lumbar puncture: CSF analysis for infection (including fungal culture), malignant cells, oligoclonal bands.",
"VZV PCR/serology if HZO is suspected.",
"PET-CT or bone marrow biopsy if lymphoma is suspected.",
"Thyroid function tests if Graves disease is in the differential.",
"Erythrocyte sedimentation rate (ESR) and CRP in all elderly patients (rule out giant cell arteritis).",
])
story.append(sp(0.5))
# ── 7. Management ─────────────────────────────────────────────────────────
story.append(h1("7. Management"))
story.append(p("Management is directed entirely at the <b>underlying aetiology</b>. There is no single "
"treatment for OAS as a syndrome. The approach should involve ophthalmology, neurology, "
"infectious disease, and/or neurosurgery as appropriate."))
story.append(h2("7.1 Infectious Causes"))
story.append(h3("Mucormycosis — Medical Emergency"))
story += b([
"Urgent <b>surgical debridement</b> of all necrotic tissue (nasal/sinus/orbital) — cornerstone of management.",
"<b>IV Liposomal Amphotericin B</b> at 5–10 mg/kg/day — antifungal of choice.",
"Optimise blood glucose control aggressively.",
"<b>Steroids are absolutely contraindicated</b> — they worsen fungal infections and can be fatal.",
"Isavuconazole or posaconazole may be used as step-down or salvage therapy.",
])
story.append(h3("Aspergillosis"))
story += b([
"<b>Voriconazole</b> is first-line antifungal therapy.",
"Surgical debridement in severe or progressive cases.",
])
story.append(h3("Herpes Zoster Ophthalmicus"))
story += b([
"IV <b>Acyclovir</b> (10 mg/kg every 8 h) or high-dose oral valacyclovir.",
"Systemic corticosteroids combined with antivirals — recent evidence (PMID 38108804, PMID 40998734) "
"supports improved outcomes.",
"Ophthalmology follow-up within 24–48 hours.",
])
story.append(h3("Bacterial Orbital Cellulitis"))
story += b([
"IV broad-spectrum antibiotics covering gram-positive, gram-negative, and anaerobes.",
"Surgical drainage if abscess is present.",
"CT/MRI to define extent of spread.",
])
story.append(sp(0.2))
story.append(h2("7.2 Inflammatory / Idiopathic Causes"))
story += b([
"<b>High-dose systemic corticosteroids</b> are the mainstay for orbital pseudotumor and Tolosa-Hunt "
"syndrome — typically a dramatic response confirms the diagnosis.",
"Steroid-sparing immunosuppressives (methotrexate, azathioprine, mycophenolate mofetil) for "
"relapsing or steroid-dependent cases.",
"Antimetabolites and cytotoxic agents are increasingly used in refractory IOIS.",
"<b>Rituximab</b> may be considered for IgG4-related orbital disease refractory to steroids.",
"<i>Caution:</i> If fungal infection cannot be excluded, avoid steroids until proven otherwise.",
])
story.append(sp(0.2))
story.append(h2("7.3 Neoplastic Causes"))
story += b([
"<b>Lymphoma:</b> Chemotherapy ± radiotherapy (often steroid-responsive — do not mistake for "
"idiopathic inflammation without tissue diagnosis).",
"<b>Metastases:</b> Radiation therapy ± systemic oncological treatment per primary tumour.",
"<b>Meningioma / direct invasion:</b> Surgical resection ± adjuvant radiation.",
])
story.append(sp(0.2))
story.append(h2("7.4 Traumatic Causes"))
story += b([
"Optic nerve decompression (surgical or endoscopic endonasal approach) for traumatic optic neuropathy.",
"High-dose corticosteroids: controversial; use case-by-case.",
"Emergency lateral canthotomy if retrobulbar haematoma with compartment syndrome.",
"Subspecialty consultation (ophthalmology, neurosurgery, facial surgery) before discharge.",
])
story.append(sp(0.2))
story.append(h2("7.5 Emergency Biopsy"))
story.append(callout(
"When MRI with contrast and lumbar puncture do not reveal a specific diagnosis and symptoms are "
"progressive, emergency orbitotomy and biopsy are warranted. "
"— Neuroanatomy Through Clinical Cases, 3rd Ed."
))
story.append(sp(0.5))
# Management algorithm table
story.append(h2("7.6 Management Algorithm Summary"))
mgmt_data = [
["Aetiology", "First-Line Treatment", "Key Cautions"],
["Mucormycosis", "Surgical debridement + IV Liposomal Amphotericin B", "AVOID steroids; optimise glucose"],
["Aspergillosis", "Voriconazole ± surgical debridement", "Biopsy required for diagnosis"],
["HZO", "IV Acyclovir + systemic corticosteroids", "Combine antiviral + steroid"],
["Bacterial cellulitis", "IV broad-spectrum antibiotics ± drainage", "CT/MRI to exclude abscess"],
["Pseudotumor / Tolosa-Hunt", "High-dose systemic corticosteroids", "Exclude fungal/lymphoma first"],
["Lymphoma", "Chemotherapy ± radiotherapy", "Biopsy before steroids if possible"],
["Metastases", "Radiation + systemic oncology", "Identify primary tumour"],
["Traumatic", "Decompression ± steroids", "Urgent ophthalmology + neurosurgery"],
["Unknown (progressive)", "Emergency orbitotomy + biopsy", "Do not delay biopsy"],
]
story.append(table(mgmt_data, [3.5*cm, 6.5*cm, 6.5*cm]))
story.append(sp(0.5))
# ── 8. Prognosis ──────────────────────────────────────────────────────────
story.append(h1("8. Prognosis"))
story.append(p("Prognosis depends critically on the speed of diagnosis and treatment, the underlying "
"aetiology, and the extent of optic nerve injury at presentation."))
story += b([
"<b>Fungal OAS</b> (especially mucormycosis) carries a mortality of <b>50–80%</b> if untreated or "
"delayed. Early surgical debridement and antifungal therapy dramatically improve survival.",
"<b>Inflammatory causes</b> (pseudotumor, Tolosa-Hunt) have excellent responses to corticosteroids "
"and a generally favourable prognosis for recovery of CN function.",
"<b>Metastatic/neoplastic disease</b> carries the worst long-term prognosis, depending on the "
"primary tumour.",
"<b>Visual recovery</b> may be incomplete even with appropriate treatment if the optic nerve has "
"sustained significant pressure injury, ischaemia, or demyelination.",
"<b>Extraocular motility:</b> CN III, IV, VI palsies may resolve partially or completely with "
"treatment. Aberrant regeneration can occur following CN III recovery.",
"<b>Herpes zoster OAS</b> may have prolonged CN deficits; prognosis is improving with early "
"combined antiviral and corticosteroid therapy.",
])
story.append(sp(0.5))
# ── 9. Related Eponyms ────────────────────────────────────────────────────
story.append(h1("9. Related Eponymous Syndromes"))
story.append(sp(0.2))
epo_data = [
["Syndrome", "Structures Involved", "Description"],
["Orbital Apex Syndrome\n(Full)", "CN II, III, IV, VI, V1 +\nOphthalmic veins", "Optic nerve + SOF + orbital vein involvement"],
["Superior Orbital Fissure\nSyndrome", "CN III, IV, VI, V1\n(NOT CN II)", "SOF contents only; no optic nerve; no visual loss"],
["Rollet Syndrome\n(Orbital Apex-Sphenoidal)", "CN III, IV, VI +\nOptic + CN V1", "Ptosis, diplopia, ophthalmoplegia, optic atrophy,\nhyperaesthesia/anaesthesia, retrobulbar neuralgia,\nexophthalmos, papilloedema"],
["Cavernous Sinus Syndrome", "CN III, IV, VI, V1 ± V2\n± Horner", "V2 may be involved; no proptosis typically;\nno optic nerve involvement"],
["Tolosa-Hunt Syndrome", "CN III, IV, VI, V1", "Idiopathic granulomatous inflammation of orbital apex\nand/or cavernous sinus; diagnosis of exclusion;\nsteroid-responsive"],
]
story.append(table(epo_data, [4.0*cm, 4.0*cm, 8.5*cm]))
story.append(sp(0.5))
# ── 10. Summary Box ───────────────────────────────────────────────────────
story.append(h1("10. Summary"))
story.append(callout(
"Orbital apex syndrome is a neurologic and ophthalmologic emergency caused by lesions "
"compressing or infiltrating the orbital apex — the convergence zone of the optic canal "
"and superior orbital fissure. The complete syndrome consists of optic neuropathy (CN II), "
"ophthalmoplegia (CN III, IV, VI), sensory loss (CN V1), and proptosis. CN V2 is characteristically "
"spared, distinguishing it from cavernous sinus syndrome. Key aetiologies include fungal "
"infections (especially mucormycosis and aspergillosis in diabetics/immunosuppressed), bacterial "
"orbital cellulitis, neoplasms (metastases, lymphoma, direct extension), and idiopathic "
"inflammatory conditions (pseudotumor, Tolosa-Hunt syndrome). Orbital MRI with gadolinium is "
"the imaging modality of choice. Treatment targets the underlying cause: antifungals (never "
"steroids) for fungi, high-dose corticosteroids for idiopathic inflammation, and oncological "
"therapy for neoplasia. Emergency biopsy is mandatory when the cause remains uncertain and "
"the condition progresses."
))
story.append(sp(0.5))
# ── 11. References ────────────────────────────────────────────────────────
story.append(h1("11. References"))
refs = [
"K.J. Lee's Essential Otolaryngology, 11th Edition — Head and Neck Surgery.",
"Blumenfeld H. Neuroanatomy Through Clinical Cases, 3rd Edition. Sinauer Associates.",
"Rosen's Emergency Medicine: Concepts and Clinical Practice, 9th Edition. Elsevier.",
"Tintinalli JE. Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th Edition. McGraw-Hill.",
"Bradley and Daroff's Neurology in Clinical Practice, 8th Edition. Elsevier.",
"Grainger & Allison's Diagnostic Radiology: A Textbook, 7th Edition. Elsevier.",
"The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment, 8th Edition.",
"Localization in Clinical Neurology, 8th Edition. Wolters Kluwer.",
"Li JXL, Tong JY, Tumuluri K. Orbital apex syndrome in herpes zoster ophthalmicus: clinical features, "
"treatment and outcomes — a case series and literature review. Orbit. 2024 Dec. PMID: 38108804.",
"Dupré R, Grosse JP, Baillif S. Orbital Apex Syndrome Secondary to Herpes Zoster Ophthalmicus: "
"A Literature Review and In-Depth Understanding. Semin Ophthalmol. 2026 May. PMID: 40998734.",
"Borchard NA, Nayak JV. Orbital Apex Syndrome. N Engl J Med. 2018 Apr 26; 378(17): e23.",
]
for i, ref in enumerate(refs, 1):
story.append(Paragraph(f"[{i}] {ref}", source_style))
story.append(sp(0.1))
# ── Build ──────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF written to: {OUTPUT}")
Running Command
python3 /home/daytona/workspace/orbital-apex-essay/generate_pdf.py
Running Command
ls -lh /home/daytona/workspace/orbital-apex-essay/Orbital_Apex_Syndrome.pdf
The PDF has been generated successfully. You can download it here:
Orbital Apex Syndrome
PDF Document · PDF
What's included in the PDF:
The document is fully formatted with a navy-blue cover header and spans 11 sections:
- Surgical Anatomy — Optic canal, SOF, structures transmitted, anatomy summary table
- Cranial Nerve Involvement — Full table of all CN deficits and their clinical results
- Aetiology — Infectious (fungal, bacterial, HZO), inflammatory, neoplastic, traumatic, vascular — with summary table
- Clinical Presentation — Core features + systemic clues to aetiology
- Differential Diagnosis — OAS vs SOF syndrome vs cavernous sinus syndrome vs pseudotumor (comparison table)
- Investigations — MRI, CT, biopsy, labs, special tests
- Management — Per-aetiology treatment with algorithm summary table (including the critical "no steroids in mucormycosis" warning)
- Prognosis — Aetiology-specific outcomes
- Related Eponymous Syndromes — Rollet, SOF, Cavernous Sinus, Tolosa-Hunt (table)
- Summary — Highlighted callout box
- References — 11 textbook and PubMed sources
This is a shared conversation. Sign in to Orris to start your own chat.