comprehensively explain about tremors and their types
Reading File
Finding Sources
Searching the Web
tremor types classification pathophysiology clinical features 2024
Reading File
Reading File
Reading File
Searching PubMed
tremor classification types management
Reading File
Reading File
Searching PubMed
essential tremor pathophysiology treatment
Loading Image
Reading File
I have an extremely rich dataset. Now I have enough to write a comprehensive answer. Let me compile everything.
Tremors: A Comprehensive Overview
Definition
Tremor is defined as an involuntary, rhythmic, oscillatory movement produced by alternating or irregularly synchronous contractions of reciprocally innervated muscles. Its rhythmic quality distinguishes it from other involuntary movements (chorea, athetosis), and its oscillatory nature (both agonist and antagonist muscles activated - bidirectional movement) distinguishes it from myoclonus (monophasic jerk) and asterixis.
- Adams and Victor's Principles of Neurology, 12th Edition
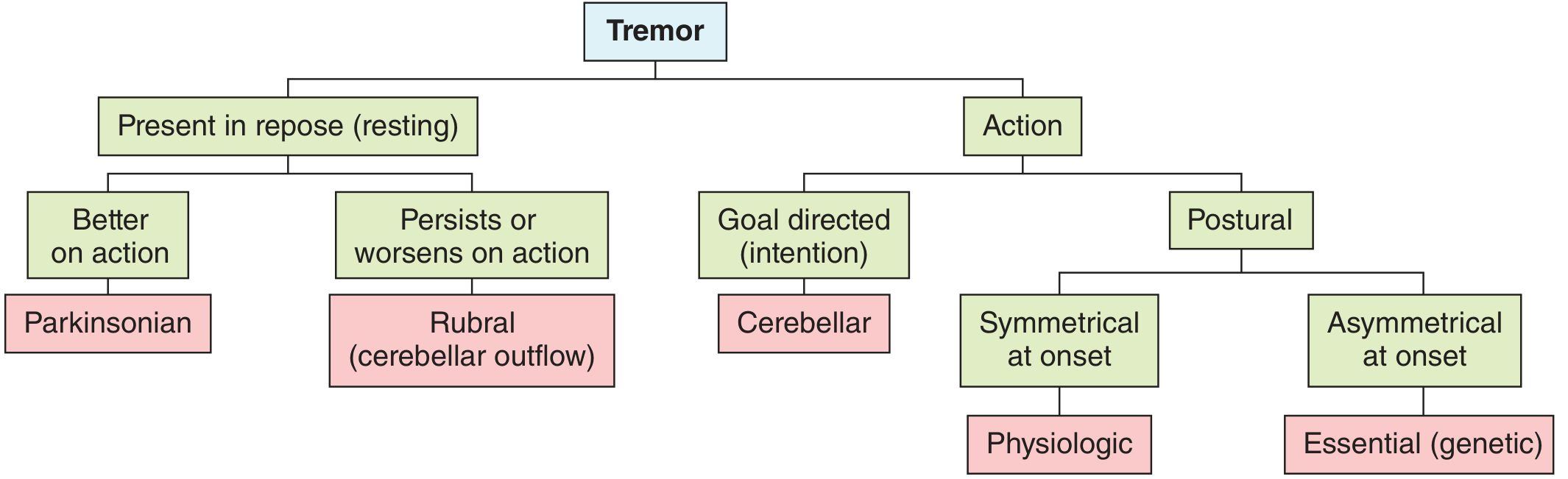
Classification Framework
Tremors are classified along two key axes:
- Activation conditions - when the tremor appears (rest vs. action)
- Etiology/Syndrome - the underlying cause
Major Types of Tremor
Summary Table (from Adams and Victor's)
| Type | Frequency (Hz) | Location | Enhanced by | Attenuated by |
|---|---|---|---|---|
| Physiologic (enhanced) | 8-13 | Hands | Epinephrine, beta-adrenergic | Alcohol, beta-blockers |
| Parkinsonian (rest) | 3-5 | Hands, forearms, fingers, feet, lips, tongue | Emotional stress | L-dopa, anticholinergics |
| Cerebellar (intention/rubral) | 2-4 | Limbs, trunk, head | Emotional stress | - |
| Postural/action | 5-8 | Hands | Anxiety, fright, alcohol withdrawal, xanthines, exercise | Beta-blockers (some cases) |
| Essential (familial/senile) | 4-8 | Hands, head, vocal cords | Anxiety, exercise, fatigue | Alcohol, propranolol, primidone |
| Orthostatic | 14-16 | Legs | Quiet standing | Repose, walking, clonazepam |
| Neuropathic | 4-7 | Hands | - | - |
| Palatal | 1-2 (60-100/min) | Palate, sometimes face, pharynx | - | Clonazepam, valproate |
| Dystonic | Irregular | Concordant with focal dystonia | - | Botulinum toxin |
1. Physiologic Tremor
Definition: A normal baseline tremor present in all healthy individuals. So fine it is barely visible to the naked eye.
- Frequency: 8-13 Hz in the hands; as slow as 6.5 Hz elsewhere
- Mechanism: Driven peripherally by mechanical-reflex oscillations and centrally by synchronized motor neuron discharges
- Not pathologic in itself
Enhanced (Exaggerated) Physiologic Tremor
When amplitude increases significantly, it becomes clinically apparent. Causes include:
- Physiologic states: Anxiety, fear, fright, exercise, fatigue
- Metabolic: Hyperthyroidism, hypoglycemia, hypercortisolism, pheochromocytoma, hypothermia
- Drugs and toxins: Lithium, nicotinic acid, xanthines (caffeine, aminophylline), cocaine, methamphetamine, corticosteroids, valproate, SSRIs, bronchodilators, cyclosporine, tacrolimus
- Withdrawal: Alcohol, benzodiazepines, barbiturates
- Mechanism: Enhancement in metabolic/toxic states is primarily due to stimulation of muscular beta-adrenergic receptors by elevated circulating catecholamines - NOT a CNS-mediated effect
- Treatment: Remove the cause; beta-adrenergic antagonists (propranolol)
2. Resting Tremor (Parkinsonian Tremor)
Definition: Tremor present when the affected limb is completely relaxed and supported against gravity. It diminishes or disappears with voluntary movement.
- Frequency: 3-5 Hz (some sources state 5-7 Hz)
- Location: Hands and forearms (most common), fingers, feet, lips, tongue, chin - notably not the head (head tremor favors essential tremor)
- Classic appearance: "Pill-rolling" tremor - appears as if the patient is rolling something between the thumb and other fingers
- Pattern: Asymmetrical at onset
- Enhanced by: Emotional stress, mental distraction (e.g., asking the patient to perform mental arithmetic while hands rest)
- Decreased by: Voluntary movement
Pathophysiology: Loss of dopaminergic neurons in the substantia nigra pars compacta, leading to disinhibition of the thalamus and altered basal ganglia-thalamo-cortical circuits. EMG shows alternating bursts in agonist and antagonist muscles (unlike action tremors).
Primary cause: Parkinson's disease - but parkinsonian tremor can also occur with drug-induced parkinsonism (neuroleptics, metoclopramide), multisystem atrophy, progressive supranuclear palsy, and other Parkinson-plus syndromes.
Treatment: Levodopa, dopamine agonists, anticholinergics (trihexyphenidyl), deep brain stimulation (DBS) of the subthalamic nucleus or globus pallidus interna.
3. Action Tremors
Action tremors appear when the limbs are in active use. They subdivide into:
a) Postural Tremor
- Occurs when a body part is maintained against gravity (e.g., arms held outstretched)
- Absent at rest; appears with muscle activation
- Best examples: Essential tremor, enhanced physiologic tremor
b) Kinetic Tremor
- Occurs during voluntary movement (not specifically goal-directed)
- Simple kinetic tremor: during any movement
- Task-specific tremor: only during particular tasks (e.g., writing, speaking)
- Primary writing tremor - a task-specific tremor that only occurs when writing or adopting a writing posture; no tremor in other conditions; frequency ~5-7 Hz
c) Intention Tremor (Goal-directed kinetic tremor)
- Tremor that increases in amplitude as the limb approaches a target
- Classic sign of cerebellar disease (appendicular cerebellar ataxia)
- Demonstrated by: Finger-nose-finger test, heel-shin test
- Also accompanied by: Dysmetria, dysdiadochokinesia, dysarthria, wide-based gait
- Frequency: 2-4 Hz (lower frequency, coarser)
- Pathophysiology: Loss of cerebellar modulation of motor output; the lateral cerebellar hemispheres and dentato-rubro-thalamo-cortical pathway are disrupted
d) Isometric Tremor
- Occurs during sustained muscle contraction without movement (e.g., squeezing a rigid object)
4. Essential Tremor
The most common movement disorder overall, with a prevalence of approximately 5% in adults.
- Frequency: 4-8 Hz (usually lower end of range), lower than physiologic tremor
- Location: Hands/arms (most common), head (titubation), vocal cords ("shaky voice"), tongue, lips; legs and trunk less often
- Pattern: Bilateral but may be asymmetrical
- Classic trigger: Posture and movement (postural + kinetic); absent at rest early on
- Worsened by: Anxiety, emotion, exercise, fatigue, caffeine
- Characteristic: Improves transiently with alcohol (a key differentiator from Parkinsonian tremor)
- Genetics: Autosomal dominant with high penetrance; previously called familial, benign, or senile tremor
- Functional impact: Can progress to illegible handwriting, inability to bring utensils or a glass to the mouth without spillage
Pathophysiology: Not fully understood. Involves oscillation in the cerebello-thalamo-cortical loop. Thalamic nucleus ventralis intermedius (Vim) shows synchronized burst discharges locked to the tremor frequency. A Purkinje cell-mediated "pacemaker" role has been proposed.
Treatment:
- First-line: Propranolol (beta-blocker) or primidone (antiepileptic)
- Second-line: Topiramate, gabapentin, clonazepam
- Alcohol (temporary, not a clinical option due to risk)
- Surgical: Thalamotomy (lesion of Vim) or DBS of the Vim nucleus - highly effective
- Focused ultrasound thalamotomy (newer option)
5. Cerebellar Tremor
- Intention tremor is the hallmark (see above), but cerebellar lesions also cause:
- Postural tremor at rest with limbs held in space (trunk and head titubation - associated with vermis lesions)
- Frequency: 2-4 Hz, coarse, low-frequency
- Associated signs: Dysmetria, dysarthria, nystagmus, ataxic gait, hypotonia
- Causes: Multiple sclerosis, stroke, tumors, alcohol-related cerebellar degeneration, spinocerebellar ataxias
6. Holmes Tremor (Rubral Tremor / Midbrain Tremor)
- A combination of rest + postural + intention tremor - the only tremor type with all three components
- Frequency: 2-4 Hz, low-frequency, often violent
- Usually unilateral
- Low amplitude at rest, but becomes coarse and violent as the limb is raised slightly or when movement is attempted
- Mechanism: Lesion involving the superior cerebellar peduncle (dentato-rubro-thalamic tract) near the red nucleus (midbrain)
- Causes: Multiple sclerosis, brainstem infarcts (midbrain stroke), trauma
- Can resemble the wing-beating tremor of Wilson's disease
- Neuroanatomy through Clinical Cases, 3rd Edition
7. Orthostatic Tremor
- A distinctive high-frequency (14-16 Hz) tremor, the fastest of all tremor types
- Occurs exclusively in the legs shortly after standing still; disappears when sitting, lying down, or walking
- Patients feel unsteady and have a tendency to fall if stationary
- Difficult to see visually; best diagnosed by palpating the thigh muscles while the patient stands or by EMG showing characteristic ~16 Hz bursts
- Treatment: Clonazepam, valproate, gabapentin
- Adams and Victor's Principles of Neurology
8. Palatal Tremor (formerly Palatal Myoclonus)
- Rhythmic movement of the soft palate at 0.5-5 Hz (60-100/min)
- Can extend to the face, pharynx, and proximal upper extremities
- Famous for persisting during sleep - a distinguishing feature from most other tremors
- May cause ear clicking due to Eustachian tube movement
- Two forms:
- Symptomatic: Due to lesions of the central tegmental tract or dentate-red nucleus-inferior olive circuit (infarcts, MS, trauma); associated with olivary hypertrophy on MRI
- Essential palatal tremor: No known cause; accompanied by ear clicking
- Treatment: Botulinum toxin injections into the tensor or levator veli palatini
- Neuroanatomy through Clinical Cases, 3rd Edition
9. Neuropathic Tremor
- Action tremor (relatively symmetric) associated with peripheral neuropathies
- Especially linked to chronic inflammatory demyelinating polyneuropathy (CIDP) and IgM paraproteinemic neuropathy
- Frequency: 4-7 Hz, involves hands
- Associated with positive Romberg sign and other neuropathy features
- Mechanism: Disruption of peripheral sensory feedback loops that normally damp tremor
10. Dystonic Tremor
- Tremor occurring in a body part affected by dystonia
- Irregular, jerky rhythm (not smooth sinusoidal oscillation)
- Location is concordant with the focal dystonia (e.g., cervical dystonic tremor with torticollis)
- May appear as head tremor, hand tremor, or voice tremor in the context of dystonia
- Treatment: Botulinum toxin injections; geste antagoniste (sensory trick) may temporarily suppress it
11. Drug-Induced Tremors
A wide range of agents can produce tremor (frequency 3-12 Hz). Main drug classes:
- Neuroleptics/antipsychotics - parkinsonian rest tremor
- Lithium - postural/action tremor, toxic doses → coarse tremor
- Valproate - action tremor (dose-dependent)
- Beta-adrenergic agonists (salbutamol, terbutaline) - enhanced physiologic
- SSRIs, tricyclics - enhanced physiologic
- Corticosteroids - enhanced physiologic
- Calcium channel blockers, amiodarone
- Immunosuppressants: cyclosporine, tacrolimus - can cause severe tremor
- Alcohol withdrawal - coarse postural/action tremor
- Management: Dose reduction or withdrawal of offending agent; beta-blockers if needed
12. Functional (Psychogenic) Tremor
A tremor without an organic neurologic basis, classified as a functional neurological disorder (FND).
Clinical features suggesting functional tremor:
- Abrupt onset, static course, spontaneous remissions
- Variable frequency (more specific than variable amplitude alone)
- Entrainment sign: When asked to copy a rhythmic tapping with the unaffected hand at a different frequency - the affected limb entrains to the same rhythm, stops, or the patient cannot copy the movement
- Ballistic movement test: Brief stopping of tremor during fast ballistic movements with the other hand
- Distractibility: Tremor diminishes with mental distraction (mental arithmetic) - opposite to organic tremor
- Loading sign: Adding wrist weights worsens functional tremor (organic tremor improves with loading)
- Coactivation sign: Simultaneous agonist-antagonist activation, resembling voluntary shivering
- Coherence: If bilateral, both limbs tremor at the exact same frequency (organic tremors have slightly different frequencies in different limbs)
- Unresponsive to antitremor drugs; responds to psychotherapy/physiotherapy
- Normal dopamine transporter (DaT) scan
- Bradley and Daroff's Neurology in Clinical Practice
Pathophysiology: Common Neural Circuits
In virtually all pathologic tremors, rhythmic burst discharges are recorded from neurons in the nucleus intermedius ventralis (Vim) of the thalamus, synchronous with the tremor frequency. These neurons:
- Are arranged somatotopically
- Respond to kinesthetic inputs from involved muscles/joints
- Project to premotor cortex via the ventrolateral thalamo-cortical pathway
- Ultimately drive tremor via the lateral corticospinal tract
This is why thalamic lesion (thalamotomy) or DBS of Vim abolishes most tremor types - it interrupts pallidothalamic and dentothalamic projections before they reach the cortex.
Differential Diagnosis: Key Distinguishing Features
| Feature | Parkinsonian | Essential | Cerebellar (Intention) | Functional |
|---|---|---|---|---|
| Present at rest | Yes | No (mild later) | No | Variable |
| Worsens with movement | No (improves) | Yes (postural) | Yes (goal-directed) | Variable |
| Frequency | 3-5 Hz | 4-8 Hz | 2-4 Hz | Variable |
| Symmetry | Asymmetric | Bilateral | Unilateral | Variable |
| Head tremor | No | Yes | Yes (titubation) | Yes |
| Alcohol response | No effect | Improves | No effect | Variable |
| Associated signs | Bradykinesia, rigidity | Usually none | Dysmetria, ataxia | Distractible |
Treatment Overview
| Tremor Type | First-Line Treatment | Second-Line / Surgical |
|---|---|---|
| Essential | Propranolol, primidone | Topiramate, DBS (Vim), focused ultrasound |
| Parkinsonian | Levodopa, dopamine agonists | DBS (STN or GPi), anticholinergics |
| Cerebellar/intention | Clonazepam (limited) | Weights on limbs; DBS (less effective) |
| Orthostatic | Clonazepam, gabapentin | Valproate |
| Palatal | Botulinum toxin | Clonazepam, valproate |
| Dystonic | Botulinum toxin | Anticholinergics |
| Enhanced physiologic | Remove cause; propranolol | - |
| Functional | Physiotherapy, CBT | No antitremor drugs |
Recent Evidence Note
A 2026 systematic review and meta-analysis (PMID 40878368) confirmed that botulinum toxin is effective for upper limb tremor in both essential tremor and dystonic tremor, supporting its use when oral agents fail or cause intolerable side effects.
Sources:
- Adams and Victor's Principles of Neurology, 12th Edition - Chapter 4: Tremor, Myoclonus, Focal Dystonias
- Neuroanatomy through Clinical Cases, 3rd Edition - Chapter 16: Movement Disorders
- Bradley and Daroff's Neurology in Clinical Practice - Functional/Psychogenic Movement Disorders
- MDS Task Force Classification of Tremor (Frontiers in Neurology, 2021)
- RACGP Tremor Review 2024
This is a shared conversation. Sign in to Orris to start your own chat.