Tonometers for 20 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information to write a detailed 20-mark answer on tonometers. Let me compile it.
Tonometers
Definition & Principle
A tonometer is an instrument used to measure intraocular pressure (IOP) by determining the ease of deforming the eye — an eye that deforms easily has low pressure. Normal IOP averages 15 mmHg (range ~10–21 mmHg). Pressures consistently above 21 mmHg are clinically significant; levels >25–30 mmHg sustained over time can cause glaucomatous optic nerve damage.
Tonometry is essential for:
- Diagnosis and monitoring of glaucoma
- Detecting acute angle-closure glaucoma (IOP may reach 60–70 mmHg)
- Monitoring response to treatment
Classification of Tonometers
1. Goldmann Applanation Tonometer (GAT) — Gold Standard
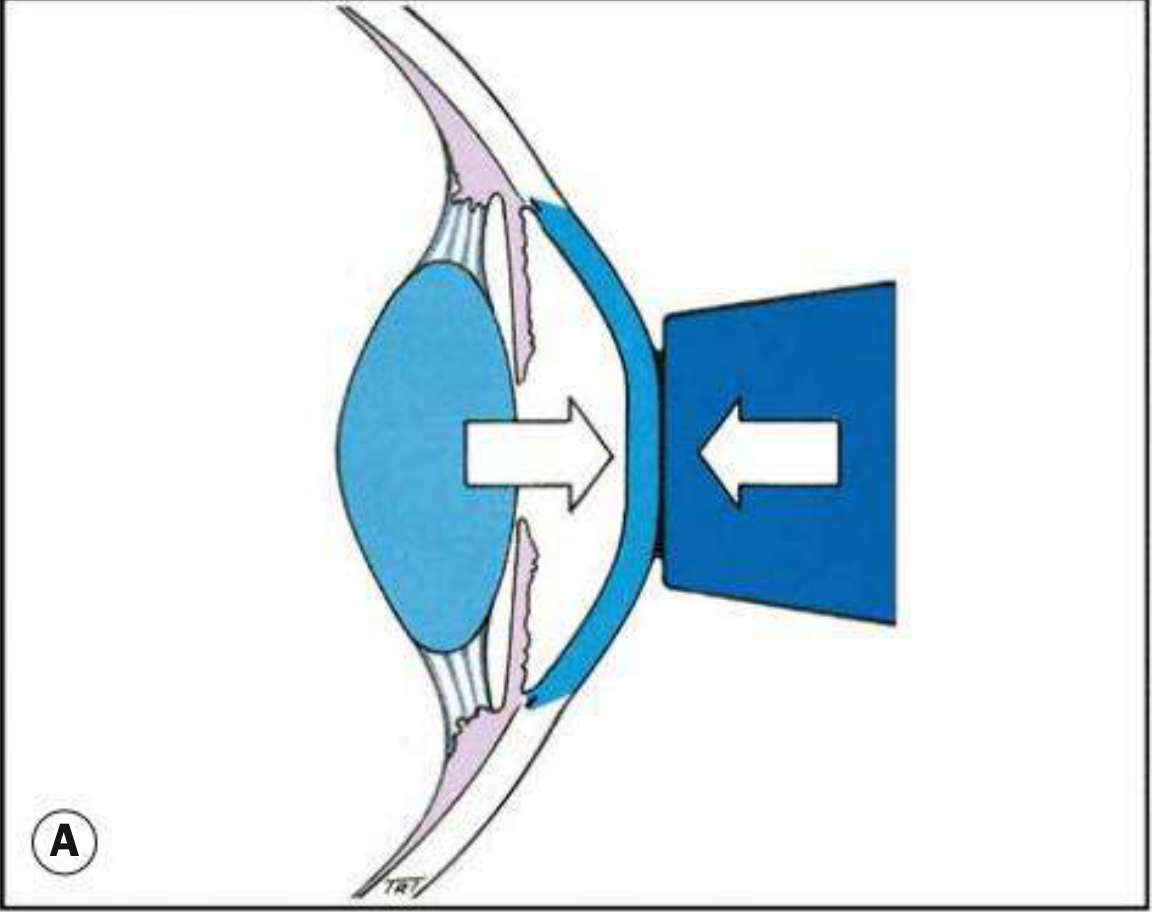
Principle (Imbert-Fick):
For an ideal, dry, thin-walled sphere: P = F/A (pressure = force/area of flattening). The cornea is not a perfect sphere — corneal rigidity tends to resist flattening, while capillary attraction of the tear meniscus pulls the prism toward the cornea. These two forces cancel each other out when the flattened area diameter is exactly 3.06 mm — this is the basis of Goldmann's design.
Instrument:
- Variable-force tonometer with a biprism mounted on a slit lamp
- The dial reading × 10 = IOP in mmHg
Technique:
- Instil topical anaesthetic (e.g. proxymetacaine 0.5%) + fluorescein
- Position patient at slit lamp, forehead against headrest
- Cobalt blue filter + maximal oblique illumination (~60°) directed at the prism
- Advance the prism until it just touches the corneal apex
- Two green semi-circular mires appear; rotate the force dial until their inner margins just align
- The dial reading × 10 gives IOP in mmHg
Sources of Error:
| Source | Effect on IOP Reading |
|---|---|
| Excessive fluorescein → thick mires | Overestimation |
| Insufficient fluorescein → thin mires | Underestimation |
| Thin cornea (CCT < 520 μm) | Underestimation |
| Thick cornea (CCT > 520 μm) | Overestimation |
| Post-refractive surgery (LASIK) | Underestimation |
| Corneal oedema | Artificial lowering |
| Astigmatism >3D | Distorted mires |
| Examiner finger pressure / lid squeezing | False high reading |
| Uncalibrated tonometer | False readings |
| Tight collar / breath-holding (↓ venous return) | Raised IOP |
Normal CCT assumed = 520 μm. Repeat readings over short intervals may give slightly falling values due to a corneal "massaging" effect.
Disinfection: 2% sodium hypochlorite (effective against adenovirus, HSV). 70% isopropyl alcohol does NOT protect against viral infection. Disposable prism caps are available.
2. Schiotz (Impression/Indentation) Tonometer
Principle: Measures the degree of corneal indentation produced by a plunger of known weight. Greater indentation = lower IOP; less indentation = higher IOP.
Instrument: A handheld device with a curved footplate that rests on the cornea, a central plunger, and a scale. Standard plunger weight = 5.5 g; heavier weights (7.5 g, 10 g) are added if reading is too high on the scale.
Technique:
- Patient lies supine, gazes at a fixed point on the ceiling
- Topical anaesthetic instilled
- Assemble with 5.5 g weight; test on convex metal calibration block (scale should read zero)
- Separate lids (using bony orbital rims only — no pressure on globe)
- Hold tonometer vertically; lower onto centre of cornea
- Read the scale; convert to mmHg using the Schiotz conversion table
Conversion Table (selected values):
| Scale Reading | 5.5 g weight (mmHg) | 7.5 g weight (mmHg) | 10 g weight (mmHg) |
|---|---|---|---|
| 2.5 | 27 | 39 | 55 |
| 4.0 | 21 | 30 | 43 |
| 5.0 | 17 | 26 | 37 |
| 7.5 | 12 | 19 | 28 |
Limitations: Seldom used today; less accurate than GAT due to effects of ocular rigidity; patient must be supine; requires skilled examiner.
3. Non-Contact Tonometer (Pneumotonometer / Air-Puff)
Principle: A jet of air flattens the central cornea. The time taken to sufficiently flatten the cornea is directly proportional to IOP. No contact is made with the eye.
Advantages:
- No topical anaesthesia required
- No risk of cross-infection
- Suitable for mass screening
- Quick and patient-friendly
Disadvantages:
- Less accurate; startling puff effect
- Accuracy improves with average of ≥3 readings
- Less reliable at very high or very low pressures
4. Palpation (Digital) Technique
Principle: The examiner presses on the sclera through the closed lids and compares the compliance of both eyes. An eye with acute angle-closure glaucoma feels rock-hard compared to the normal fellow eye.
Technique:
- Direct patient to look downward (without closing lids)
- Rest both hands on forehead; alternately indent each globe with an index finger
- An experienced clinician can estimate IOP within 3–5 mmHg
Limitation: Requires significant experience; not quantitative; only useful for detecting grossly elevated IOP.
5. Portable Applanation Tonometers
a) Perkins Tonometer:
- Uses a Goldmann prism + portable light source (hand-held)
- Applies the same Imbert-Fick principle as GAT
- Useful for bed-bound, anaesthetized, or uncooperative patients
- Requires topical anaesthesia and fluorescein
b) Tono-Pen (Electronic Applanation):
- Hand-held electronic contact tonometer (modified Mackay-Marg design)
- Probe tip contains a transducer that measures applied force
- Averages multiple readings; displays IOP + statistical confidence indicator
- Main advantage: measures IOP accurately in oedematous or distorted corneas, and through a soft contact lens
- Uses sterile disposable covers — suitable for use in infected eyes
c) iCare (Rebound Tonometer):
- Uses a 1.8 mm plastic ball on a magnetised wire
- Probe rebounds off the cornea; deceleration is proportional to IOP
- Anaesthesia not required
- Suitable for children, self-monitoring, and community screening
- Home version (iCare HOME2) used for diurnal IOP monitoring
- Probe must be at 90° to the frontal plane of the eye, 4–8 mm from the cornea
6. Dynamic Contour Tonometer (DCT) — e.g. PASCAL
Principle: Uses a solid-state pressure sensor with a corneal contour-matching concave surface. Measures IOP relatively independently of corneal mechanical factors (thickness, rigidity).
Advantages:
- Less influenced by CCT and previous refractive surgery
- Mounted on slit lamp like GAT
- More physiological measurement
7. Ocular Response Analyser (ORA)
- Air-puff technology records two applanation measurements: one during corneal inward movement and one during rebound
- Average = Goldmann-correlated IOP
- Difference between the two = Corneal Hysteresis (CH) — a measure of how corneal tissue absorbs and dissipates energy
- Low CH indicates higher risk of glaucoma progression
- Less influenced by previous laser refractive surgery
- Strongly correlates with magnitude of IOP reduction from prostaglandin therapy
Contraindications to Tonometry
| Contraindication | Reason |
|---|---|
| Suspected penetrating ocular injury | Risk of extrusion of intraocular contents |
| Active ocular/facial infection (herpetic/viral) | Risk of spreading infection |
| Corneal defect/abrasion | Additional trauma |
| Significant apprehension/blepharospasm/nystagmus | Inadequate examination; risk of corneal injury |
Relative contraindication: Infected eye — use non-contact tonometer or Tono-Pen with sterile cover; swab contact surfaces with alcohol and allow to dry.
Indications for Urgent Tonometry
- Acute angle-closure glaucoma — severe ocular/periorbital pain, smoky vision, cloudy cornea, mid-dilated fixed pupil, nausea/vomiting
- Iritis — risk of secondary angle-closure glaucoma or steroid-induced IOP rise
- Hyphema — blood in anterior chamber (e.g. post-trauma)
- Open-angle glaucoma screening — patients >40 years, family history, optic disc changes, visual field defects, or IOP ≥21 mmHg
Summary Comparison Table
| Tonometer | Principle | Anaesthesia | Contact | Best Use |
|---|---|---|---|---|
| Goldmann | Applanation (Imbert-Fick) | Yes | Yes | Gold standard, clinic |
| Schiotz | Impression/indentation | Yes | Yes | Portable, historical |
| Pneumotonometer | Air-puff applanation | No | No | Screening |
| Perkins | Applanation (Goldmann prism) | Yes | Yes | Bedside/anaesthetised |
| Tono-Pen | Electronic applanation | Yes | Yes | Oedematous corneas, contact lens wearers |
| iCare | Rebound | No | Brief | Children, self-monitoring |
| DCT (PASCAL) | Contour-matching sensor | Yes | Yes | CCT-independent measurement |
| ORA | Dual air-puff | No | No | Corneal hysteresis |
Sources: Kanski's Clinical Ophthalmology 10th ed.; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Guyton and Hall Medical Physiology; Pfenninger and Fowler's Procedures for Primary Care.
This is a shared conversation. Sign in to Orris to start your own chat.