U.t.i as per 2nf year mbbs pharma
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have all the material needed for a thorough 2nd year MBBS pharmacology answer on UTI. Here is the complete write-up:
Urinary Tract Infections (UTI) - Pharmacology (2nd Year MBBS)
1. Introduction & Common Pathogens
UTIs are among the most common bacterial infections worldwide, primarily affecting women and the elderly. The most frequent causative organisms are:
- E. coli (most common, ~80%)
- Klebsiella pneumoniae
- Staphylococcus saprophyticus (young sexually active women)
- Enterococcus faecalis
- Proteus mirabilis
- Pseudomonas aeruginosa (hospital-acquired, catheter-associated)
2. Classification of UTI
| Type | Location | Example |
|---|---|---|
| Lower UTI | Bladder/urethra | Cystitis, urethritis |
| Upper UTI | Kidney/ureters | Pyelonephritis |
| Uncomplicated | Healthy, non-pregnant women | Simple cystitis |
| Complicated | Men, pregnancy, catheters, obstruction | Recurrent/severe UTI |
3. Drugs Used in UTI
A. Urinary Tract Antiseptics/Antimicrobials (act primarily in urine)
These drugs achieve effective concentrations in the urine but NOT in systemic tissues - hence they are only used for lower UTI (cystitis), not pyelonephritis.
1. Nitrofurantoin
Mechanism of action:
Converted intracellularly by bacterial reductases to highly reactive intermediates that nonspecifically damage ribosomal proteins, and inhibit DNA, RNA, and protein synthesis. The mechanism is not fully understood - multiple bacterial targets are affected simultaneously, which is why resistance emerges very slowly.
Spectrum:
- Bactericidal against gram-negative (E. coli, Klebsiella) and gram-positive (Enterococcus, Staphylococcus) urinary pathogens
- Proteus spp. and Pseudomonas aeruginosa are intrinsically resistant
Pharmacokinetics:
- Well absorbed orally; rapidly metabolized and excreted
- Achieves urinary concentrations ~200 mcg/mL - no systemic antibacterial action
- Excreted via glomerular filtration AND tubular secretion
- Drug activity is enhanced at urine pH <5.5 (acidic urine)
- Formulations: macrocrystals (4x/day) vs macrocrystals + monohydrate combination (2x/day, Macrobid)
Dose: 100 mg orally 4 times/day (or 100 mg BD as long-acting preparation)
Adverse effects:
- Common: Anorexia, nausea, vomiting, diarrhea
- Serious (prolonged use >1 month): Pulmonary fibrosis, peripheral neuropathy, autoimmune hepatitis
- Hemolytic anemia in G6PD-deficient patients
- Hypersensitivity: rashes, pulmonary infiltrates
Contraindications:
- Significant renal insufficiency (CrCl <30-60 mL/min) - ineffective AND toxic
- Pyelonephritis or upper UTI (inadequate tissue levels)
- G6PD deficiency
Key exam point: Nitrofurantoin is currently first-line for uncomplicated cystitis (5-day course), especially as resistance to TMP-SMX and fluoroquinolones has increased.
2. Methenamine (Methenamine Mandelate / Methenamine Hippurate)
Mechanism of action:
Methenamine is a pro-drug. In acidic urine (pH ≤ 5.5), it hydrolyzes to release formaldehyde (HCHO) + ammonia. Formaldehyde is a non-specific bactericidal agent that denatures bacterial proteins and nucleic acids.
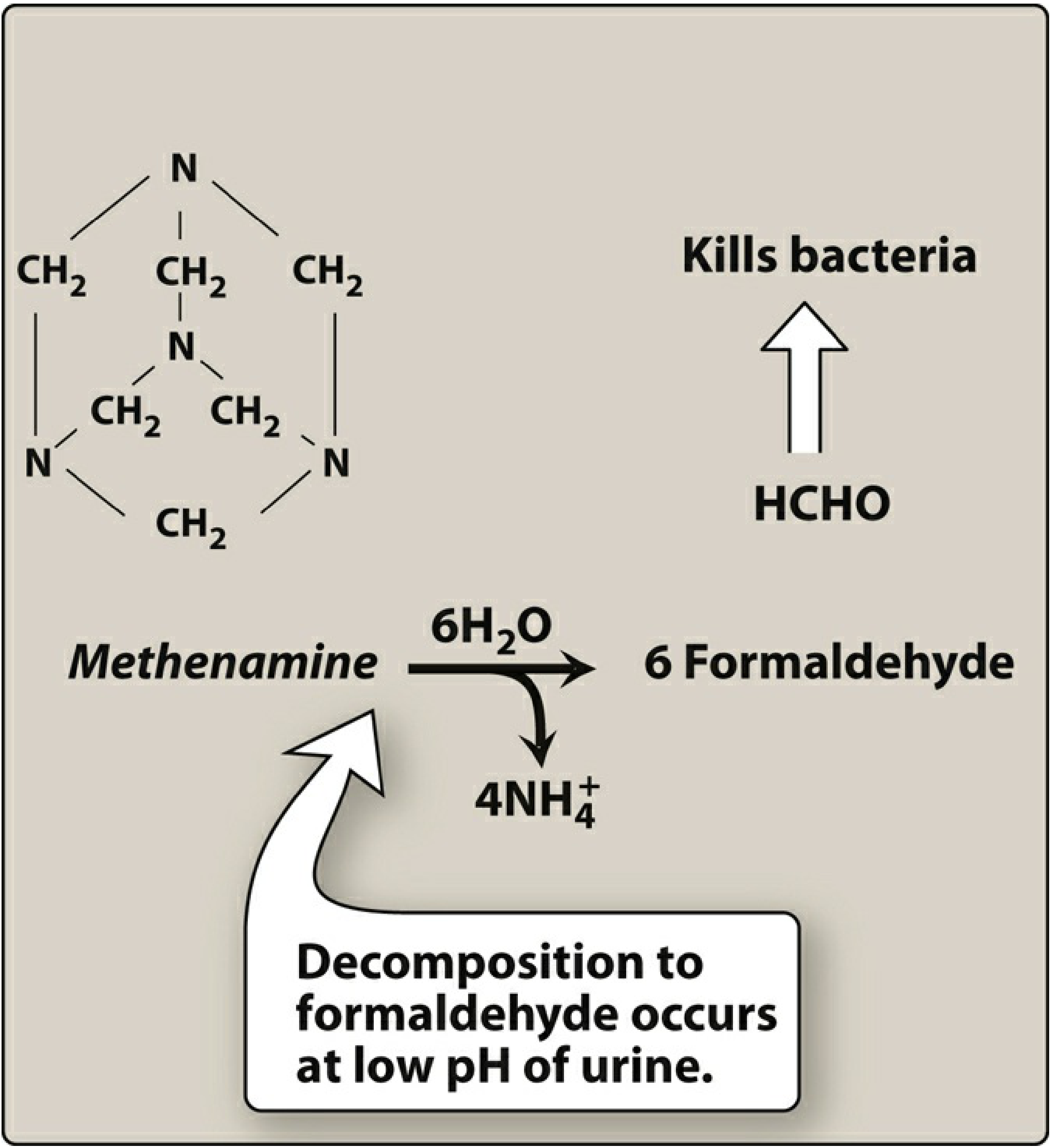
Methenamine decomposes to 6 formaldehyde molecules + 4 NH4+ at acidic urine pH - Lippincott Pharmacology
Formulations:
- Methenamine mandelate - combined with mandelic acid (keeps urine acidic)
- Methenamine hippurate - combined with hippuric acid (preferred in renal insufficiency as mandelic acid precipitates in renal failure)
Spectrum:
- Active against E. coli, Enterococcus, Staphylococcus
- Limited against Proteus - because Proteus produces urease, which alkalinizes urine, blocking formaldehyde release
- No resistance development (bacteria cannot develop resistance to formaldehyde)
Use: Chronic suppressive therapy to reduce frequency of recurrent UTIs. NOT used for acute treatment.
Adverse effects:
- GI distress (most common)
- High doses: albuminuria, hematuria, rash
Important drug interaction:
- Do NOT combine with sulfonamides (TMP-SMX) - increases crystalluria risk AND mutual antagonism
Contraindication: Renal insufficiency (with mandelate salt - mandelic acid precipitates)
3. Fosfomycin
Mechanism of action:
Inhibits enolpyruvyl transferase (MurA enzyme) - a key early step in peptidoglycan (bacterial cell wall) synthesis. Also reduces bacterial adherence to urinary epithelium.
Use: First-line for acute uncomplicated cystitis, given as a single oral dose (3g sachet). Particularly useful against multidrug-resistant E. coli and Enterococcus faecalis (including VRE).
Key exam point: Single-dose treatment = fosfomycin.
4. Systemic Antibiotics Used for UTI
These are used for both lower and upper UTI (pyelonephritis):
A. Trimethoprim-Sulfamethoxazole (Co-trimoxazole / TMP-SMX)
Mechanism - Sequential folate blockade (double blockade):
| Drug | Enzyme Inhibited | Step Blocked |
|---|---|---|
| Sulfamethoxazole (sulfonamide) | Dihydropteroate synthetase | Competes with PABA - blocks conversion of PABA → dihydrofolic acid |
| Trimethoprim | Dihydrofolate reductase (DHFR) | Blocks conversion of dihydrofolic acid → tetrahydrofolic acid |
This sequential blockade produces a synergistic bactericidal effect - bacteria cannot synthesize purines/thymidine and die.
Spectrum: Broad gram-negative coverage including E. coli, Klebsiella, Proteus, Enterobacteriaceae
Use: Uncomplicated cystitis (3-day course); avoid if local E. coli resistance >20%
Adverse effects:
- Nausea, vomiting, skin rash
- Hematologic toxicity (megaloblastic anemia - folate depletion)
- Hyperkalemia
- Crystalluria (with sulfonamide component)
- Stevens-Johnson syndrome (rare but serious)
- Teratogenic - avoid in 1st trimester and near term
B. Fluoroquinolones
Mechanism:
- Inhibit DNA gyrase (topoisomerase II) in gram-negative bacteria
- Inhibit topoisomerase IV in gram-positive bacteria
- Both are type II topoisomerases; inhibition prevents DNA supercoil relaxation, causing DNA strand breaks and cell death - bactericidal
Drugs used for UTI:
- Ciprofloxacin - best gram-negative coverage; used for complicated UTI and pyelonephritis
- Levofloxacin - broader spectrum, once daily
- Norfloxacin - primarily urinary concentrations only; for uncomplicated UTI (note: this is now largely replaced)
- Ofloxacin - urinary tract infections
Pharmacokinetics: High oral bioavailability, excellent tissue penetration, good urinary concentrations - can be used for upper UTI/pyelonephritis.
Adverse effects:
- Nausea, vomiting, photosensitivity
- QT prolongation (cardiac risk)
- Black box warnings: Tendinitis/tendon rupture, peripheral neuropathy, CNS effects (seizures, psychiatric)
- Avoid in children and pregnancy (cartilage damage in growing animals)
- Chelation with antacids, Ca2+, Mg2+, Fe2+ (reduce absorption)
Current status: Due to rising resistance and serious adverse effects, fluoroquinolones are now reserved for complicated UTI/pyelonephritis where alternatives are not suitable. They are NO longer preferred first-line for uncomplicated cystitis.
C. Beta-Lactams
Amoxicillin-Clavulanate:
- Active against E. coli producing beta-lactamase
- Used in pregnancy (safe)
Cephalosporins (e.g., Cephalexin, Cefixime):
- Used for uncomplicated UTI and during pregnancy
- Ceftriaxone IV for severe pyelonephritis
D. Aminoglycosides (Gentamicin, Amikacin)
- Reserved for severe/complicated UTI and hospital-acquired infections
- Gentamicin IV/IM for pyelonephritis
- Narrow therapeutic index - monitor renal function and drug levels
5. Treatment Summary (Current First-Line)
| Indication | Drug of Choice | Duration |
|---|---|---|
| Uncomplicated cystitis (women) | Nitrofurantoin | 5 days |
| Uncomplicated cystitis | Fosfomycin | Single dose |
| Uncomplicated cystitis | TMP-SMX (if resistance <20%) | 3 days |
| Pyelonephritis (mild-moderate) | Ciprofloxacin / Levofloxacin | 7-14 days |
| Pyelonephritis (severe) | IV Ceftriaxone / Aminoglycoside | 14 days |
| Pregnancy UTI | Cephalexin / Amoxicillin-Clav / Nitrofurantoin* | 7 days |
| Chronic suppression | Methenamine / Nitrofurantoin low dose | Long-term |
| Complicated/ESBL UTI | Fosfomycin / Meropenem | Per culture |
*Avoid nitrofurantoin near term (38-42 weeks) due to risk of neonatal hemolysis.
6. Key Pharmacology Points for Exam
- Nitrofurantoin - inhibits DNA/RNA synthesis; first-line for cystitis; NOT for pyelonephritis; causes pulmonary fibrosis with long use; contraindicated in renal failure
- Methenamine - prodrug; releases formaldehyde in acidic urine (pH <5.5); chronic suppression only; no resistance; avoid with sulfonamides
- Fosfomycin - inhibits MurA (cell wall); single dose; for uncomplicated cystitis
- TMP-SMX - double/sequential folate blockade (sulfonamide blocks DHPS; trimethoprim blocks DHFR); 3-day course; avoid in areas of >20% resistance
- Fluoroquinolones - inhibit DNA gyrase (GNB) and topoisomerase IV (GPB); now reserved for pyelonephritis; black box: tendon rupture
- Proteus raises urine pH - makes methenamine and nitrofurantoin less effective
- G6PD deficiency - avoid nitrofurantoin (hemolytic anemia)
- Single-dose = Fosfomycin; avoid single-dose nitrofurantoin and beta-lactams (high recurrence)
Sources: Katzung's Basic and Clinical Pharmacology 16th Ed; Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.