Urethritis
Reading File
Finding Sources
Searching PubMed
urethritis treatment guidelines
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Here is a thorough overview of urethritis drawn from multiple authoritative sources.
Urethritis
Definition
Urethritis is inflammation of the urethra, most commonly caused by sexually transmitted pathogens. Typical symptoms include urethral discharge, dysuria, urethral stinging or itching, and penile tip irritation, though many cases are entirely asymptomatic. There are an estimated 2.8 million cases annually in the United States.
Classification
Urethritis is divided into two major categories:
| Type | Cause | Key Features |
|---|---|---|
| Gonococcal Urethritis (GU) | Neisseria gonorrhoeae | ~5-20% of urethritis cases; profuse, purulent (white/yellow/green) discharge |
| Non-Gonococcal Urethritis (NGU) | C. trachomatis, M. genitalium, others | ~80-95% of urethritis cases; thin, clear or gray discharge |
Etiology of NGU
The causative organisms of NGU in order of frequency:
- Chlamydia trachomatis - 15-40% of NGU cases; most common in men under 24
- Mycoplasma genitalium - 15-25% of symptomatic NGU; 20-30% of persistent/recurrent cases
- Trichomonas vaginalis - prevalence varies widely by region (2-13%)
- Ureaplasma urealyticum - weak association, consider when no other pathogen identified
- HSV-1, HSV-2, adenovirus - less common causes
- Idiopathic - many men have no definitive pathogen identified
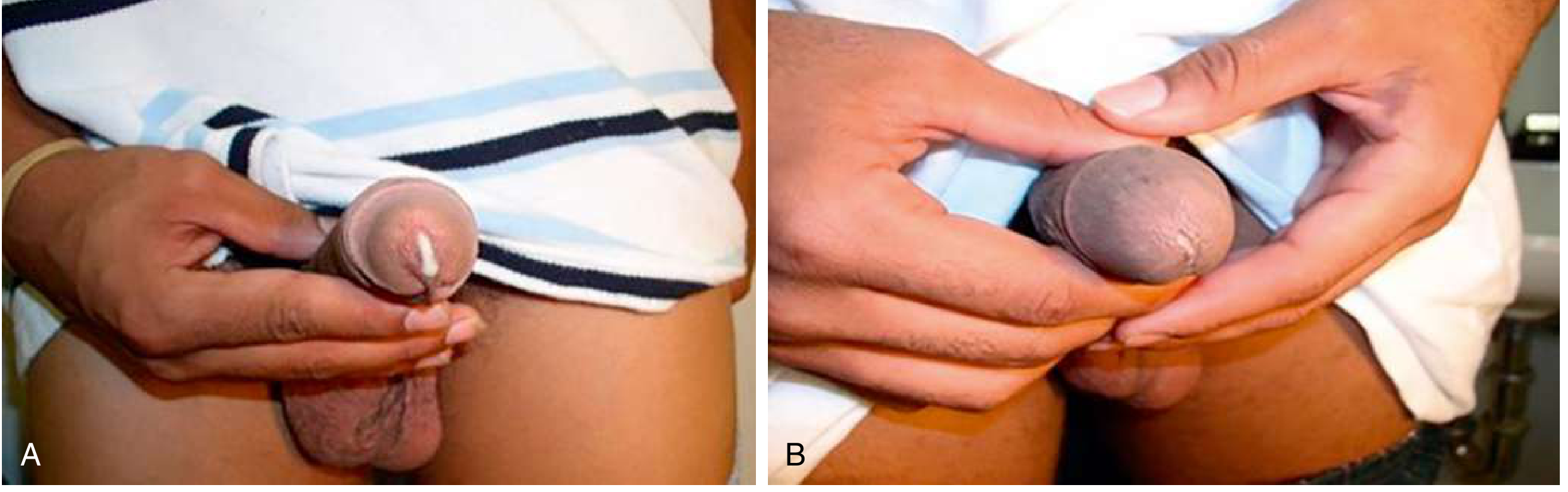
Clinical Features
Symptoms:
- Urethral discharge (purulent in GU, mucopurulent or clear in NGU)
- Dysuria
- Urethral burning, itching, or stinging
- Meatal irritation/erythema
- Often asymptomatic (especially in women and ~10% of men with GU)
Gonococcal urethritis: Incubation 2-6 days; profuse, purulent discharge; meatal erythema; penile lymphedema can occur.
Non-gonococcal urethritis: Symptoms generally less prominent; clinical features alone cannot reliably distinguish from GU - coinfection is common.
Diagnosis
Urethritis can be confirmed by any of the following:
- Mucoid, mucopurulent, or purulent discharge on examination
- Gram stain of urethral secretions showing ≥2 WBCs per oil immersion field (CDC updated threshold - previous threshold of ≥5 WBC/hpf missed significant chlamydia and gonorrhea cases)
- Positive leukocyte esterase on first-void urine
- >10 WBCs/hpf from first-void urine
Gram stain findings:
- Gram-negative intracellular diplococci = presumptive N. gonorrhoeae (diagnostic in symptomatic men; sensitivity limited, so negative result does not rule out)
- ≥2 WBCs with no intracellular diplococci = NGU
NAATs (Nucleic Acid Amplification Tests):
- Preferred method for detecting both N. gonorrhoeae and C. trachomatis (highest sensitivity)
- First-catch urine is the preferred specimen in males
- NAATs also available for T. vaginalis and M. genitalium (no FDA-approved M. genitalium NAAT yet)
- Note: NAATs are NOT FDA-cleared for rectal, oropharyngeal, or conjunctival gonorrhea - culture is preferred in those sites and in cases of sexual assault
When to culture: Suspected treatment failure, sexual assault in prepubescent patients, antimicrobial resistance surveillance.
Treatment
Gonococcal Urethritis
Current CDC-recommended regimen (note: resistance has driven regimen changes over the years):
- Ceftriaxone 500 mg IM single dose (1 g if weight ≥150 kg) - the mainstay
- If ceftriaxone unavailable: Cefixime 400 mg PO + Azithromycin 1 g PO (both in single doses)
- Cephalosporin allergy: Azithromycin 2 g PO once + gemifloxacin 320 mg PO OR gentamicin 240 mg IM
Important note: Treat for chlamydia co-infection empirically if not ruled out by NAAT.
Non-Gonococcal Urethritis
First-line (initial episode):
- Doxycycline 100 mg PO twice daily for 7 days (preferred per Rosen's EM; higher cure rates for M. genitalium)
- OR Azithromycin 1 g PO single dose (cure rates for M. genitalium have dropped from 85% to ~40% due to resistance)
Alternative regimens:
- Erythromycin base 500 mg PO QID x 7 days
- Levofloxacin 500 mg PO once daily x 7 days
- Ofloxacin 300 mg PO twice daily x 7 days
Treatment Algorithm for NGU
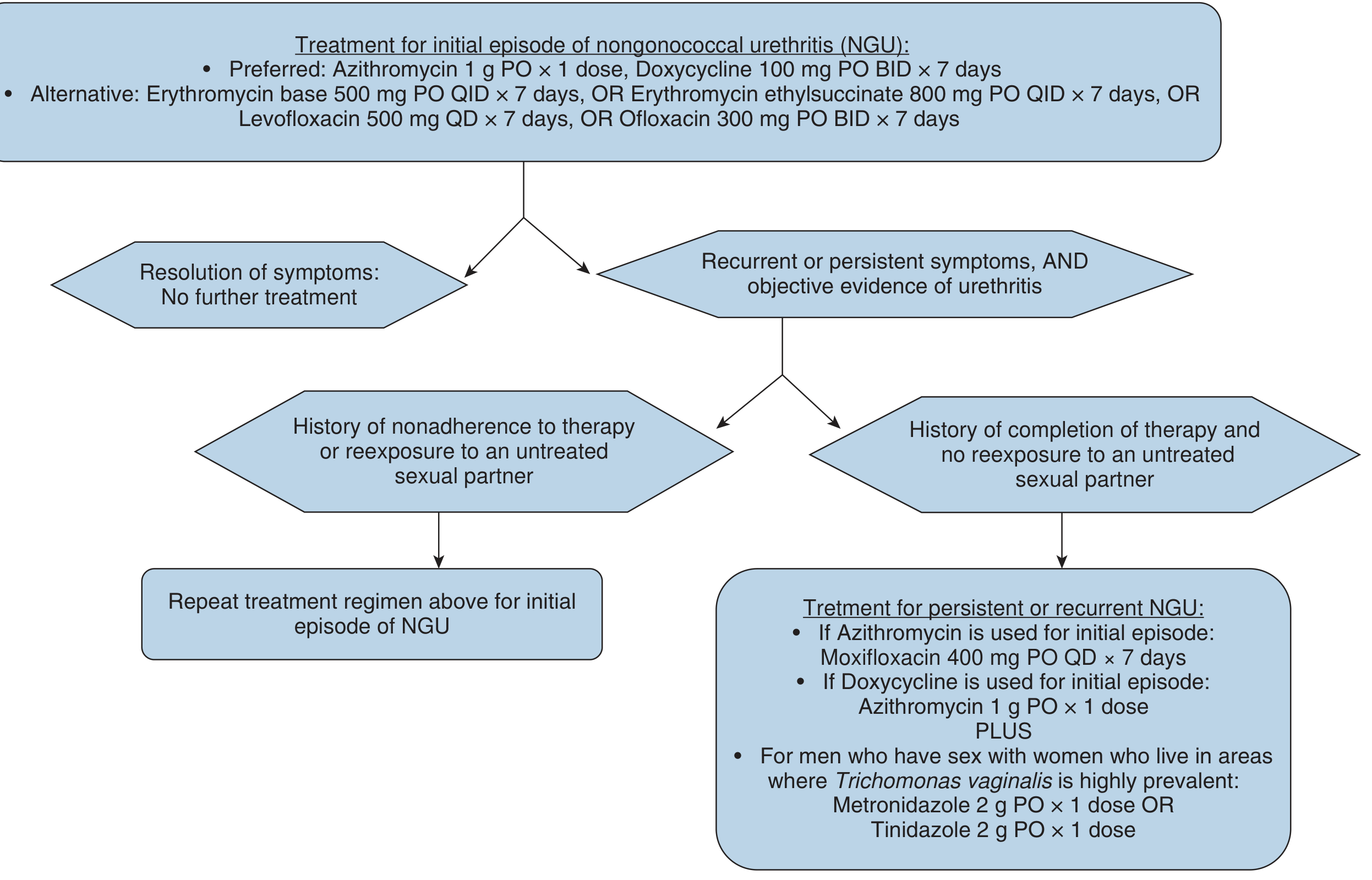
Persistent or Recurrent NGU
Consider resistant M. genitalium or T. vaginalis. Distinguish between:
- Non-adherence or re-exposure to untreated partner - Repeat the initial regimen
- Treatment failure despite completion and no re-exposure:
- If azithromycin was used initially: Moxifloxacin 400 mg PO daily x 7-14 days
- If doxycycline was used initially: Azithromycin 1 g PO x 1 dose
- In areas of high T. vaginalis prevalence: Add Metronidazole 2 g PO once OR Tinidazole 2 g PO once
Trichomoniasis (when T. vaginalis identified)
- Metronidazole 2 g PO once OR Tinidazole 2 g PO once
Complications
| Complication | Notes |
|---|---|
| Epididymitis | Most common; unilateral pain/swelling; treat with ceftriaxone 500 mg IM + doxycycline 100 mg BID x 10 days |
| Orchitis | Often accompanies epididymitis (epididymo-orchitis) |
| Prostatitis | |
| Proctitis | |
| Pelvic Inflammatory Disease (PID) | In women with ascending infection; risk of tubal scarring, infertility, ectopic pregnancy |
| Disseminated Gonococcal Infection (DGI) | Rare; treat with ceftriaxone 1 g IV/IM every 24 hours |
| Reiter Syndrome | Post-chlamydial reactive arthritis |
| Periurethral abscess / penile cellulitis | Usually responds to standard single-dose GU treatment |
Partner Management
- Partners with sexual contact within the preceding 60 days should be referred for evaluation, testing, and presumptive treatment
- Patients should abstain from intercourse for 7 days after single-dose treatment, or until completion of multi-day therapy with symptom resolution
- Screen concurrently for gonorrhea, chlamydia, syphilis, HIV (and trichomoniasis where appropriate)
- 3-month re-testing is recommended (not a test of cure at <3 weeks due to residual nucleic acids)
Special Considerations
Antimicrobial resistance: A major and growing challenge.
- N. gonorrhoeae has developed resistance to penicillin, tetracycline, fluoroquinolones, and azithromycin - ceftriaxone remains the mainstay
- M. genitalium is increasingly resistant to azithromycin; moxifloxacin is the rescue agent
- The CDC's Gonococcal Isolate Surveillance Project (GISP) monitors trends
Women: Often asymptomatic for both GU and NGU; may present with cervicitis or sequelae (PID). NAATs of first-void urine or self-collected vaginal swab are the standard.
HIV: HIV status does not change antibiotic regimens for urethritis.
Sources: Campbell-Walsh-Wein Urology; Goldman-Cecil Medicine; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine
Recent guideline note (2026): A 2026 German practice guideline (PMID 41779165) provides a practical update on urethritis management - the core treatment framework above remains consistent with current standards, though monitoring local resistance patterns for M. genitalium and N. gonorrhoeae is increasingly emphasized.
This is a shared conversation. Sign in to Orris to start your own chat.