BONE HEALING RELATIVE AND ABSOLUTE STABILITY
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bone healing" AND "relative stability" AND "absolute stability"
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material from the most authoritative orthopaedic textbooks. Let me compile the full detailed response.
Bone Healing: Relative and Absolute Stability
The mechanical environment at the fracture site is the single most important determinant of the type of bone healing that occurs. The two governing concepts are absolute stability and relative stability, each producing a fundamentally different biological response.
1. The Strain Concept - Foundation of Both Modes
Strain is the fundamental link between mechanical stability and healing biology.
Strain = Change in fracture gap / Original fracture gap (ΔL/L)
Strain at the fracture site determines which healing pathway is activated:
| Strain Level | Result |
|---|---|
| < 2% | Primary (direct) bone healing - intramembranous ossification |
| 2% - 10% | Secondary bone healing - endochondral ossification + callus |
| > 10% | No bone formation possible |
- Miller's Review of Orthopaedics, 9th Edition
A key insight: stability determines strain, and strain determines the type of healing.
2. Absolute Stability
Definition
Absolute stability means no motion at the fracture site under physiologic load. Strain is zero or near-zero.
Resulting Healing: Direct (Primary) Bone Healing
- Healing proceeds without callus formation
- Osteoclastic "cutting cones" cross the fracture gap directly, followed by osteoblast deposition of new osteons (Haversian remodeling)
- Bypasses the inflammatory/cartilaginous stages of normal healing
- Proceeds directly to the remodeling stage
- No visible periosteal callus on radiographs - makes confirmation of union difficult
"The process of direct bone healing does not require the intermediate steps of natural bone healing and proceeds directly to the remodeling stage. This does not increase the speed of healing - rather the process of direct bone healing is recognized as a much slower process." - Rockwood & Green's Fractures in Adults, 10th Ed. 2025
Two subtypes of direct healing:
- Contact healing - when cortical surfaces are in direct apposition (gap < 0.01 mm); osteonal remodeling crosses directly
- Gap healing - when a residual gap exists (up to ~1 mm); gap fills with woven bone first, then undergoes secondary Haversian remodeling
Implants that provide Absolute Stability:
- Lag screws (interfragmentary compression) - provide rigid compression; typically a neutralization plate is added to protect the lag
- Compression plating (using DCP/LCP in compression mode) - eccentric screw placement generates axial compression
- Neutralization plating + lag screw - neutralizes deforming forces while lag screw compresses fragments
"Compression plating is a technique that allows the surgeon to obtain absolute stability in the setting of a simple (most commonly transverse or short oblique) fracture pattern." - Rockwood & Green's, 10th Ed.
Indications:
- Intra-articular fractures - require anatomical reduction + absolute stability; callus at the fracture site would inhibit joint movement
- Simple (transverse or short oblique) diaphyseal fractures amenable to compression
- Surgically accessible fractures where direct reduction is achievable without major soft tissue stripping
Important Clinical Caveat:
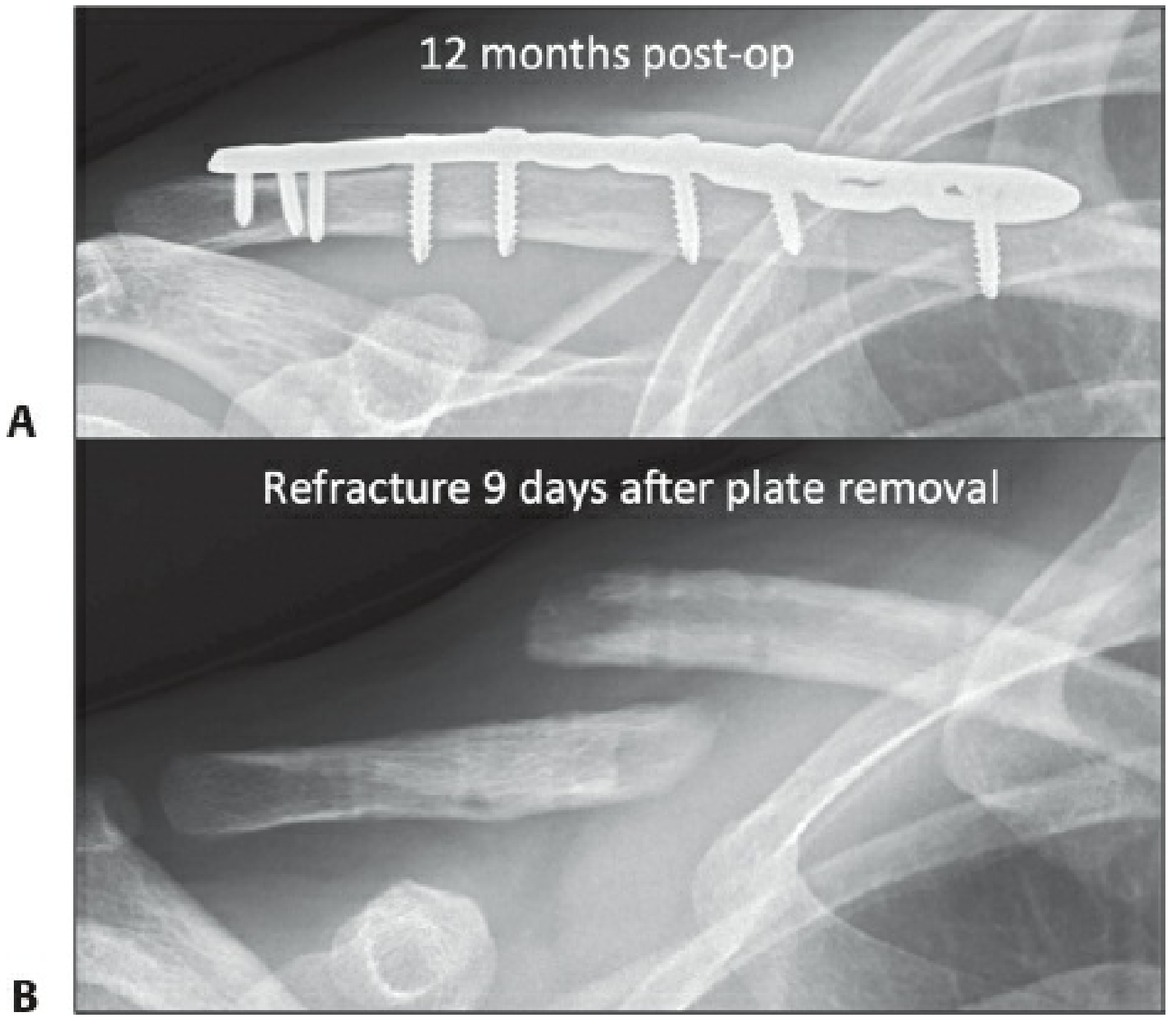
Absolute stability is technically demanding and difficult to fully achieve in practice. Modern clinical studies report callus in nearly all fractures fixed with compression techniques, emphasizing how hard true absolute stability is to obtain. Because direct bone healing is slow and produces no visible callus, early plate removal risks refracture - plate removal should be delayed up to 2 years.
3. Relative Stability
Definition
Relative stability allows controlled micromotion at the fracture site under physiologic load. This micromotion is the stimulus for callus formation.
Resulting Healing: Indirect (Secondary) Bone Healing
Secondary bone healing proceeds through the classic stages of endochondral ossification:
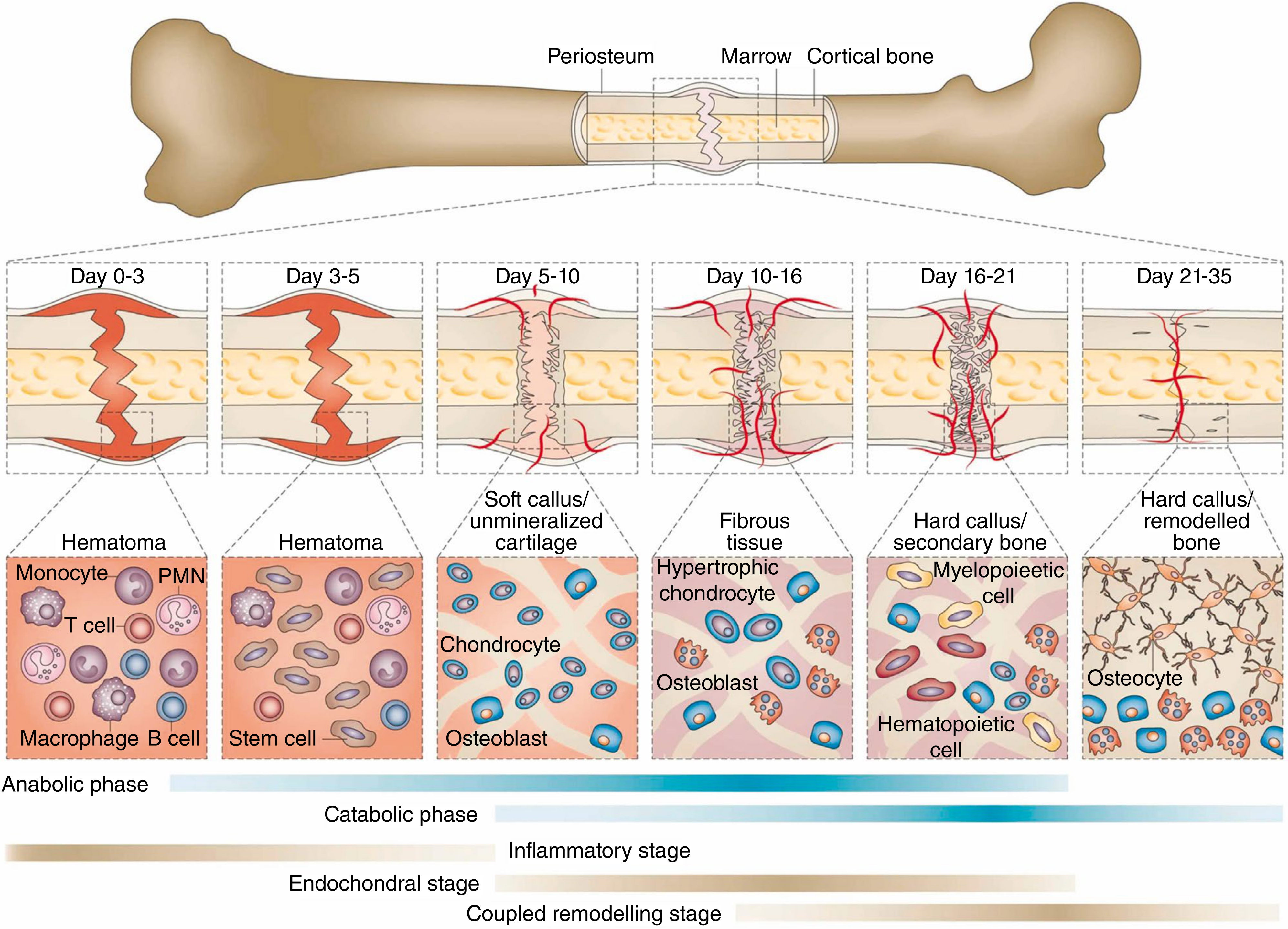
Stage 1 (Days 0-3): Fracture hematoma forms - inflammatory cells invade, lysosomal degradation of necrotic tissue begins
Stage 2 (Days 3-10): Pluripotential mesenchymal cells differentiate into fibroblasts, chondroblasts, and osteoblasts - soft cartilaginous callus forms; angiogenesis begins
Stage 3 (Days 10-21): Cartilaginous callus undergoes endochondral ossification - replaced by woven bone (hard callus)
Stage 4 (Days 21+, months to years): Woven bone replaced by lamellar bone; medullary canal restored; Wolff's Law remodeling
"Micromotion at the fracture site under physiologic load leads to callus formation. Strain decreases as callus matures, leading to increased stability." - Miller's Review of Orthopaedics, 9th Ed.
Self-reinforcing nature:
As callus matures and mineralizes, the effective fracture gap widens (bridges comminution), reducing strain over time. This progressive stiffening is the hallmark of successful secondary healing.
Implants that provide Relative Stability:
- Intramedullary (IM) nails - share load with the bone, allow elastic deformation; goal is always relative stability
- Bridge plates / locked plating - plate "bridges" area of comminution with fixation above and below; allows some elastic deformation
- External fixators
- Functional braces / casts
"IM nails are most frequently employed to stabilize fractures of the diaphyseal and metaphyseal regions. In all of these applications, the goal is relative stability and the maintenance of appropriate length, alignment, and rotation." - Rockwood & Green's, 10th Ed.
Indications:
- Comminuted/multifragmentary fractures where anatomic reduction of each fragment is not feasible
- Metaphyseal/diaphyseal fractures (non-articular)
- Fractures managed with biological (indirect) reduction techniques to preserve the fracture hematoma and periosteal blood supply
Pitfall - Too Much Motion:
If the fixation is too flexible and motion exceeds the tolerated strain threshold (> 10%), callus becomes hypertrophic as the bone attempts to distribute force over a larger area. This can result in hypertrophic nonunion - biologically active but mechanically unable to bridge.
4. Comparison Table
| Feature | Absolute Stability | Relative Stability |
|---|---|---|
| Motion at fracture | None | Controlled micromotion |
| Strain | ~0% | 2-10% |
| Healing type | Direct (primary) | Indirect (secondary) |
| Ossification | Intramembranous | Endochondral |
| Callus | None | Periosteal + bridging callus |
| Radiographic union | Slow/invisible | Visible callus progression |
| Healing speed | Slower | Faster |
| Implants | Lag screws, compression plates | IM nails, bridge plates, casts |
| Reduction required | Anatomical | Alignment (not necessarily anatomical) |
| Fracture hematoma | Typically removed | Preserved |
| Best for | Intra-articular, simple diaphyseal | Comminuted, metaphyseal/diaphyseal |
| Main risk | Slow healing, refracture if plate removed early | Hypertrophic nonunion if too much motion |
5. Surgical Decision-Making
The surgeon targets one mode deliberately based on fracture characteristics:
-
Absolute stability path: Obtain direct anatomic reduction (often requires hematoma removal) + interfragmentary compression. Chosen for intra-articular fractures and accessible simple fractures.
-
Relative stability path: Indirect reduction preserving the fracture hematoma and soft tissue envelope + bridge fixation. Chosen for comminuted patterns, periarticular metaphyseal fractures, and multiply injured patients.
"When planning to treat fracture surgically, the surgeon should target relative or absolute stability to induce endochondral or intramembranous ossification, respectively. Constructs that mix techniques of nonanatomic reduction and relative stability often lead to failure." - Rockwood & Green's Fractures in Adults, 10th Ed. 2025
A common error is mixing incompatible strategies - e.g., performing a non-anatomic (relative) reduction but then applying rigid fixation (absolute stability construct). The rigid construct eliminates the callus-promoting micromotion, yet the non-anatomic gap is too large for direct healing - resulting in failure.
6. Bone Type Considerations
Diaphyseal (cortical) bone:
- Decreased blood supply - longer healing
- Strain concentrated over smaller surface area
- More amenable to compression techniques in simple transverse/short oblique patterns
Metaphyseal (cancellous) bone:
- Larger surface area and better blood supply - heals faster
- Strain distributes over larger area - lower local strain
- However, joint surfaces tolerate very little malreduction (< 2 mm) - often requires longer NWB despite faster union
Sources:
- Rockwood & Green's Fractures in Adults, 10th Ed. 2025
- Miller's Review of Orthopaedics, 9th Ed.
- Campbell's Operative Orthopaedics, 15th Ed. 2026
- Bailey & Love's Short Practice of Surgery, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.