Analyse this report in English and give most possible diagnosis along with complications and benefits if present
python3 -c " import pdfplumber with pdfplumber.open('/home/daytona/workspace/attachments/0378c3cb-68d0-4b86-b97e-3cc1c466366e/v8_6kPm0C_289.pdf') as pdf: print(f'Pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() print(f'--- PAGE {i+1} ---') print(text) tables = page.extract_tables() if tables: print(f'TABLES on page {i+1}:') for j, table in enumerate(tables): print(f'Table {j+1}:') for row in table: print(row) "
polycythemia high RBC hematocrit hemoglobin thrombocytopenia causes differential diagnosis
Laboratory Report Analysis
Organized Findings: What's Abnormal
| Parameter | Result | Reference Range | Flag |
|---|---|---|---|
| RBC | 5.9 | 4.0–5.0 ×10¹²/L | ↑ HIGH |
| Hemoglobin (HGB) | 165 g/L | 130–160 g/L | ↑ HIGH |
| Hematocrit (HCT) | 53% | 40–48% | ↑ HIGH |
| Platelets (PLT) | 153 | 180–320 ×10⁹/L | ↓ LOW |
| Mean Platelet Volume (MPV) | 13 fL | 7.4–10.4 fL | ↑ HIGH |
| Large Platelets % | 47.8% | 11–45% | ↑ HIGH |
| Basophils % | 0% | 0.1–1% | ↓ LOW |
| Immature Granulocytes | 0.01 ×10⁹/L | 0 | Slightly raised |
Most Probable Diagnoses
1. Secondary Polycythemia (Erythrocytosis) - MOST LIKELY
- Dehydration / relative polycythemia - plasma volume contraction concentrates red cells without a true increase in mass. This is the simplest explanation and should be excluded first.
- High-altitude habitat or heavy smoking - both cause chronic hypoxia, raising EPO, and thus RBC production.
- Sleep apnea - an underdiagnosed cause of nocturnal hypoxia in young men.
- Anabolic steroid / testosterone use - common in young men and a well-known cause of erythrocytosis; erythropoietin stimulation via androgens.
- Chronic lung disease or carbon monoxide exposure (less likely given normal WBC/basophils and young age).
2. Polycythemia Vera (PV) - Less Likely but Must Be Excluded
3. Thrombocytopenia with Platelet Hyper-reactivity / Immune Thrombocytopenia (ITP) - Concurrent Finding
- PLT 153 ×10⁹/L (mild thrombocytopenia - below 180)
- MPV 13 fL - significantly elevated (normal 7.4–10.4)
- Large platelet % 47.8% - elevated
- Immune Thrombocytopenic Purpura (ITP) - autoimmune platelet destruction with compensatory megakaryocyte activation
- Early Bernard-Soulier syndrome (rare, hereditary, giant platelets)
- Peripheral destruction from other causes (hypersplenism if PV/splenomegaly is present)
4. Normal Variant / Athlete's Pseudopolycythemia
Diagnostic Flowchart (Harrison's 22E)
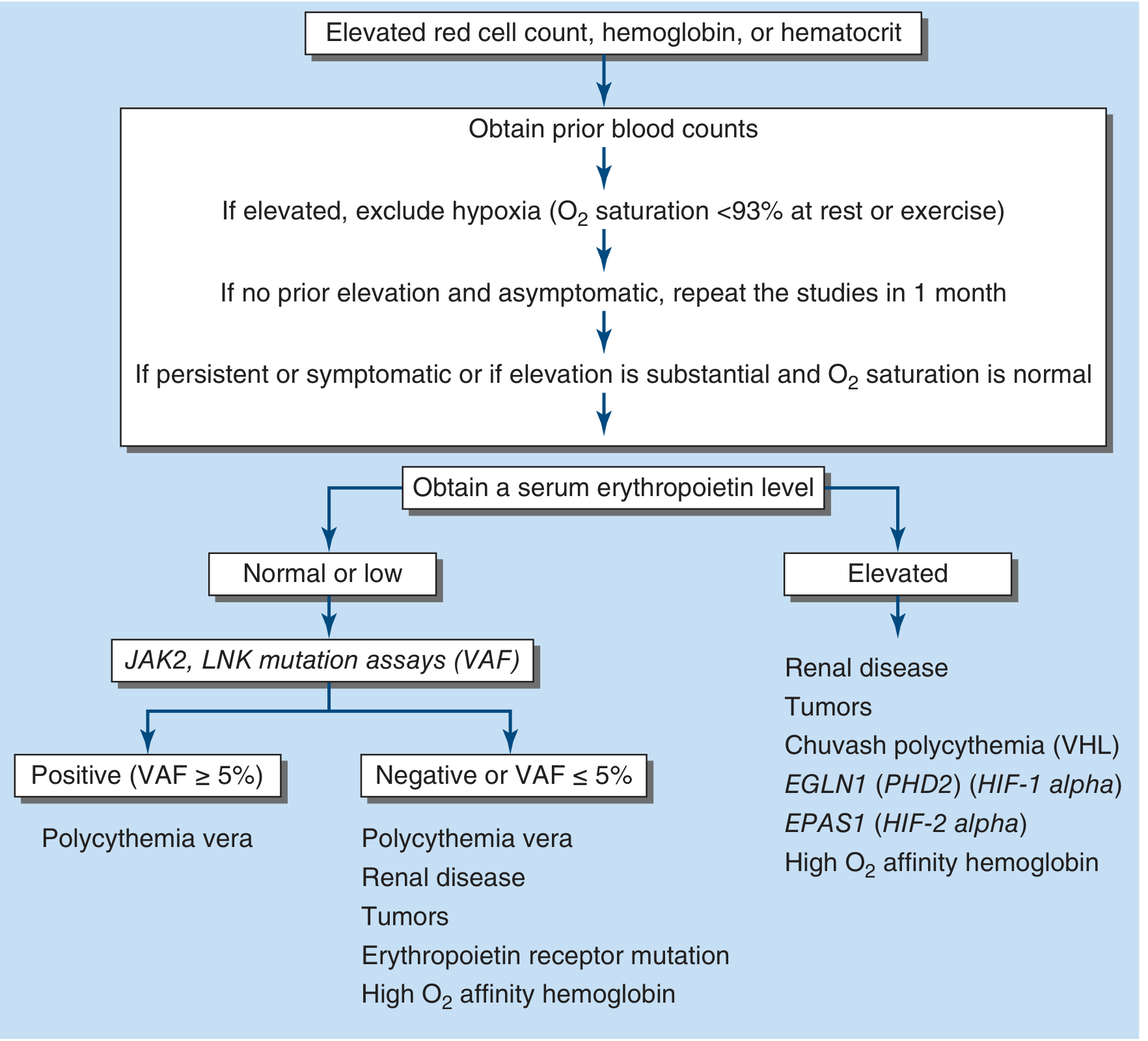
- Check O₂ saturation at rest and on exertion (exclude hypoxia)
- Obtain serum erythropoietin (EPO) level
- Low/normal EPO → order JAK2 V617F mutation assay → if positive: Polycythemia Vera
- Elevated EPO → look for secondary causes (renal disease, tumors, high altitude, anabolic steroids)
Potential Complications
From Polycythemia / High Hematocrit (HCT 53%):
- Hyperviscosity syndrome - blood viscosity increases logarithmically above HCT 55%; risk of thrombosis and microhemorrhage
- Venous thromboembolism (DVT, pulmonary embolism) - significantly increased risk
- Arterial thrombosis - stroke, transient ischemic attack, myocardial infarction
- Budd-Chiari syndrome / hepatic vein thrombosis (particularly in PV)
- Headache, tinnitus, vertigo, visual disturbances - from cerebral hyperviscosity
- Hypertension - common with elevated red cell mass
- Cor pulmonale - if underlying hypoxemia drives the polycythemia
- Progression to myelofibrosis or AML - if PV is the underlying cause
From Thrombocytopenia (PLT 153) with High MPV:
- Bleeding risk - especially if PLT drops further; epistaxis, mucosal bleeding, easy bruising
- Paradoxical thrombosis - large hyper-reactive platelets despite low count can still form clots
- Risk of severe bleeding with PLT <50 if not monitored
Notable "Benefit" / Protective Findings
- Normal TSH (2.686 mU/L) - thyroid function is completely normal; hypothyroidism (which can cause anemia/fatigue) and hyperthyroidism (which can cause erythrocytosis) are both excluded.
- Normal WBC and differential - no evidence of infection, leukemia, or immune activation at this time.
- Normal ESR (1 mm/hr) - confirms absence of significant systemic inflammation, autoimmune disease, or malignancy-related acute phase response.
- Normal MCV (89.8 fL), MCH, MCHC - red cells are normocytic and normochromic; iron deficiency and B12/folate deficiency are not masking or contributing.
- No nucleated red cells (NRBC = 0) - no bone marrow stress response or hemolytic crisis.
- Normal lymphocytes and monocytes - no lymphoma pattern, no monocytosis suggesting chronic myelomonocytic leukemia.
Recommended Next Steps
| Test | Purpose |
|---|---|
| Serum EPO level | Key branch point: low = primary (PV), high = secondary |
| JAK2 V617F mutation | Confirm/exclude PV if EPO is low/normal |
| Pulse oximetry (rest + exertion) | Exclude hypoxia as secondary cause |
| Serum ferritin + iron studies | Exclude iron deficiency (can mask polycythemia severity) |
| Renal ultrasound + creatinine | Exclude renal cause of excess EPO |
| Repeat CBC in 4–6 weeks | Confirm persistence and trend |
| Peripheral blood smear | Assess platelet morphology (giant platelets → Bernard-Soulier?) |
| Anti-platelet antibodies (PAIgG) | If ITP suspected |
Disclaimer: This interpretation is for educational purposes. As stated on the report itself, only the treating physician can establish a formal diagnosis using the full clinical picture.
- Harrison's Principles of Internal Medicine 22E, Chapter 56 (Polycythemia)
- Tintinalli's Emergency Medicine, Chapter 231 (Polycythemia)
- Robbins & Kumar Basic Pathology (Polycythemia classification)
- The Washington Manual of Medical Therapeutics (PV diagnostic criteria)



Analyse these also
elevated reticulocyte count 1.74% thrombocytopenia high RDW-SD causes diagnosis young male
Combined Report Analysis - Patient: Lakshay, 24 Years / Male
All Three Reports - Data Extraction
Report 1: Complete Blood Count (CBC)
| Parameter | Result | Reference Range | Flag |
|---|---|---|---|
| Haemoglobin (Hb) | 16.3 g/dL | 13–17 g/dL | Normal |
| Total Leukocyte Count (TLC) | 8.80 ×10⁹/L | 4–10 ×10⁹/L | Normal |
| Polymorphs (Neutrophils%) | 56.9% | 40–80% | Normal |
| Lymphocytes% | 35.4% | 20–40% | Normal |
| Monocytes% | 6.9% | 2–10% | Normal |
| Eosinophils% | 0.6% | 1–6% | ↓ Low |
| Basophils% | 0.2% | 1–2% | ↓ Low |
| Abs. Neutrophil Count | 5.01 ×10⁹/L | 2–7 ×10⁹/L | Normal |
| Abs. Lymphocyte Count | 3.11 ×10⁹/L | 1–3 ×10⁹/L | ↑ High |
| Abs. Monocyte Count | 0.61 ×10⁹/L | 0.2–1 ×10⁹/L | Normal |
| Platelet Count | 125 ×10⁹/L | 200–550 ×10⁹/L | ↓ LOW |
| RBC Count | 5.45 ×10¹²/L | 4.5–5.5 ×10¹²/L | Upper normal |
| PCV (Hematocrit) | 50.1% | 40–50% | ↑ Borderline High |
| MCV | 92.0 fL | 83–101 fL | Normal |
| MCH | 30.0 pg | 27–32 pg | Normal |
| MCHC | 32.5 g/dL | 31.5–34.5 g/dL | Normal |
| RDW-CV | 14.1% | 11.6–14% | ↑ Borderline High |
Report 2 (Page 2 of CBC):
| Parameter | Result | Reference Range | Flag |
|---|---|---|---|
| RDW-SD | 47.4 fL | 39–46 fL | ↑ HIGH |
Report 3: Reticulocyte Count
| Parameter | Result | Reference Range | Flag |
|---|---|---|---|
| Reticulocyte Count | 1.74% | 0.5–1.5% | ↑ HIGH |
Report 4: Lipid Profile
| Parameter | Result | Reference Range | Flag |
|---|---|---|---|
| Serum Triglycerides | 188 mg/dL | 60–160 mg/dL | ↑ HIGH |
| Serum Cholesterol | 191 mg/dL | 130–230 mg/dL | Normal |
| HDL | 47 mg/dL | 30–60 mg/dL | Normal |
| LDL | 104 mg/dL | 0–160 mg/dL | Normal |
| VLDL | 37 mg/dL | 16–32 mg/dL | ↑ HIGH |
Key Abnormalities - Summary
- PLT 125 ×10⁹/L - moderately low (reference: 200-550)
- Reticulocyte count 1.74% - elevated (reference: 0.5-1.5%)
- RDW-SD 47.4 fL - elevated (reference: 39-46 fL)
- RDW-CV 14.1% - borderline high
- Absolute lymphocytosis (3.11, upper limit 3.0) - mild
- PCV 50.1% - borderline elevated
- Triglycerides 188 mg/dL - elevated
- VLDL 37 mg/dL - elevated
- Eosinophils 0.6% and Basophils 0.2% - both low
Diagnostic Interpretation
The Most Critical Pattern: Elevated Reticulocyte Count + Thrombocytopenia + Elevated RDW
Most Probable Diagnoses
1. Immune Thrombocytopenic Purpura (ITP) - HIGHEST PROBABILITY
- PLT isolated at 125 (moderate thrombocytopenia)
- Normal WBC and differential
- Normal Hb - no anemia to suggest bone marrow failure
- Young male (though classic chronic ITP is more common in women; in young males it tends to be acute/post-viral)
2. Hemolytic Anemia (Compensated) with Concurrent Thrombocytopenia
- Hereditary spherocytosis - autosomal dominant, mild hemolysis, usually detected in young adults during stress
- G6PD deficiency - common in Indian males; episodic hemolysis triggered by oxidative stress, drugs, infections
- Autoimmune hemolytic anemia (AIHA) - warm antibody type; can co-exist with ITP as Evans syndrome
3. Evans Syndrome (ITP + AIHA Combined) - Important to Exclude
4. Secondary Polycythemia / High-Normal Erythrocytosis
5. Mixed Nutritional Deficiency (Iron + B12/Folate) Causing Dimorphic Anemia
6. Familial / Primary Hypertriglyceridemia (Type IV Dyslipidemia) - Fredrickson Type IV
- Primary/familial hypertriglyceridemia (genetic predisposition)
- Secondary hypertriglyceridemia from insulin resistance, sedentary lifestyle, high-carbohydrate/alcohol diet, or undiagnosed prediabetes
Complications
From Thrombocytopenia (PLT 125):
- Mucocutaneous bleeding - petechiae (pinpoint skin bleeds, especially dependent areas), purpura, ecchymoses
- Gingival bleeding and epistaxis - common early symptoms of ITP
- Menorrhagia (not applicable here - male patient)
- Serious bleeding risk if PLT falls below 50: GI bleeding, hematuria
- Life-threatening CNS hemorrhage (rare, if PLT drops severely below 20-30 ×10⁹/L)
- Per Robbins: "Subarachnoid hemorrhage and intracerebral hemorrhage are serious and sometimes fatal complications, but fortunately rare in treated patients."
From Hemolytic Anemia (if confirmed):
- Worsening anemia if bone marrow compensation fails
- Aplastic crisis (if parvovirus B19 infection occurs in a patient with ongoing hemolysis)
- Pigment gallstones (from chronic elevated bilirubin)
- Iron overload with chronic transfusion requirement
- Fatigue, jaundice, splenomegaly with progressive course
From Hypertriglyceridemia (TG 188 mg/dL):
- Acute pancreatitis - major risk when TG exceeds 500 mg/dL; currently at 188 mg/dL, the risk is emerging but not yet critical
- Accelerated atherosclerosis - premature cardiovascular disease in young adults with persistent hypertriglyceridemia + insulin resistance
- Fatty liver disease (NAFLD/MASLD) - high VLDL driving hepatic fat deposition
- Future progression to metabolic syndrome if diet and lifestyle are not modified
- Pancreatitis risk rises substantially if untreated and TG crosses 500 mg/dL
Protective / Reassuring Findings
- Hb 16.3 g/dL - completely normal - even if hemolysis is occurring, the bone marrow is fully compensating; no clinical anemia at this point
- Normal WBC (8.80) - no leukopenia, leukocytosis, or left shift to suggest bone marrow failure, leukemia, or active infection
- Normal MCV (92 fL) and MCH - macrocytes are not predominating; B12 deficiency is not a dominant feature
- Total cholesterol 191 mg/dL - normal - overall cardiovascular risk from the lipid profile is moderate, not severe
- LDL 104 mg/dL - normal - the most atherogenic fraction is well-controlled
- Normal absolute neutrophil count (5.01) - immune function is intact
- PCV 50.1% - borderline but not in polycythemia range - oxygen-carrying capacity is good
Recommended Next Steps
| Test | Reason |
|---|---|
| Peripheral blood smear | Look for large platelets, spherocytes, fragmented RBCs (schistocytes), polychromasia |
| Direct Antiglobulin Test (DAT/Coombs) | Confirm or exclude AIHA; if positive alongside thrombocytopenia = Evans syndrome |
| Serum LDH + indirect bilirubin + haptoglobin | Confirm hemolysis (LDH↑, bilirubin↑, haptoglobin↓ in hemolysis) |
| Serum ferritin + iron studies | Exclude iron deficiency contributing to RDW elevation |
| Serum B12 + folate | Exclude megaloblastic component |
| Bone marrow aspiration (if diagnosis unclear) | Rule out marrow failure; ITP shows normal/increased megakaryocytes |
| Platelet antibody testing (anti-GPIIb/IIIa) | Supports ITP diagnosis (low sensitivity but specific if positive) |
| Fasting glucose + HbA1c | Screen for prediabetes/insulin resistance driving hypertriglyceridemia |
| Repeat lipid profile (fasting state) | Confirm triglyceride elevation in true fasting state |
| G6PD enzyme assay | Especially relevant in young Indian males with hemolytic pattern |
Overall Clinical Picture
- ITP (primary immune thrombocytopenic purpura) - isolated PLT 125 with compensated hematopoiesis
- Compensated hemolytic anemia (etiology to be determined - G6PD, hereditary spherocytosis, AIHA) - explaining the elevated reticulocytes and RDW
- The combination of both raises the suspicion of Evans syndrome (autoimmune destruction of both platelets and RBCs)
- Familial/secondary hypertriglyceridemia (Fredrickson Type IV) as an independent metabolic finding requiring lifestyle intervention and monitoring
This analysis is for educational and interpretive purposes. Formal diagnosis must be established by the treating clinician, Dr. Sudhir Attri, using the full clinical history, physical examination, and follow-up investigations.
Include results from this also
python3 -c " import pdfplumber with pdfplumber.open('/home/daytona/workspace/attachments/0378c3cb-68d0-4b86-b97e-3cc1c466366e/6619082500003-2.pdf') as pdf: print(f'Pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() print(f'--- PAGE {i+1} ---') print(text) "
elevated ALT 104 GGT 108 ALP 121 young male causes NAFLD alcoholic liver disease interpretation
Updated Integrated Analysis - All Reports Combined
New Report Data - Max Lab (01 Aug 2025)
HbA1c
| Parameter | Result | Reference | Flag |
|---|---|---|---|
| HbA1c (NGSP%) | 4.60% | <5.7% | ✅ Normal (Non-Diabetic) |
| Average Glucose (last 3 months) | 85.32 mg/dL | - | ✅ Excellent |
Liver Function Test (LFT)
| Parameter | Result | Reference | Flag |
|---|---|---|---|
| Total Protein | 8.22 g/dL | 6.6–8.3 | Normal |
| Albumin | 5.0 g/dL | 3.5–5.2 | Normal |
| Globulin | 3.2 g/dL | 2.3–5.0 | Normal |
| A:G Ratio | 1.6 | 1.2–1.5 | ↑ Slightly high |
| Total Bilirubin | 0.41 mg/dL | 0.3–1.2 | Normal |
| Direct Bilirubin | 0.12 mg/dL | 0.0–0.2 | Normal |
| Indirect Bilirubin | 0.29 mg/dL | 0.1–1.0 | Normal |
| SGOT / AST | 45.7 U/L | <50 | Normal (borderline) |
| SGPT / ALT | 104 U/L | <50 | ↑↑ HIGH (2× ULN) |
| ALP | 121 U/L | 30–120 | ↑ Borderline High |
| GGT (GGTP) | 108.2 U/L | 7–50 | ↑↑ HIGH (>2× ULN) |
CBC (Max Lab)
| Parameter | Result | Reference | Flag |
|---|---|---|---|
| Haemoglobin | 17.1 g/dL | 13–17 | ↑ Slightly above |
| PCV | 49.5% | 40–50 | Normal (upper limit) |
| TLC | 9.6 ×10⁹/L | 4–10 | Normal |
| RBC | 5.57 ×10¹²/L | 4.5–5.5 | ↑ Slightly above |
| MCV | 89.0 fL | 83–101 | Normal |
| MCH | 30.7 pg | 27–32 | Normal |
| MCHC | 34.5 g/dL | 31.5–34.5 | Normal (upper limit) |
| Platelet Count | 162 ×10⁹/L | 150–410 | Low-normal (earlier was 125) |
| MPV | 12.4 fL | 7.8–11.2 | ↑ HIGH |
| RDW | 14.5% | 11.5–14.5 | Normal (upper limit) |
| Eosinophils% | 0.6% | 1–6 | ↓ Low |
Thyroid Profile (Total T3, T4, TSH)
| Parameter | Result | Reference | Flag |
|---|---|---|---|
| T3 (Total) | 1.20 ng/mL | 0.87–1.78 | ✅ Normal |
| T4 (Total) | 6.50 µg/dL | 5.93–13.29 | ✅ Normal |
| TSH | 5.74 uIU/mL | 0.34–5.6 | ↑ ELEVATED |
Anti-TPO Antibody
| Parameter | Result | Reference | Flag |
|---|---|---|---|
| Anti-TPO | 15.20 IU/mL | 1–16 | Normal (upper limit) |
Timeline of Key Parameters Across All Reports
| Parameter | Max Lab (01 Aug) | PGIMS (07-08 Aug) |
|---|---|---|
| Hemoglobin | 17.1 g/dL ↑ | 16.3 g/dL (normal) |
| PCV/HCT | 49.5% | 50.1% ↑ |
| RBC | 5.57 ↑ | 5.45 |
| Platelets | 162 | 125 ↓ |
| MPV | 12.4 fL ↑ | (not separately listed) |
| Reticulocytes | not tested | 1.74% ↑ |
| RDW | 14.5% | 47.4 fL (SD) ↑ |
| TSH | 5.74 ↑ | not tested |
Integrated Diagnostic Picture
THE DOMINANT FINDING: Hepatocellular Pattern Liver Injury
Most Probable Diagnoses - Updated and Refined
1. Non-Alcoholic Fatty Liver Disease / Metabolic-Associated Steatotic Liver Disease (NAFLD/MASLD) - MOST LIKELY
- ALT 104 + GGT 108 = hepatocellular pattern liver injury (AST:ALT <1 = non-alcoholic)
- Elevated triglycerides (188 mg/dL) + elevated VLDL (37) = underlying dyslipidemia driving hepatic fat deposition
- Normal HbA1c (4.60%) = diabetes is excluded, but this does NOT exclude early insulin resistance or metabolic syndrome
- Slightly elevated Hb + PCV in a young, likely well-nourished male supports a picture of caloric excess
- NAFLD is now the most common liver disease globally in young adults, strongly associated with hypertriglyceridemia and central obesity even without frank diabetes
2. Subclinical Hypothyroidism - CONFIRMED
- Hypertriglyceridemia - thyroid hormones regulate hepatic lipid metabolism; even mild hypothyroidism raises triglycerides and VLDL
- Elevated liver enzymes - hypothyroidism can cause hepatic steatosis and mild transaminase elevation
- Thrombocytopenia - there is an established association between autoimmune thyroid disease and immune thrombocytopenia (ITP)
- Relative erythrocytosis in some cases
3. Immune Thrombocytopenic Purpura (ITP) - Associated with Autoimmune State
4. Compensated Hemolytic Anemia / Increased Red Cell Turnover
5. Possible Early Hashimoto's Thyroiditis
Complications - Updated Comprehensive List
From Subclinical Hypothyroidism / Early Hashimoto's:
- Progression to overt hypothyroidism - fatigue, weight gain, cold intolerance, bradycardia, constipation, depression
- Worsening dyslipidemia - further rise in triglycerides and LDL if hypothyroidism progresses
- Cardiovascular disease risk - accelerated atherosclerosis from combined hypothyroidism + hypertriglyceridemia
- Goiter formation - as the thyroid works harder against immune attack
- Associated autoimmune conditions - type 1 diabetes, pernicious anemia, celiac disease, Addison's disease (polyglandular autoimmune syndrome)
- Perpetuation of ITP - shared autoimmune mechanism
From Liver Disease (NAFLD/MASLD):
- Progression to NASH (Non-Alcoholic Steatohepatitis) - with ongoing inflammation causing fibrosis
- Liver fibrosis → cirrhosis - if metabolic triggers (hypertriglyceridemia, insulin resistance) are not addressed
- Hepatocellular carcinoma (HCC) - risk in cirrhotic NAFLD, though this is a distant concern at age 24
- Portal hypertension with varices in advanced disease
- The GGT elevation is particularly concerning as a predictor of future metabolic risk - elevated GGT is associated with increased cardiovascular events, insulin resistance, and liver fibrosis progression
From Hypertriglyceridemia:
- Acute pancreatitis (risk rises sharply if TG exceeds 500 mg/dL; currently 188)
- Accelerated atherosclerosis - VLDL is atherogenic
- Worsening NAFLD - hepatic fat driven by excess VLDL/triglyceride flux
From Thrombocytopenia (PLT 125, trending down from 162):
- Petechiae, purpura, easy bruising - mucocutaneous bleeding
- Risk of serious bleeding if count drops further (<50)
- Intracranial hemorrhage if PLT drops severely
Protective / Reassuring Findings
- HbA1c 4.60% - excellent glycemic control; diabetes is definitively excluded. The average glucose of 85.32 mg/dL is optimal, meaning insulin resistance, while possible, has not yet affected glucose metabolism
- Bilirubin completely normal (0.41 mg/dL) - liver synthetic function is intact; no jaundice; significant hemolysis is less likely
- Albumin 5.0 g/dL - excellent liver synthetic function; no hypoalbuminemia which would indicate cirrhosis or severe liver disease
- Normal T3 and T4 - despite elevated TSH, thyroid hormone levels are still adequate; overt hypothyroidism is not yet present
- Anti-TPO within normal range (15.2, ref <16) - borderline but not overtly positive; autoimmune thyroid disease is early and may not progress
- Normal total cholesterol (191) and LDL (104) - the most dangerous lipid fraction is controlled; overall CVD risk is moderate
- Normal AST (45.7) - the AST:ALT ratio of 0.44 rules out alcohol-related liver disease and cirrhosis (which would show AST > ALT)
- Normal bilirubin with normal albumin - the liver is not failing despite the enzyme elevations; this is a hepatocellular injury pattern, not liver failure
Recommended Next Steps - Final Updated List
| Test | Priority | Reason |
|---|---|---|
| Repeat TSH + Free T4 (fasting, morning) | HIGH | Confirm subclinical hypothyroidism; morning specimen required for accurate TSH |
| Anti-TPO repeat in 3 months | HIGH | Confirm/exclude early Hashimoto's; borderline result needs trend |
| Ultrasound abdomen (liver) | HIGH | Assess for hepatic steatosis (NAFLD), liver size, spleen size |
| Hepatitis B surface antigen (HBsAg) + Anti-HCV | HIGH | Exclude viral hepatitis as cause of elevated ALT/GGT |
| Fasting insulin + HOMA-IR | HIGH | Detect insulin resistance even with normal HbA1c (early metabolic syndrome) |
| Repeat platelet count weekly | HIGH | Trend is falling (162→125); needs close monitoring |
| Peripheral blood smear | HIGH | Look for large platelets, spherocytes, schistocytes |
| DAT (Direct Coombs Test) | MEDIUM | Confirm/exclude AIHA; together with ITP = Evans syndrome |
| Serum ferritin + iron studies | MEDIUM | Assess iron stores; elevated ferritin can indicate NAFLD |
| Serum LDH + haptoglobin | MEDIUM | Confirm or exclude hemolysis |
| G6PD assay | MEDIUM | Young Indian male with elevated reticulocytes |
| FibroScan or liver biopsy (if ultrasound abnormal) | LOW (later) | Grade severity of liver fibrosis if NAFLD confirmed |
| Anti-nuclear antibody (ANA) | MEDIUM | Screen for broader autoimmune disease given thyroid autoimmunity + ITP pattern |
Final Summary
| System | Finding | Most Probable Cause |
|---|---|---|
| Liver | ALT 104, GGT 108, ALP 121↑ (AST:ALT 0.44) | NAFLD / early NASH |
| Thyroid | TSH 5.74 ↑, T3/T4 normal, Anti-TPO borderline | Subclinical hypothyroidism (early Hashimoto's) |
| Lipids | Triglycerides 188 ↑, VLDL 37 ↑ | Hypertriglyceridemia (driven by hypothyroidism + metabolic state) |
| Platelets | PLT 125-162 (trending down), MPV ↑ | ITP (autoimmune, associated with thyroid autoimmunity) |
| RBCs | HCT 50-53%, Reticulocytes 1.74% ↑, RDW-SD ↑ | Relative erythrocytosis with active marrow; hemolysis less likely given normal bilirubin |
| Glycemia | HbA1c 4.60% - perfect | Excellent; insulin resistance possible but not yet affecting glucose |
This is an educational interpretation. Formal diagnosis and treatment decisions must be made by the treating physician with full clinical context.
Give non pharmacological treatment and suggest some lifestyle modifications and also suggest some dietary habits to improve these conditions along with pharmacological treatment
NAFLD hypertriglyceridemia subclinical hypothyroidism ITP lifestyle diet treatment guidelines 2024 2025
ITP immune thrombocytopenia lifestyle precautions diet exercise restrictions management
Complete Treatment Guide for Mr. Lakshay, 24M
Addressing: NAFLD/Liver Injury | Subclinical Hypothyroidism | Hypertriglyceridemia | ITP (Thrombocytopenia) | Borderline Erythrocytosis
CONDITION 1: NAFLD / Liver Injury (ALT 104, GGT 108, ALP 121)
Non-Pharmacological Treatment
- Aerobic exercise: Brisk walking, jogging, cycling, swimming - 150 to 200 minutes per week (30-40 min/day, 5 days/week). This directly reduces hepatic fat even without significant weight loss
- Resistance training: 2-3 sessions per week (weights, bodyweight squats, push-ups). Muscle-building improves insulin sensitivity and reduces liver fat independently of aerobic exercise
- A 5-7% reduction in body weight through exercise alone reduces ALT levels and liver fat significantly within 8-12 weeks
- Start gradually - even 20 minutes of daily walking creates measurable improvement
- Zero alcohol - even small amounts of alcohol dramatically worsen liver inflammation when ALT/GGT are already elevated. Alcohol is the most hepatotoxic lifestyle factor for this patient
- Avoid all hepatotoxic supplements - many ayurvedic/herbal preparations, high-dose protein supplements, and fat-burners are directly hepatotoxic
- No self-medication with NSAIDs (ibuprofen, diclofenac) - these worsen liver injury and also suppress platelet function
- Screen for sleep apnea - it causes hypoxia (relevant to erythrocytosis) and worsens insulin resistance/NAFLD. If snoring + daytime fatigue are present, a sleep study is warranted
Dietary Habits for Liver Health
- Olive oil (1-2 tbsp/day) - monounsaturated fats reduce hepatic fat; substitute ghee/butter with olive or mustard oil for cooking
- Coffee (plain, unsweetened) - 2-3 cups/day has strong evidence for reducing liver fibrosis and GGT levels; one of the most liver-protective dietary habits known
- Green leafy vegetables (spinach, methi, sarson) - rich in folate and antioxidants; support liver detoxification pathways
- Cruciferous vegetables (broccoli, cauliflower, cabbage) - sulforaphane compounds support hepatocyte health
- Walnuts, almonds, flaxseeds - plant-based omega-3 fatty acids
- High-fiber foods: Oats, brown rice, whole pulses, raw vegetables - slow glucose absorption, reduce triglyceride synthesis
- Turmeric (haldi) - curcumin has documented anti-inflammatory and hepatoprotective effects; 1 tsp daily in food is beneficial
- Maida (refined wheat flour) and white rice - these cause rapid glucose spikes that drive hepatic fat production (de novo lipogenesis)
- Packaged/processed foods - hidden trans-fats, high fructose corn syrup, and seed oils
- Sugary drinks (cold drinks, packaged juices, sherbet) - fructose is the primary driver of NAFLD; even "healthy" fruit juices in excess are harmful to the liver
- Refined sugar and sweets - mithai, chocolates, biscuits - directly converted to liver fat
- Fried foods (samosas, pakoras, chips) - saturated and trans-fat overload
- Red meat in excess - processed meats (sausage, salami) are associated with worse liver disease
CONDITION 2: Hypertriglyceridemia (TG 188, VLDL 37)
Non-Pharmacological Treatment
Dietary Habits for Triglycerides
- Eliminate sugary drinks completely - liquid sugar/fructose raises triglycerides faster than any other food. This includes packaged juices
- Reduce refined carbohydrates - less roti/rice at each meal; replace with more dal, vegetables, and protein
- Omega-3 fatty acids - HIGH PRIORITY:
- Fatty fish: Mackerel (bangda), sardines, salmon - 2-3 servings/week
- Flaxseeds (alsi): 1 tbsp ground daily in curd or roti dough
- Walnuts: 5-6 walnuts daily
- Omega-3s directly suppress hepatic VLDL synthesis and lower triglycerides by 15-30%
- Reduce simple carbohydrates at dinner especially - the liver converts late-night carbs most efficiently into triglycerides
- Increase dietary fiber: Psyllium husk (Isabgol) 1 tsp in water before meals - reduces triglyceride absorption
- Strictly limit alcohol - even one drink significantly raises triglycerides in susceptible individuals
Pharmacological Treatment (if lifestyle fails after 3 months)
- Fenofibrate 145 mg once daily - first-line drug for isolated hypertriglyceridemia; reduces TG by 30-50% and raises HDL
- Omega-3 ethyl esters (Icosapent ethyl / Vascepa) - prescription-strength omega-3; reduces TG by up to 30%
- Niacin (extended-release) - effective but causes flushing; less commonly used now
- Note: Statins (atorvastatin) target LDL, not TG; since LDL is normal here, a statin is not the primary drug
CONDITION 3: Subclinical Hypothyroidism + Borderline Hashimoto's (TSH 5.74, Anti-TPO 15.2)
Non-Pharmacological Treatment
- Cortisol (stress hormone) directly suppresses thyroid function and worsens autoimmune activity
- Yoga and meditation: 20-30 minutes daily - pranayama (especially Anulom Vilom and Kapalbhati) specifically supports thyroid function and stress reduction
- Adequate sleep: 7-8 hours is mandatory; sleep deprivation raises TSH and worsens thyroid autoimmunity
- Avoid overtraining/excessive exercise - paradoxically, extreme physical stress raises cortisol and suppresses thyroid
- Avoid taking iodine supplements without medical supervision - excess iodine can trigger or worsen Hashimoto's thyroiditis
- Avoid raw goitrogenic vegetables in large amounts (raw cabbage, broccoli, cauliflower, kale in excess) - these contain compounds that inhibit thyroid peroxidase. Cooking neutralizes most goitrogens, so cooked portions are fine
Dietary Habits for Thyroid
- Selenium-rich foods: Brazil nuts (2/day), sunflower seeds, eggs, mushrooms - selenium is critical for thyroid peroxidase function and reduces Anti-TPO antibodies over time
- Zinc-rich foods: Pumpkin seeds (kaddu ke beej), chickpeas, lentils, eggs - zinc supports thyroid hormone conversion
- Iodized salt in normal cooking quantities - adequate but not excessive iodine intake
- Vitamin D: Sunlight exposure 20-30 minutes daily (important for autoimmune modulation); vitamin D deficiency is common in Hashimoto's and worsens it
- Soy products in excess (if taking levothyroxine in future, soy interferes with absorption)
- Gluten - some evidence suggests a gluten-free or reduced-gluten diet may lower Anti-TPO antibodies in Hashimoto's; worth trialing for 3-6 months
Pharmacological Treatment
- At TSH 5.74 with symptoms: Most guidelines recommend starting levothyroxine (L-T4) at a low dose (25-50 mcg once daily in the morning, 30-45 minutes before food/tea)
- Dosing principle: Start low, titrate every 6-8 weeks based on TSH; target TSH 1-3 in a 24-year-old
- If TSH <10 and truly asymptomatic: Some guidelines suggest watchful waiting with repeat TSH in 3-6 months before starting treatment
- Anti-TPO monitoring: Repeat every 6 months; rising Anti-TPO despite normal TSH after treatment may need specialist review
- Vitamin D supplementation (60,000 IU weekly for 8 weeks then monthly) if serum 25-OH Vitamin D is low - highly recommended to check
CONDITION 4: ITP / Thrombocytopenia (PLT 125 → falling from 162)
Non-Pharmacological Treatment - Safety First
- Avoid contact sports and high-impact activities - football, wrestling, martial arts, cricket (batting/fielding with hard ball) carry significant risk of internal bleeding or head injury with low platelets
- Safe exercise alternatives: Swimming (pool, not competitive), stationary cycling, yoga, brisk walking - these are excellent and do not carry bleeding risk
- Use soft-bristle toothbrush to prevent gum bleeding
- Be cautious with razors - electric shaver preferred to avoid skin cuts
- Avoid unnecessary injections/blood draws from arms with haematomas
- Aspirin (even in low dose) - absolutely contraindicated when platelet count is low
- NSAIDs (ibuprofen, diclofenac, naproxen) - impair platelet aggregation
- Alcohol - directly suppresses platelet production in bone marrow AND is hepatotoxic
- Herbal supplements with antiplatelet effects: Ginkgo biloba, garlic supplements in large doses, fish oil in very high doses (>4g/day)
- Psychological stress activates the immune system and can worsen autoimmune platelet destruction. Mindfulness meditation and adequate sleep directly reduce immune system hyperactivation
Dietary Habits for Platelets
- Papaya leaf extract - has traditional and some clinical evidence for raising platelet counts; fresh papaya and papaya leaf juice are commonly used in India
- Pomegranate juice - rich in antioxidants that support platelet formation
- Pumpkin and pumpkin seeds - beta-carotene and zinc support megakaryocyte production
- Leafy greens high in Vitamin K (spinach, methi, bathua) - Vitamin K is required for platelet function and clot formation
- Wheatgrass juice - some evidence for supporting platelet production
- Beetroot - rich in nitrates and iron; supports hematopoiesis
- Coconut water - hydration and electrolyte support
- Alcohol - direct bone marrow suppressant; absolutely avoid
- Quinine (tonic water) - can trigger immune-mediated platelet destruction
- Aspartame/artificial sweeteners in excess - some evidence of platelet function impairment
- High doses of vitamin E supplements - anticoagulant effect
Pharmacological Treatment
| Platelet Level | Treatment |
|---|---|
| >30,000 with no bleeding (current level) | Monitor closely (weekly CBC); no medication required yet |
| <30,000 with minor mucocutaneous bleeding | Dexamethasone 40 mg/day orally for 4 days (preferred over prednisone for initial treatment) |
| <20,000 or significant bleeding | Hospital admission; add IVIG 1g/kg to corticosteroids |
| <10,000 or life-threatening bleed | IVIG + steroids + consider eltrombopag (TPO receptor agonist) |
| Chronic refractory ITP | Rituximab (anti-CD20), splenectomy as last resort |
- Important: Since thrombocytopenia here may be secondary to subclinical hypothyroidism/Hashimoto's, treating the thyroid with levothyroxine may independently improve the platelet count
- Avoid platelet transfusions unless life-threatening bleeding - they are rapidly destroyed in ITP
CONDITION 5: Borderline Erythrocytosis (HCT 49-53%, RBC elevated)
Non-Pharmacological Treatment
- Drink 3-3.5 litres of water daily - relative polycythemia (dehydration-related) resolves completely with proper hydration; even true erythrocytosis is less symptomatic when well-hydrated
- Avoid tea/coffee as primary fluid sources - these are mildly diuretic
- Carry a 1-litre water bottle and complete 3 refills daily
- Good hydration + avoiding diuretics (tea, alcohol, caffeine excess) reduces blood viscosity
- Low-dose aspirin is used in polycythemia vera to reduce clot risk - but CANNOT be given here due to concurrent thrombocytopenia (contradictory indication). This makes it even more important to stay hydrated and avoid dehydration
Consolidated Daily Routine - Practical Guide
Morning
| Time | Action |
|---|---|
| 6:30 AM | Wake up. 2 glasses of warm water |
| 6:45 AM | 20-30 min yoga/pranayama (Anulom Vilom, Kapalbhati) - supports thyroid, reduces stress |
| 7:15 AM | 30-40 min brisk walk or jogging |
| 8:00 AM | Breakfast (see meal plan below) |
| (If starting levothyroxine) | Take it 30-45 min BEFORE breakfast, with plain water only |
Meal Plan Framework
- Vegetable oats upma or daliya with vegetables
- 2 boiled eggs or a bowl of curd (dahi)
- 1 tbsp ground flaxseeds mixed into curd
- 1-2 walnuts
- Plain black/green tea or filter coffee (no sugar)
- A handful of mixed nuts (almonds, walnuts, pumpkin seeds)
- Seasonal fruit (apple, papaya, pomegranate preferred)
- 1-2 chapatis (whole wheat/multigrain) - reduce from previous quantity if more than 3
- Dal (any lentil - protein + fiber)
- 2 vegetable sabzis (one leafy green essential)
- Small bowl of curd/raita
- Salad with olive oil dressing
- Herbal tea or plain coffee
- Sprouts chaat or roasted chickpeas
- More vegetables, less grain/rice
- Grilled/roasted fish or paneer (protein)
- Soup (vegetable/dal)
- Avoid eating after 9 PM - late-night eating directly raises morning triglycerides
What to Drink Daily
- Water: 3-3.5 litres
- Plain coffee (unsweetened): 2-3 cups (liver protective, reduces GGT)
- Green tea or tulsi tea: 1-2 cups
- Papaya leaf juice (small glass): supports platelet count
- AVOID: Cold drinks, packaged juices, alcohol, excessive tea (tannins interfere with iron absorption)
Supplements Worth Discussing with Your Doctor
| Supplement | Condition | Evidence |
|---|---|---|
| Vitamin D3 (60,000 IU/week) | Hashimoto's, immune regulation | Strong - check levels first |
| Omega-3 (EPA+DHA 2-4g/day) | Triglycerides, liver, anti-inflammatory | Strong |
| Selenium (200 mcg/day) | Hashimoto's, reduces Anti-TPO | Good |
| Magnesium glycinate (300mg/day) | Insulin resistance, sleep, thyroid | Moderate |
| Milk Thistle (Silymarin 140mg TDS) | Liver protection (ALT, GGT) | Good - well-tolerated |
| Berberine (500mg BD with meals) | Triglycerides, insulin resistance, liver | Emerging strong evidence |
What to Monitor and When
| Test | Frequency | Why |
|---|---|---|
| CBC (platelet count) | Every 2-4 weeks | Platelet trend is falling - needs close watch |
| LFT (ALT, GGT, ALP) | Every 6-8 weeks initially | Track liver response to lifestyle changes |
| TSH + Free T4 | Every 3 months (or 6 weeks after starting levothyroxine) | Confirm hypothyroidism and monitor treatment |
| Anti-TPO | Every 6 months | Track Hashimoto's progression |
| Fasting lipid profile (TG, VLDL) | Every 3 months | Track triglyceride response to diet/exercise |
| Ultrasound abdomen | Once now, repeat at 6 months | Baseline liver assessment, then track NAFLD |
| Fasting insulin + HOMA-IR | Once now | Detect insulin resistance even with normal HbA1c |
Important note: This is an educational guide based on the lab reports. All pharmacological treatments - especially levothyroxine, steroids for ITP, and fenofibrate - must be prescribed and monitored by Dr. Sudhir Attri or a specialist. Never self-medicate. Lifestyle and dietary changes can begin immediately and will produce measurable improvement within 8-12 weeks.