Asd murmur
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is a complete summary of the ASD murmur:
Atrial Septal Defect (ASD) - Murmur & Clinical Features
Key Auscultatory Findings
The hallmark of ASD on auscultation is the wide, fixed splitting of S2 (the second heart sound). This is the most distinctive feature and what differentiates ASD from other causes of a split S2.
Why fixed splitting occurs: Normally, S2 splits wider on inspiration (increased venous return to the right heart delays pulmonary valve closure). In ASD, inspiration increases venous return but simultaneously increases the right atrial pressure, which decreases left-to-right shunting. These two effects cancel each other out, so the splitting remains constant throughout the respiratory cycle - hence "fixed." - Goldman-Cecil Medicine, p. 984
The Murmur Itself
| Feature | Details |
|---|---|
| Type | Soft midsystolic (systolic ejection) murmur |
| Grade | 2-3/6 |
| Location | Second to third left intercostal space (left upper sternal border / LUSB) |
| Mechanism | Increased flow across the pulmonary valve (not through the ASD itself - the ASD shunt is low velocity and usually silent) |
| Character | Crescendo-decrescendo (ejection pattern) |
Note: The left-to-right shunt across the ASD is low-velocity and generally silent. The murmur is generated by the increased pulmonary flow through the pulmonic valve, not by blood moving through the defect itself. - Harrison's Principles of Internal Medicine 22E (2025)
Additional Murmur: Mid-Diastolic Rumble
In large left-to-right shunts, a mid-diastolic rumble may be heard at the lower left sternal border (LLSB) due to increased flow across the tricuspid valve. This indicates a hemodynamically significant shunt (Qp:Qs typically >2:1). - Goldman-Cecil Medicine, p. 984
Summary of Auscultation (Harriet Lane, 23rd Edition)
| Finding | Detail |
|---|---|
| S2 splitting | Wide, fixed split |
| Systolic murmur | Grade 2-3/6 SEM at LUSB |
| Diastolic murmur | Mid-diastolic rumble at LLSB (if large shunt) |
Other Physical Examination Findings
- Right ventricular heave/impulse - palpable at the left parasternal area (expiration) or subxiphoid area (inspiration) if significant shunt exists
- Dilated pulmonary artery - may be palpable in the 2nd left intercostal space
- No thrill (unlike VSD)
ECG Findings
- Incomplete right bundle branch block (RBBB) - rSr' or rsR' pattern in V1 - the hallmark ECG finding
- Right axis deviation (RAD)
- With large ASD: mild RVH with RSR' in V1
- Prolonged PR interval possible
- Atrial fibrillation or flutter (in older/adults with long-standing ASD)
Chest X-Ray
- Pulmonary vascular plethora (increased pulmonary vascular markings bilaterally)
- Dilated main pulmonary artery and its branches
- Right atrial and right ventricular enlargement
- May show cardiomegaly if hemodynamically significant
Types of ASD & Prevalence
| Type | Frequency | Location |
|---|---|---|
| Secundum | ~90% | Fossa ovalis / central septum - deficiency of septum secundum |
| Primum | ~5% | Adjacent to AV valves; often with AV valve abnormalities ± VSD |
| Sinus venosus | ~5% | Near SVC entrance; may have anomalous pulmonary venous return |
- Robbins Pathologic Basis of Disease

Pathophysiology
The primary defect causes a left-to-right shunt (since left atrial pressure > right atrial pressure postnatally). Chronic large shunting (Qp:Qs >3:1) causes:
- Right heart volume overload and enlargement
- Increased pulmonary blood flow
- Eventually pulmonary hypertension (less common in secundum ASD than in VSD/PDA)
- Risk of paradoxical embolism and stroke (right-to-left shunting during straining/Valsalva)
Clinical Course
- Most children are asymptomatic in the first 2-3 decades
- Symptoms emerge in adulthood: dyspnea on exertion, palpitations, fatigue
-
70% become symptomatic by the fifth decade - Goldman-Cecil Medicine
- Atrial arrhythmias (AF, flutter) are common late complications
Differentiation from Innocent Murmur
ASD murmur can be confused with an innocent pulmonary ejection murmur. The key distinguishing feature is the fixed splitting of S2 - innocent murmurs do not cause fixed S2 splitting. - Harrison's Principles of Internal Medicine 22E
Treatment Indications
- ASD closure (percutaneous or surgical) is indicated when right-sided heart enlargement is present, with or without symptoms
- Centrally located secundum ASD up to 3.5 cm can be closed by transcatheter device (Amplatzer septal occluder)
- Surgical closure uses direct suture, autologous pericardium, or prosthetic patch under cardiopulmonary bypass
- Most centers recommend closure before school age - Sabiston Textbook of Surgery
Vsd murmur
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed. Here is a comprehensive answer:
Ventricular Septal Defect (VSD) - Murmur & Clinical Features
The Murmur - Key Features
| Feature | Details |
|---|---|
| Type | Holosystolic (pansystolic) murmur |
| Grade | 2-5/6 (louder with smaller defects due to higher velocity jet) |
| Location | Lower left sternal border (LLSB) - 3rd to 4th left intercostal space |
| Radiation | Throughout the precordium |
| Thrill | Palpable systolic thrill at LLSB (common with moderate-large defects) |
| Quality | Harsh, blowing |
| Timing | Begins with S1 and continues to S2 (holosystolic/pansystolic) |
"A ventricular septal defect is usually manifested by a holosystolic murmur with a palpable thrill along the mid- to lower left sternal edge." - Harrison's Principles of Internal Medicine 22E (2025)
Why holosystolic? Throughout systole, left ventricular pressure exceeds right ventricular pressure, driving a continuous left-to-right jet across the defect from S1 all the way to S2.
Additional Murmur: Apical Mid-Diastolic Rumble
With large shunts, increased flow returning from the lungs causes relative mitral stenosis, producing a mid-diastolic rumble at the apex. This indicates a hemodynamically significant VSD (Qp:Qs >2:1). - Harriet Lane Handbook, 23rd ed.
"Maladie de Roger" - The Small VSD Paradox
A very small VSD (maladie de Roger) produces a very loud, harsh murmur with a palpable thrill, yet is physiologically trivial. This occurs because the tiny defect creates a very high-velocity jet. As the VSD enlarges (or becomes non-restrictive), the murmur may actually soften as the pressure gradient between ventricles falls.
Summary Table (Harriet Lane, 23rd Edition)
| Parameter | Small VSD | Medium VSD | Large VSD |
|---|---|---|---|
| Murmur | 2-5/6 holosystolic at LLSB ± thrill | Same + apical diastolic rumble | Same; may soften if pulmonary HTN develops |
| ECG | Normal | LVH ± LAE | BVH ± LAE or pure RVH |
| CXR | Normal | Cardiomegaly + increased PVMs | Marked cardiomegaly + pulmonary overcirculation |
| S2 | Normal | May be narrow with pulmonary HTN | P2 loud/narrow split if Eisenmenger |
Types of VSD by Location
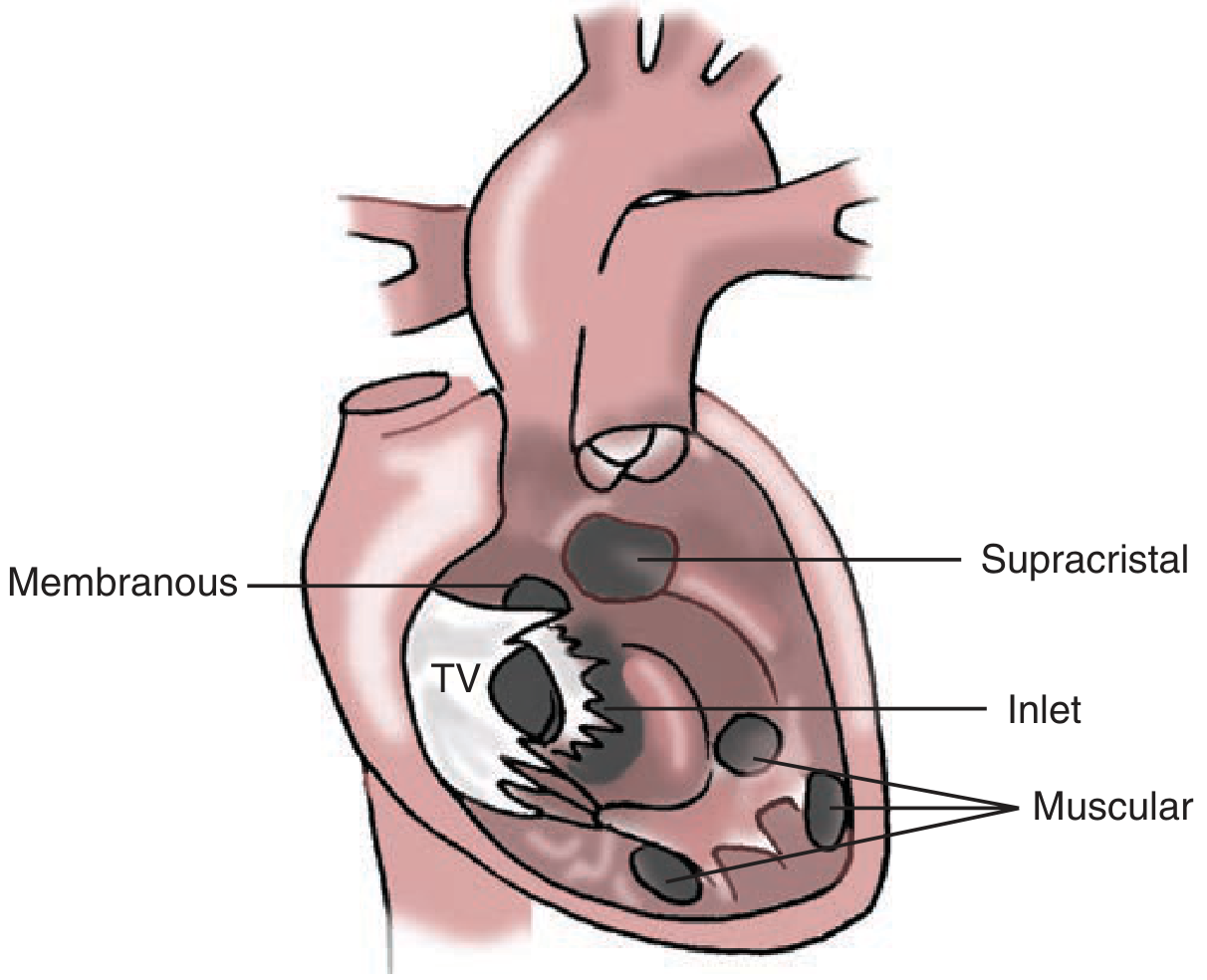
| Type | Frequency | Location |
|---|---|---|
| Perimembranous (membranous) | ~80% | Below aortic valve in membranous septum; most common type requiring surgery |
| Muscular | Most common overall | Trabecular septum; may be multiple ("Swiss cheese"); often close spontaneously |
| Supracristal (outlet/infundibular) | Uncommon | Conal septum, below pulmonary valve |
| Inlet (AV canal type) | ~5% | Below tricuspid valve, near AV valves; associated with Down syndrome |
- Schwartz's Principles of Surgery, 11th Ed.; Goldman-Cecil Medicine
Pathophysiology
- Small/restrictive VSD: High-pressure gradient between LV and RV → loud murmur, low flow, Qp:Qs <1.5, normal PA pressure. Right heart unaffected.
- Moderate VSD: Qp:Qs >1.2, elevated PA pressure but PVR still low. Left heart volume overload (left atrial and ventricular dilation).
- Large/non-restrictive VSD: High Qp:Qs (≥1.5), elevated PA pressure and PVR. Right heart affected. Risk of Eisenmenger syndrome (~10% of large VSDs).
Natural History
- ~50% of small muscular VSDs close spontaneously
- Closure rates highest in the first decade; unusual after that
- Infants at 1 month: ~80% chance of spontaneous closure; at 12 months: only ~25%
- Large unclosed VSDs almost universally progress to irreversible pulmonary vascular disease
Eisenmenger Syndrome - What Happens to the Murmur
When pulmonary hypertension develops and pressures equalize (then reverse), the left-to-right shunt diminishes and the holosystolic murmur softens or disappears. Cyanosis appears. A loud, single P2 and signs of right heart failure replace the original murmur.
ECG Findings
- Small VSD: Normal
- Moderate VSD: LVH ± left atrial enlargement (LAE)
- Large VSD: Biventricular hypertrophy (BVH) ± LAE, or pure RVH if pulmonary hypertension is dominant
Chest X-Ray
- Small VSD: Normal
- Moderate-large VSD: Cardiomegaly, increased pulmonary vascular markings (pulmonary plethora)
- Eisenmenger: Enlarged proximal pulmonary arteries with peripheral pruning
Complications
- Infective endocarditis - the turbulent jet causes endocardial damage that acts as a nidus for bacterial colonization, even with small restrictive defects
- Aortic regurgitation - particularly with supracristal VSDs, the aortic valve cusp can prolapse into the defect
- Eisenmenger syndrome - irreversible pulmonary vascular disease with shunt reversal
- Heart failure - with large shunts in infancy
VSD vs ASD Murmur - Quick Comparison
| Feature | VSD | ASD |
|---|---|---|
| Type | Holosystolic (pansystolic) | Midsystolic ejection murmur |
| Location | LLSB (3rd-4th ICS) | LUSB (2nd-3rd ICS) |
| S2 | Normal (or loud P2 if PHT) | Wide, FIXED splitting |
| Thrill | Yes (common) | Rare |
| Mechanism | Direct shunt jet across septum | Increased flow across pulmonic valve |
| Diastolic component | Apical rumble (mitral) | LLSB rumble (tricuspid) |
Ecgo findings bith
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
I now have all the echo images and data needed. Here is a comprehensive comparison:
Echocardiographic Findings: ASD vs VSD
ASD - Echocardiographic Findings
2D Echo
| Finding | Detail |
|---|---|
| Septal dropout | Echo dropout (apparent gap) in the atrial septum - best seen in subcostal 4-chamber view |
| RV dilation | Right ventricular enlargement due to chronic volume overload |
| RA dilation | Right atrial enlargement |
| Paradoxical septal motion | Interventricular septum moves paradoxically (toward LV in systole) due to RV volume overload |
| Dilated pulmonary artery | Enlarged main pulmonary artery and branches |
| LA and LV | Normal or small (blood preferentially shunts to right side) |
Best views: Subcostal 4-chamber (most reliable for detecting ASD - avoids near-field dropout artifact), apical 4-chamber, parasternal short-axis. TEE is superior for sinus venosus and small defects.
Color Doppler
- Left-to-right color flow jet crossing from LA to RA through the atrial septum
- Turbulent (aliased) color signal at the defect site
- TTE Color Doppler apical 4-chamber view showing LA-to-RA shunt:
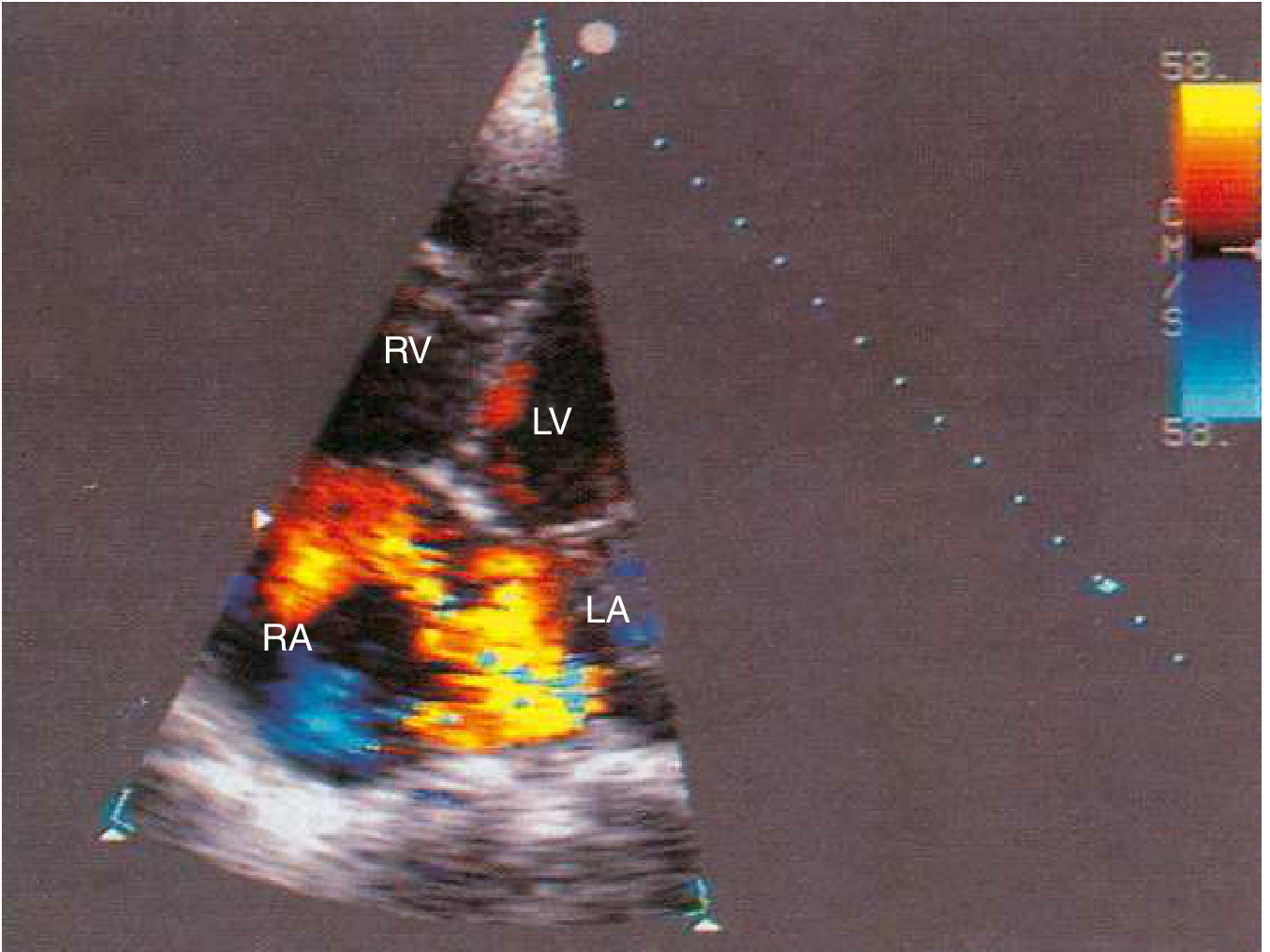
Color flow Doppler: LA-to-RA shunt through a moderately sized ASD (Goldman-Cecil Medicine)
- TEE provides superior resolution to measure defect size and rims for device planning:
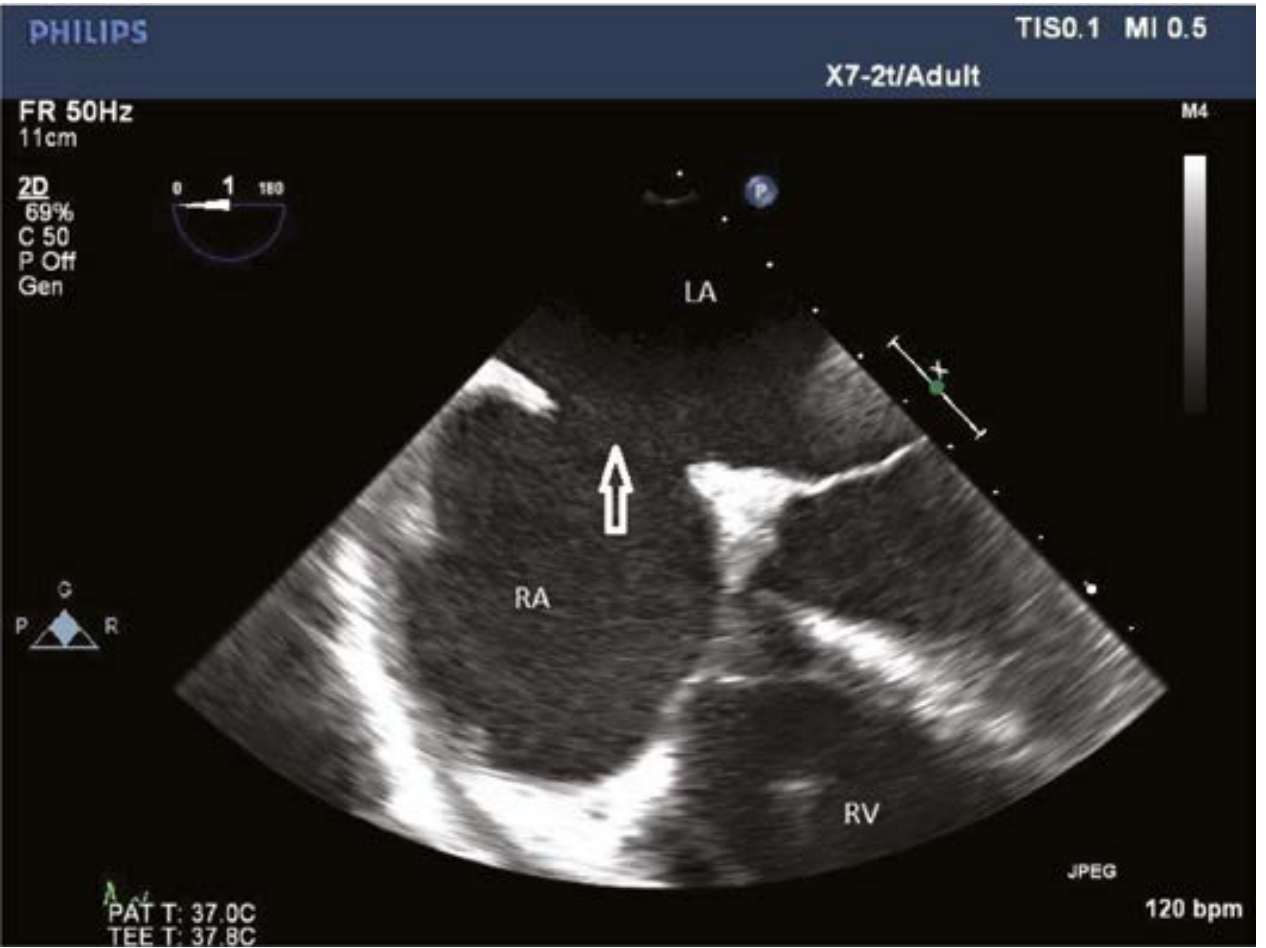
TEE: Large secundum ASD (arrow) with LA above, RA below, RV at bottom (Creasy & Resnik's Maternal-Fetal Medicine)
Doppler Findings
| Modality | Finding |
|---|---|
| Pulsed wave (PW) | Increased systolic flow velocity in pulmonary artery |
| Continuous wave (CW) | Low-velocity (laminar) flow across defect - confirms low-pressure shunt |
| TR jet velocity | Used to estimate pulmonary artery systolic pressure (PASP = 4v² + RAP) |
| Qp:Qs calculation | Ratio of pulmonary to systemic flow quantified via RVOT and LVOT Doppler |
Key ASD Echo Points
- Sinus venosus ASD is easily missed on TTE - TEE or bubble contrast is needed
- Agitated saline (bubble) contrast - microbubbles appear in LA if right-to-left shunting (with Valsalva); helps detect PFO/ASD
- TTE is diagnostic for ostium secundum and primum; TEE needed for complete sinus venosus evaluation
- Ostium primum ASD: look for associated cleft mitral valve and AV valve abnormalities
VSD - Echocardiographic Findings
2D Echo
| Finding | Detail |
|---|---|
| Septal dropout | Gap in the interventricular septum - location identifies type |
| LV dilation | Left ventricular and left atrial enlargement (LV volume overload from pulmonary venous return) |
| RVH | Right ventricular hypertrophy if pulmonary hypertension develops |
| LA dilation | Dilated left atrium due to increased pulmonary venous return |
| Dilated pulmonary artery | With large shunts/pulmonary hypertension |
Best views: Parasternal long-axis (membranous/perimembranous VSD below aortic valve), parasternal short-axis (inlet, muscular VSDs), apical 4-chamber (all types), subcostal.
2D + Color Doppler VSD (Parasternal Long-Axis):
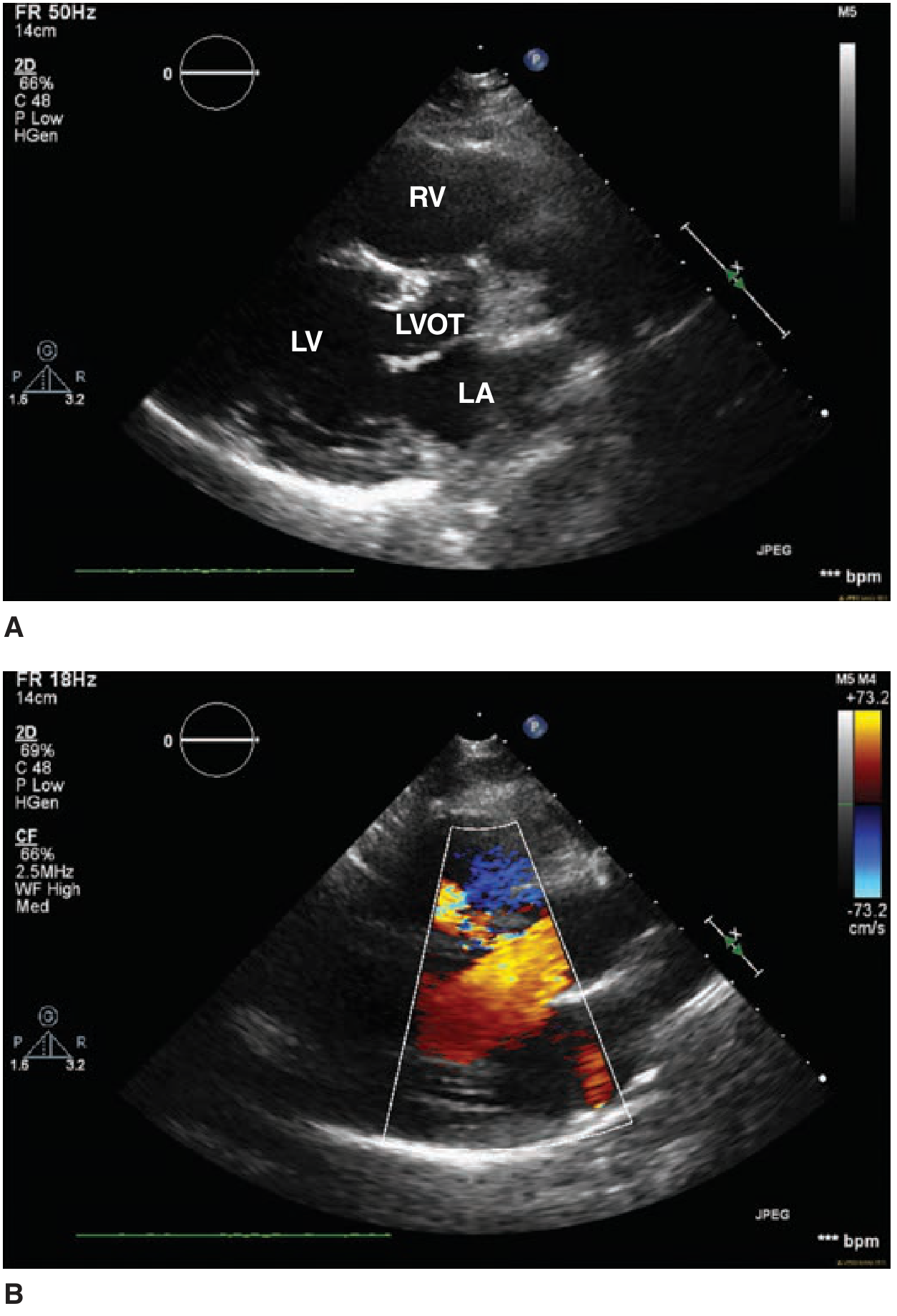
(A) 2D: Disruption of normal tissue structure in the membranous septum just below LVOT. (B) Color Doppler: Turbulent left-to-right systolic jet across the defect - Fuster & Hurst's The Heart, 15th Edition
Color Doppler
- High-velocity turbulent jet from LV to RV in systole (aliased red/blue mosaic)
- Jet direction: left-to-right (unless Eisenmenger)
- Jet seen predominantly in systole (vs ASD which is seen throughout cardiac cycle)
- Location of the jet on color Doppler identifies the type of VSD
Doppler Findings
| Modality | Finding |
|---|---|
| CW Doppler | High-velocity systolic jet across VSD (typically 4-5 m/s with restrictive VSD) |
| Pressure gradient | Using modified Bernoulli: ΔP = 4v²; e.g., 4 m/s → 64 mmHg gradient |
| RVSP estimation | RVSP = systolic BP - VSD gradient (if RVSP is near systolic BP → non-restrictive or near Eisenmenger) |
| TR jet | Independent estimate of PASP |
| Qp:Qs | Calculated via RVOT/LVOT Doppler to quantify shunt severity |
Key VSD Echo Points
- Echo identifies the defect, assesses LA and LV size (determines hemodynamic significance), estimates PA pressure, and detects RV hypertrophy - Goldman-Cecil Medicine, p. 1043
- Small restrictive VSD: Normal LV/LA size, high-velocity jet, normal PA pressure
- Large non-restrictive VSD: Dilated LV/LA, low-velocity jet, elevated PA pressure, RVH
- Eisenmenger: RV hypertrophy, dilated PA, bidirectional or right-to-left shunt on color Doppler; LV may be small
- Supracristal VSD - look for prolapse of right coronary cusp of aortic valve causing aortic regurgitation (seen in parasternal long-axis view)
ASD vs VSD Echo - Side-by-Side Comparison
| Echo Parameter | ASD | VSD |
|---|---|---|
| Defect location | Atrial septum | Interventricular septum |
| Best 2D view | Subcostal 4-chamber | Parasternal long-axis / short-axis |
| Color jet | LA→RA (low velocity, laminar) | LV→RV (high velocity, turbulent mosaic) |
| Jet timing | Throughout cardiac cycle | Predominantly systolic |
| RV | Dilated (volume overload) | Hypertrophied (if PHT); otherwise normal |
| LV | Normal or small | Dilated (volume overload) |
| LA | Normal | Dilated (large shunt) |
| RA | Dilated | Normal |
| Paradoxical septal motion | Yes (RV volume overload) | No (unless severe PHT) |
| PA pressure | Mildly elevated | Can be markedly elevated |
| Bubble contrast | Bubbles cross to LA (R→L with Valsalva) | Not typically used |
| TEE advantage | Sinus venosus ASD, device sizing | Inlet/muscular VSD, AR complication |
| CW Doppler velocity | Low (~1-1.5 m/s) | High (~4-5 m/s restrictive) |
- Sources: Textbook of Clinical Echocardiography; Goldman-Cecil Medicine; Fuster & Hurst's The Heart, 15th Ed.; Schwartz's Principles of Surgery, 11th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.