Ecg
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Searching Images
atrial fibrillation ECG pattern
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Atrial Fibrillation (AF) on ECG.
ECG Features of Atrial Fibrillation
(Table 18-8, Tintinalli's Emergency Medicine)
| Feature | Detail |
|---|---|
| P waves | Absent — replaced by flat or chaotic baseline (fibrillatory f-waves) |
| Baseline | Irregular oscillations, most prominent in lead V1 |
| Ventricular rhythm | Irregularly irregular — no repeating pattern to R-R intervals |
| QRS complexes | Narrow (normal) — unless pre-existing BBB or pre-excitation syndrome |
| Ventricular rate | Typically 120–170 bpm (unmedicated); can exceed 200 bpm with accessory pathways |
Classic ECG Examples of AF
Three examples of AF with irregular ventricular response (from Tintinalli's):
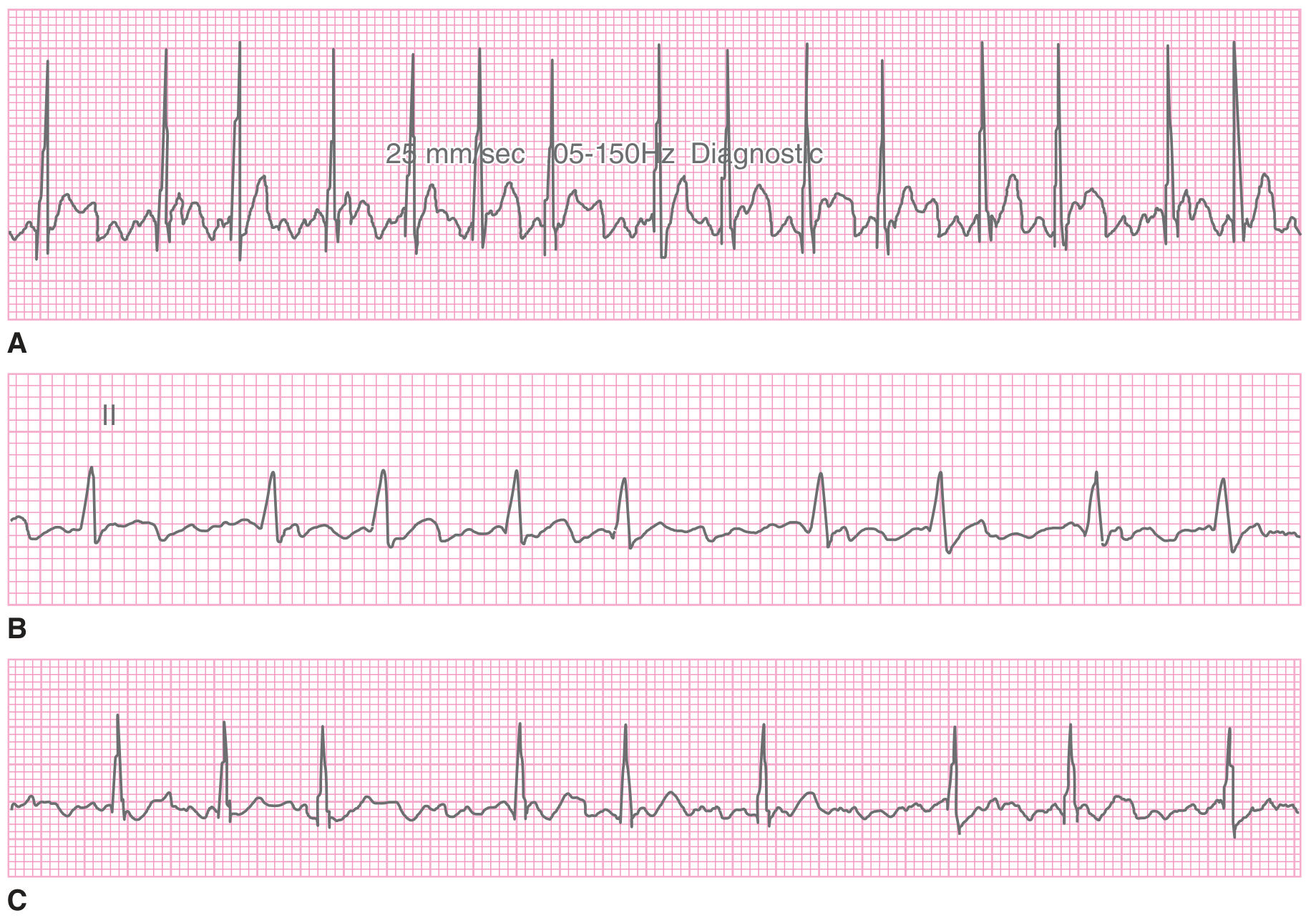
(A) Rapid, chaotic baseline with fast ventricular response
(B) Clearly irregular R-R intervals in lead II, no P waves
(C) Slower ventricular rate — note the variable spacing between QRS complexes
And a 12-lead ECG demonstrating classic AF with a single PVC:
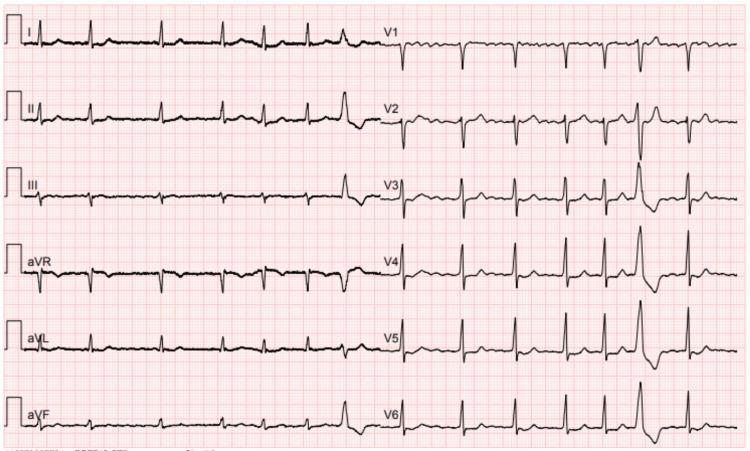
Key features visible: absent P waves, irregular R-R intervals, narrow QRS complexes, one wide PVC beat.
Mechanism
- Chaotic, disorganized electrical activity in the atria fires at rates >600 bpm
- The AV node acts as a "gatekeeper" — its refractory period limits ventricular response to ~120–170 bpm
- Because conduction is random, ventricular rhythm is never regularly irregular — it is truly random
How to Distinguish from Similar Rhythms
| Rhythm | Key Difference |
|---|---|
| Atrial Flutter | Regular sawtooth flutter waves ~300 bpm; ventricular rhythm often regular (2:1 block → ~150 bpm) |
| Multifocal Atrial Tachycardia (MAT) | ≥3 distinct P wave morphologies; P waves are present; often confused with AF |
| AF + BBB | Wide QRS complexes; can mimic VT |
| AF + WPW | Very rapid rate (>200 bpm), delta waves, wide bizarre QRS |
Clinical Significance
Common causes:
- Ischemic heart disease / valvular disease (most common)
- Congestive cardiomyopathy, myocarditis
- Thyrotoxicosis
- Alcohol binge ("holiday heart")
- Blunt chest trauma
Consequences of AF:
- Loss of atrial kick — reduces ventricular filling, can precipitate heart failure
- Rapid ventricular rate — impairs coronary and systemic perfusion
- Thromboembolism — blood stagnates in the left atrial appendage → clot → stroke
ED Management (Key Principles)
Three pillars of AF management:
- Rate control — beta-blockers, calcium channel blockers, digoxin
- Rhythm conversion — cardioversion (electrical or pharmacological) if <48 hrs or anticoagulated ≥3–4 weeks
- Anticoagulation — use CHADS₂ or CHA₂DS₂-VASc score to risk-stratify
- <12 hrs AF: ~0.3% embolic risk on conversion
- 12–48 hrs: ~1%
-
48 hrs: elevated across all groups — anticoagulate 3–4 weeks before conversion
Sources: Tintinalli's Emergency Medicine (Tbl 18-8), Guyton & Hall Medical Physiology, Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.