CT ABDOMEN CONTRAST AND ABDOMEN TRIPLE PHASE
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
CT abdomen contrast vs triple phase CT indications technique phases explained
Finding Sources
Reading Web Page
https://litfl.com/abdominal-ct-phases
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a thorough, well-structured guide to CT Abdomen with Contrast and Triple-Phase CT of the Abdomen, synthesized from authoritative radiology and surgical textbooks.
CT Abdomen with Contrast
What Is It?
CT abdomen with contrast uses intravenous (IV) iodinated contrast medium to enhance vascular structures, organs, and pathological lesions. Oral contrast may be added to opacify the bowel lumen. The study dramatically improves detection and characterization of lesions compared to non-contrast CT alone.
Indications
- Abdominal pain (suspected appendicitis, diverticulitis, bowel obstruction, perforation)
- Trauma evaluation (hepatic, splenic, renal, mesenteric injuries)
- Detection and staging of abdominal tumors, enlarged lymph nodes, metastases
- Fluid collections (abscess, hemorrhage, ascites)
- Vascular pathology (mesenteric ischemia, aortic aneurysm, venous thrombosis)
- Air outside the GI tract (pneumoperitoneum)
Standard Technique
| Parameter | Detail |
|---|---|
| Patient position | Supine, arms elevated |
| Scan extent | Diaphragm to symphysis pubis |
| Slice thickness | ≤0.75 mm |
| Tube voltage | ≤120 kVp |
| Contrast dose | 100-120 mL non-ionic iodinated contrast at 3-5 mL/s |
| Oral contrast | Given in select cases for bowel opacification |
The upper abdomen is routinely imaged in both arterial and portal venous phases when evaluating solid organ injury or suspected vascular injury.
- Grainger & Allison's Diagnostic Radiology: "Contrast medium should be used whenever possible, with the upper abdomen imaged in both the arterial and portal venous phases."
The Contrast Phases - What Happens After Injection
After IV contrast is injected, the study is timed to capture contrast in different vascular compartments:
| Phase | Timing After Injection | What It Shows Best |
|---|---|---|
| Non-contrast (unenhanced) | Before injection | Calcification, hemorrhage, baseline density |
| Early Arterial | ~25-30 sec | Aorta, celiac/SMA branches, hypervascular lesions |
| Late Arterial (Hepatic Arterial) | ~35-45 sec post-trigger | Hypervascular liver lesions (HCC, FNH, adenoma) |
| Portal Venous | ~70-80 sec | Best overall phase - solid organs, bowel, portal vein, hepatic metastases |
| Delayed / Equilibrium | ~2-5 min | Fibrosis, cholangiocarcinoma, HCC washout, collecting system |
The portal venous phase is the most commonly used single phase for routine abdominal CT - it provides the best balance of solid organ, bowel, and vascular enhancement.
Triple-Phase CT Abdomen
Definition
Triple-phase CT refers to three acquisitions of the liver/abdomen obtained at distinct time points after IV contrast injection:
- Late Arterial Phase (~35-45 sec post bolus trigger)
- Portal Venous Phase (~60-75 sec)
- Delayed Phase (~2-5 minutes)
Note on terminology: Some institutions define triple-phase as Non-contrast + Late Arterial + Portal Venous, and call the above protocol "four-phase." A true non-contrast phase added to the three above makes it a quadruple-phase or four-phase CT. Always confirm your local protocol.
Indications
Triple-phase CT is specifically ordered when characterizing focal liver lesions or staging hepatobiliary and pancreatic malignancies:
| Indication | Rationale |
|---|---|
| Hepatocellular carcinoma (HCC) | Arterial hyperenhancement + venous/delayed washout is diagnostic |
| Focal nodular hyperplasia (FNH) | Central scar enhancement on delayed phase |
| Hepatic adenoma | Arterial enhancement, sometimes with fat or hemorrhage |
| Hemangioma | Peripheral nodular enhancement, progressive fill-in |
| Hypervascular liver metastases | Neuroendocrine, renal cell, thyroid, melanoma |
| Pancreatic adenocarcinoma | Best seen as hypovascular mass on portal venous phase; pancreatic phase (~45s) added |
| Colorectal liver metastases | Staging; triple-phase CT chest/abdomen/pelvis is standard of care |
| Gallbladder carcinoma | Vessel anatomy, liver volume, staging |
| Renal masses (washout protocol) | CT washout to differentiate adenoma from RCC |
- Bailey and Love's Surgery: "Routine staging [of colorectal liver metastases] involves triple-phase CT chest/abdomen/pelvis, contrast MRI scan."
- Washington Manual: "Triple-phase CT or quadruple-phase CT is indicated for liver mass evaluation. A delayed phase is useful when HCC is suspected."
How HCC is Diagnosed on Triple-Phase CT
HCC is a hypervascular tumor supplied predominantly by the hepatic artery. Its imaging hallmark on multiphase CT is:
- Arterial phase hyperenhancement - the lesion enhances brighter than surrounding liver parenchyma
- Portal venous or delayed phase washout - the lesion becomes hypoenhancing (darker) compared to liver
This pattern of arterial enhancement + washout is diagnostic of HCC without biopsy in the appropriate clinical setting (cirrhosis, chronic hepatitis B/C).
The HCC surveillance and LI-RADS diagnostic algorithm shows how multiphase CT integrates into clinical decision-making:
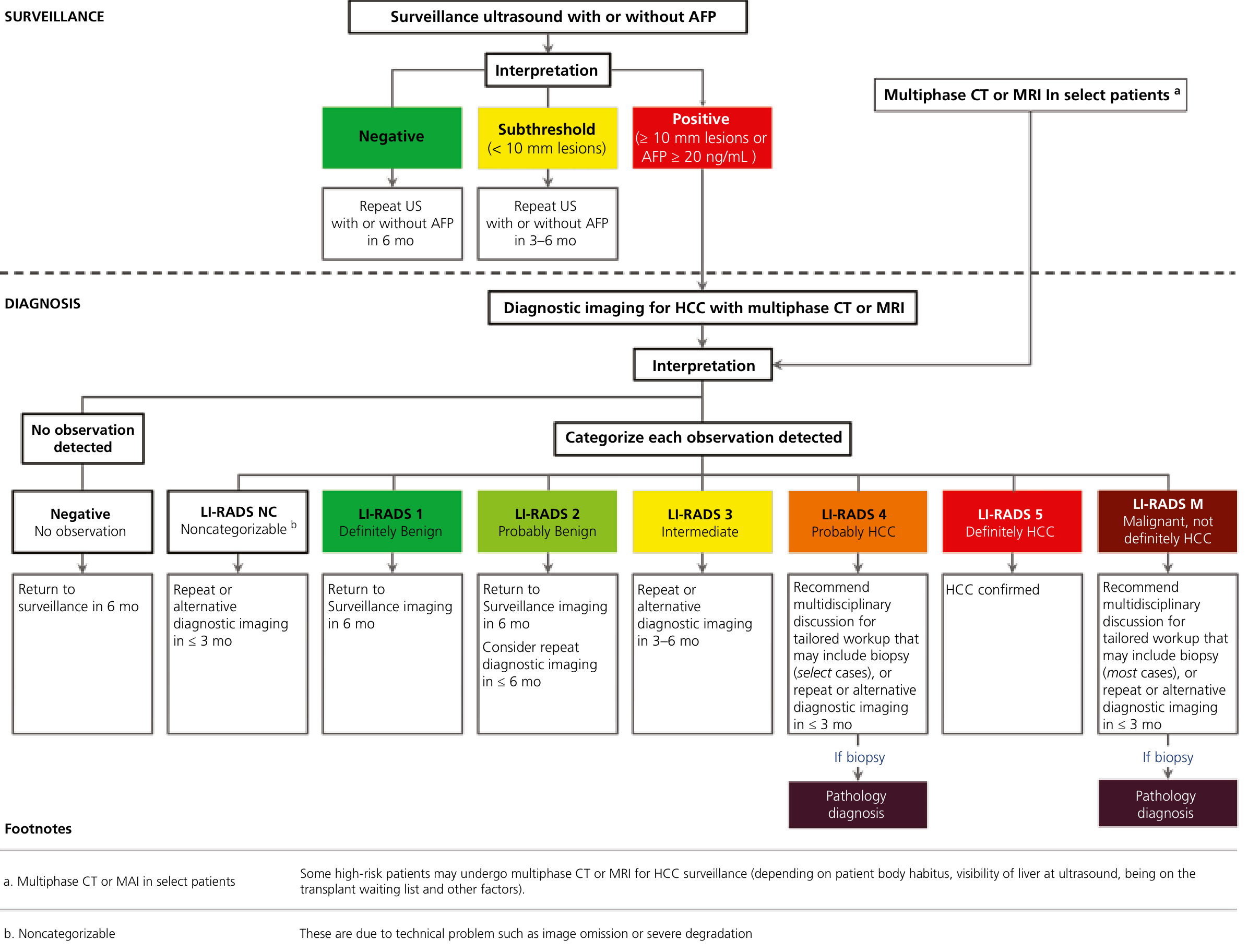
Yamada's Textbook of Gastroenterology - Diagnostic algorithm for HCC with multiphase CT/MRI and LI-RADS categorization
Triple-Phase CT Technique (Radiopaedia Protocol)
- Patient position: Supine, arms above head
- Scout: Diaphragm to iliac crests
- Bolus tracking: ROI placed at aorta at level of diaphragmatic hiatus; threshold = 150 HU
- Contrast: 100-120 mL non-ionic contrast at 3-5 mL/s
- Scan delays:
- Late arterial: 15-30 sec post bolus trigger (35-45 sec after injection start)
- Portal venous: 60-75 sec after injection (independent of arterial timing)
- Delayed: 2-5 minutes
- Respiration: Inspiration, breath-hold for each phase
CT Abdomen Contrast vs. Triple-Phase - Key Differences
| Feature | Standard CT Abdomen Contrast | Triple-Phase CT |
|---|---|---|
| Phases acquired | Usually 1 (portal venous) | 3 (arterial + portal venous + delayed) |
| Radiation dose | Lower | Higher (3x acquisitions) |
| Primary use | General abdominal pathology | Liver/pancreatic lesion characterization |
| Lesion detection | Good for most pathology | Optimized for focal liver lesions, HCC, hypervascular tumors |
| Cost and time | Lower | Higher |
Radiation Considerations
Triple-phase CT delivers significantly higher radiation due to multiple acquisitions. According to research on dose reduction strategies, the unenhanced phase can be acquired at 3-fold reduced tube current without affecting attenuation value measurements, achieving a 22% total dose reduction while maintaining diagnostic quality in the contrast-enhanced phases.
Key principles for dose reduction in CT abdomen:
- Use automatic exposure control (AEC)
- Reduce dose on non-contrast phase (lower image quality acceptable)
- In children: split-bolus technique to achieve both arterial and venous enhancement in a single acquisition (Grainger & Allison's)
- Avoid triple-phase unless specifically clinically indicated
Summary of Clinical Use
| Clinical Question | Recommended CT Protocol |
|---|---|
| Acute abdominal pain (appendicitis, diverticulitis) | CT abdomen/pelvis with IV contrast (portal venous phase) |
| Abdominal trauma | Non-contrast + arterial + portal venous (3-phase) |
| GI bleeding | Non-contrast + arterial + portal venous |
| Liver mass / HCC screening positive | Triple-phase CT (arterial + portal venous + delayed) |
| Colorectal liver mets staging | Triple-phase CT chest/abdomen/pelvis |
| Pancreatic mass | Pancreatic protocol CT (pancreatic phase ~45s + portal venous) |
| Renal mass | CT renal mass / washout protocol |
| Mesenteric ischemia | CT angiography (arterial + portal venous phases) |
Give me the protocol for CT Carotid ANGIO
Finding Sources
Searching the Web
CT carotid angiography protocol technique scan parameters contrast timing CTA neck
Finding Sources
Reading Web Page
https://www.asnr.org/wp-content/uploads/2017/01/5_Cervicocer…
Finding Sources
Searching the Web
CTA carotid protocol radiopaedia scan range kVp mAs slice thickness bolus tracking
Reading File
Reading File
Loading Image
Here is the complete CT Carotid Angiography (CTA Neck) protocol, compiled from ACR-ASNR guidelines, major radiology textbooks, and institutional protocols:
CT Carotid Angiography (CTA Neck) Protocol
Indications
| Clinical Scenario | Detail |
|---|---|
| Carotid artery stenosis | TIA, ischemic stroke, amaurosis fugax |
| Carotid artery dissection | Spontaneous or post-trauma |
| Pre-operative planning | Before carotid endarterectomy (CEA) or carotid artery stenting (CAS) |
| Stroke workup | To assess extracranial and intracranial vessels |
| Aortic arch anatomy | Variant anatomy, subclavian steal, innominate artery disease |
| Carotid body tumor / vascular mass | Characterization |
| Post-procedural follow-up | Post-stent, post-CEA surveillance |
| Vertebrobasilar insufficiency | Vertebral artery origin stenosis |
CTA has an overall sensitivity of 97% and specificity of 99% for detecting carotid stenosis. - Fischer's Mastery of Surgery
Patient Preparation
| Step | Detail |
|---|---|
| IV access | 20G or larger antecubital catheter - preferably RIGHT arm (avoids streak artifact from undiluted contrast in the left brachiocephalic vein) |
| Saline flush test | Test the line with a rapid saline bolus before contrast injection to confirm patency |
| Renal function screening | Check creatinine/eGFR before contrast |
| Allergy history | Document iodine contrast allergy; premedicate if needed |
| Hydration | Adequate IV hydration, especially in CKD patients |
| Patient positioning | Supine, arms along the chest/sides (not above head, as shoulder elevation can degrade neck vessel visualization) |
| Breath hold / respiration | Free breathing / quiet breathing - no breath hold needed (unlike chest CT); swallowing should be avoided during scan |
Right arm injection is preferred per ACR-ASNR guidelines to prevent artifact from undiluted contrast pooling in the left brachiocephalic vein overlying the arch vessels.
Scout / Topogram
- AP and lateral scout
- Coverage from thorax through vertex of skull
- Used to plan scan range
Scan Parameters
| Parameter | Value |
|---|---|
| Scan mode | Helical (mandatory for CTA) |
| Gantry rotation time | ≤0.5 sec per rotation |
| kVp | 100-120 kVp (lower kVp increases contrast enhancement; use 100 kVp in average-sized patients to reduce dose and boost iodine signal) |
| mAs | 180 mAs (AEC preferred - automatic exposure control) |
| Detector collimation | 0.75 mm (16-slice) to 0.5 mm (64-slice and above) |
| Slice thickness (acquisition) | ≤1.5 mm (ACR-ASNR guideline); most institutions use 0.75-1.25 mm |
| Reconstruction interval | ≤50% of slice thickness (i.e., overlapping reconstructions - e.g., 1 mm slices at 0.5 mm increments) |
| Reconstruction kernel | Soft tissue / standard (NOT bone kernel - too noisy for vessels) |
| Pitch | ~0.8-1.0 (fast pitch appropriate for CTA to minimize scan time) |
| FOV | 250-350 mm (adjust to patient) |
Scan Coverage
| Boundary | Coverage |
|---|---|
| Inferior extent | Aortic arch / origin of great vessels (below aortic arch) |
| Superior extent | Vertex of skull / mid-orbits (2 cm above sella turcica) |
Full coverage includes:
- Aortic arch and origin of subclavian/brachiocephalic arteries
- Common carotid arteries
- Carotid bifurcation (most important area)
- Internal and external carotid arteries (cervical course)
- Vertebral arteries (origin to skull base)
- Circle of Willis and intracranial vessels
- Up to vertex
"CTA and CEMRA both allow a full assessment of the arterial tree from the aortic arch to the circle of Willis and beyond." - Grainger & Allison's Diagnostic Radiology
Scan Direction
Craniocaudal (head to foot) is inferior to superior - IMPORTANT:
- Scan direction should be inferior to superior (craniocaudal approach going from aortic arch upward)
- This follows the direction of contrast flow from heart → carotid arteries → brain
- Scanning in the direction of blood flow ensures contrast is present in each vessel segment as the scanner reaches it
- Some institutions use craniocaudal (top to bottom) to reduce perivenous streak artifact from contrast in the subclavian/brachiocephalic vein - this is an alternative validated approach
Contrast Protocol
| Parameter | Value |
|---|---|
| Contrast agent | Non-ionic iso-osmolar or low-osmolar iodinated contrast (e.g., Omnipaque 350, Isovue 370, Iohexol) |
| Volume (adult) | 80-135 mL (institutions vary: OHSU uses 50 mL at high flow; most protocols use 80-120 mL; ACR minimum 4 mL/sec in patients ≥50 kg) |
| Injection rate | 4-5 mL/sec minimum (up to 6 mL/sec in larger patients); higher flow rate = sharper bolus = better arterial enhancement |
| Saline chaser | 30-50 mL saline flush at same rate immediately after contrast - reduces total contrast volume needed and pushes contrast bolus through venous system |
| Pediatric dosing | Weight-based; scale injection rate proportionally; use right arm access |
Bolus Timing - Bolus Tracking (Preferred Method)
Automatic triggering (SmartPrep / CARE Bolus / Sure-Start) is the standard:
- Place ROI (region of interest) in the ascending aorta or aortic arch
- Run low-dose monitoring scans every 1 second starting 5 seconds after contrast injection begins (monitoring at 100 kVp, 20-40 mAs)
- Trigger threshold: 100-150 HU above baseline in the aorta
- When threshold is reached, scanner automatically initiates the CTA acquisition (with a typical 5-8 second delay for table/gantry prep + patient instruction)
Alternative - Test Bolus:
- Inject 10-15 mL test bolus at same flow rate
- Serial low-dose scans at the aortic arch level every 1-2 seconds
- Measure time to peak enhancement → use as fixed scan delay for full bolus
Pre-Contrast Phase
A non-contrast series may be obtained first when:
- Suspected mural hemorrhage (dissection - intramural hematoma appears bright pre-contrast)
- Mapping calcification for stenosis assessment
- Localizing anatomy
Section thickness for non-contrast: same as CTA or ≤5 mm (ACR-ASNR).
Reconstructions / Post-Processing
After raw acquisition, the following reformats are generated:
| Reconstruction | Detail |
|---|---|
| Axial source images | 1 mm thickness, reviewed first - most important for stenosis measurement |
| Sagittal reformats | 1 mm |
| Coronal reformats | 1 mm |
| Sagittal MIP (Maximum Intensity Projection) | 3 mm slabs - shows vessel course and stenosis |
| Coronal MIP | 3 mm slabs |
| 3D Volume Rendering (VR) | Overall vascular anatomy, surgical planning, patient communication |
| Curved planar reformations (CPR) | Straightens vessel for accurate stenosis length measurement |
| Bone subtraction | Software removes skull base/cervical spine to better visualize vessels |
Window settings for viewing: W400/L40 (standard soft tissue) for axial; adjust to W730/L310 for heavily calcified stenoses.
What the Radiologist Reports
- Degree of stenosis using NASCET criteria:
- Stenosis % = (1 - residual lumen diameter / normal distal ICA diameter) × 100
- Symptomatic: ≥70% stenosis = high benefit from CEA; 50-69% = moderate benefit
- Plaque morphology (calcified vs. soft/lipid-rich - juxtoluminal hypodensity = unstable plaque)
- Occlusion vs. near-occlusion ("trickle flow")
- Tandem lesions (intracranial + extracranial disease)
- Carotid bulb/ICA anatomy, tortuosity, kinks, coils
- Aortic arch type and variant origin of vessels (surgical planning)
- Vertebral artery dominance/patency
- Circle of Willis completeness
CTA vs. Other Modalities for Carotid Stenosis
| Modality | Sensitivity | Specificity | Key Notes |
|---|---|---|---|
| CTA | 97% | 99% | No flow artifacts; shows calcification well; radiation + contrast |
| Duplex US | ~90% | ~90% | First-line, operator-dependent; cannot assess arch |
| CE-MRA | 94% | 93% | No radiation; may overestimate stenosis; can miss calcification |
| DSA (catheter) | Gold standard | Gold standard | Invasive; 1% stroke risk; required before carotid stenting |
- Fischer's Mastery of Surgery, Grainger & Allison's Diagnostic Radiology
Example CTA Carotid Image
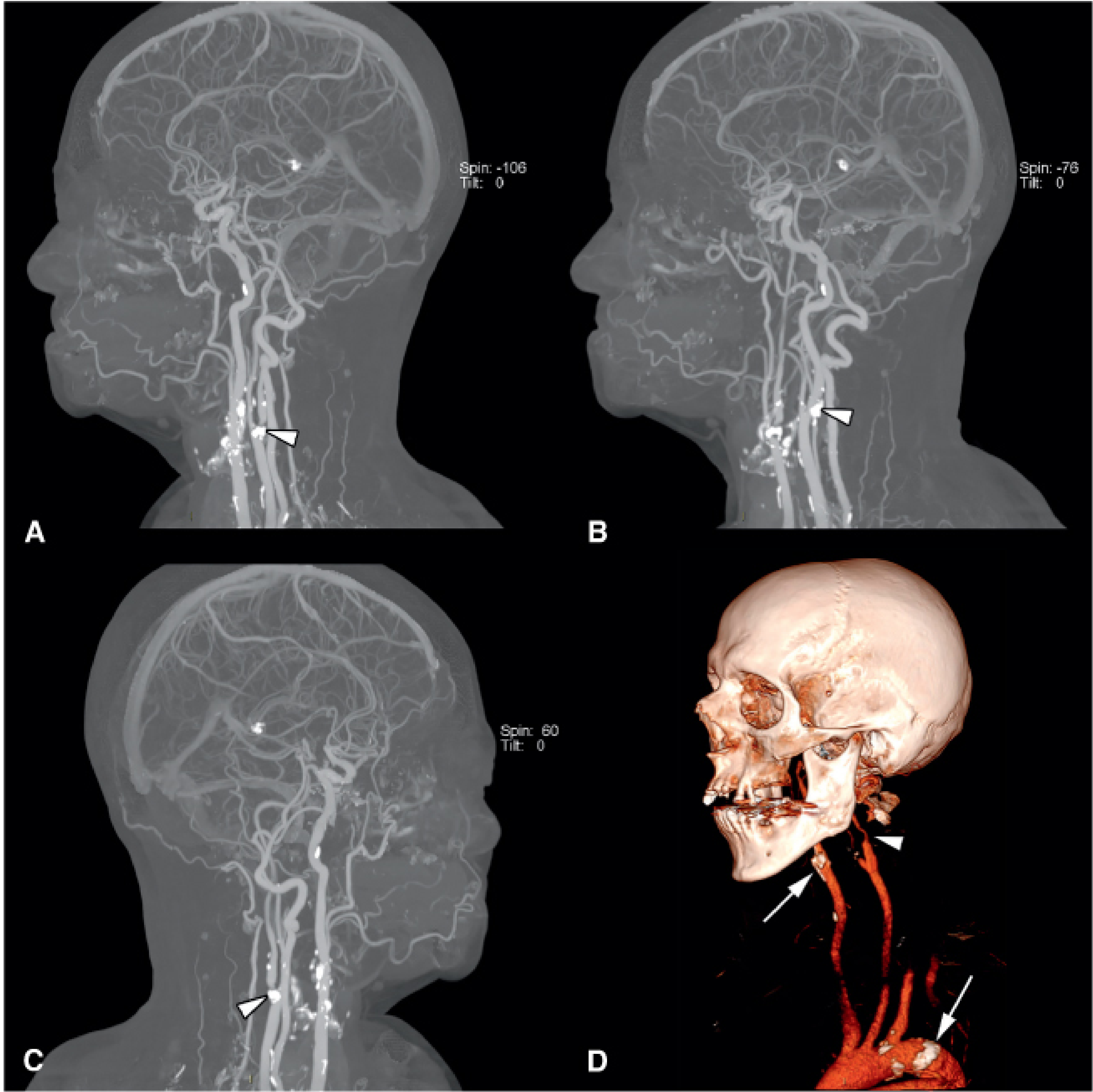
CTA head and neck with 3D vessel reconstruction. Arrowheads show carotid bifurcation calcification; the right image (D) shows a 3D bone-subtracted volume rendering with approximately 90% stenosis of the left ICA. - Fischer's Mastery of Surgery
Key Tips and Pitfalls
| Issue | Solution |
|---|---|
| Venous contamination (left brachiocephalic vein streak) | Use right arm injection; consider craniocaudal scan direction |
| Heavy calcification | Adjust window width; use CTA source images (not MIP) to measure true lumen |
| Arterial-venous overlap | Optimize timing with bolus tracking; avoid late acquisition |
| Motion artifact (swallowing) | Instruct patient not to swallow during scan; short scan time helps |
| Contrast nephropathy | Screen creatinine; hydrate; use minimum effective contrast volume |
| Near-occlusion | CTA source images + MIP together; arterial + slightly delayed phase discriminate occlusion from trickle flow |
This is a shared conversation. Sign in to Orris to start your own chat.