Anatomy and embryology of parathyroid gland. MS ENT university exam pattern for 20 marks.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative ENT sources (Cummings, Bailey & Love, Scott-Brown's). Let me compile the full 20-mark MS ENT university exam answer.
Anatomy and Embryology of the Parathyroid Gland
(MS ENT University Exam - 20 Marks)
INTRODUCTION (1 mark)
The parathyroid glands are small endocrine glands located posterior to the thyroid. Their developmental embryology and surgical anatomy are intimately linked - a thorough understanding of both is essential for the successful surgical treatment of parathyroid disease. They were first described by Sir Richard Owen in 1852 during dissection of an Indian rhinoceros, and subsequently in humans by Ivar Sandstrom in 1880, who named them "glandulae parathyreoidae."
EMBRYOLOGY (6 marks)
Pharyngeal Pouch Origin
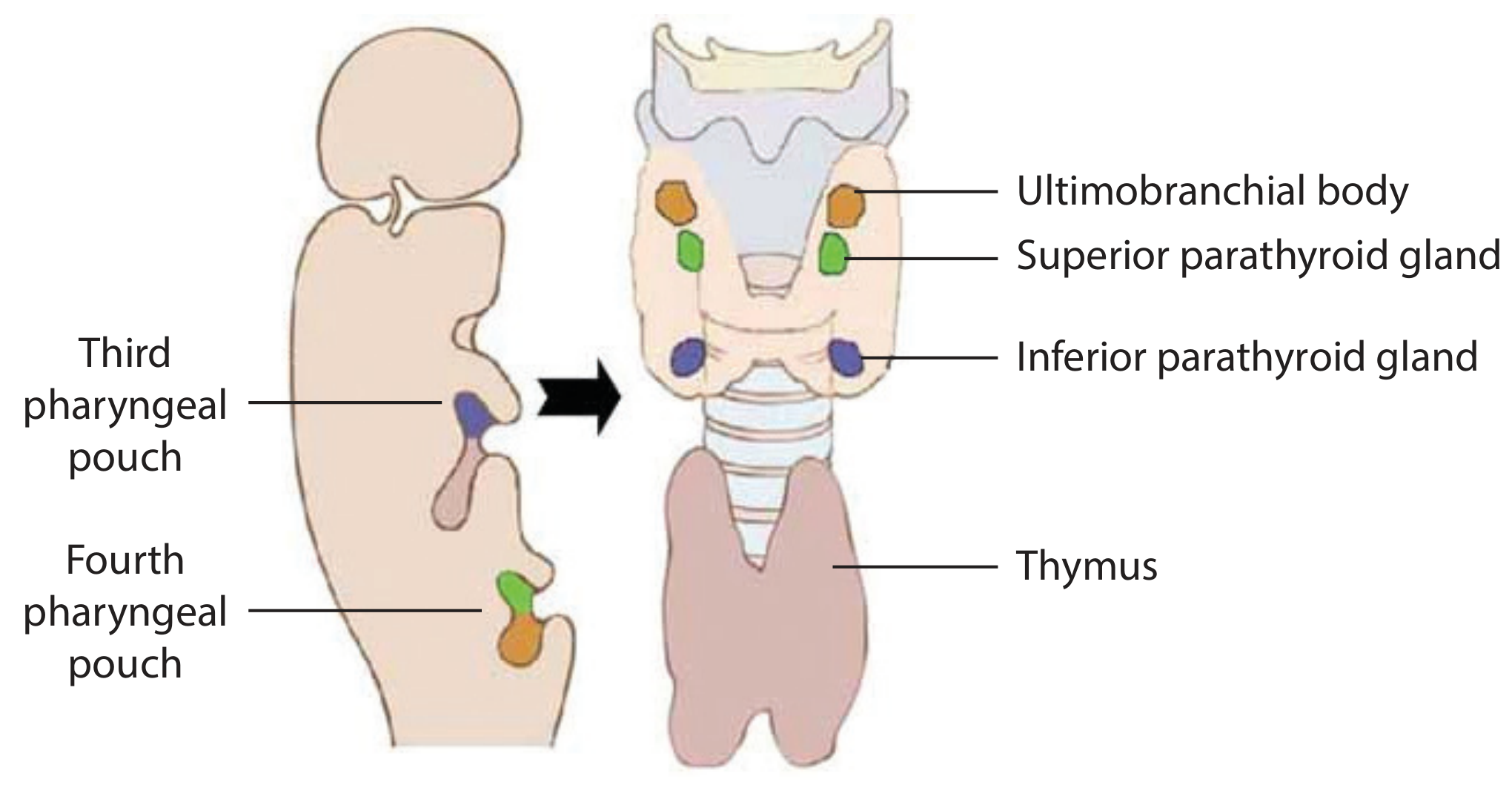
Fig. 1 - Diagram of normal pharyngeal organ development (Scott-Brown's Otolaryngology, Vol 1)
The parathyroid glands develop from the 3rd and 4th pharyngeal pouches between the 5th and 12th weeks of gestation. Development begins in the 5th week and descent to join the thyroid is complete by approximately the 7th week.
| Gland | Pouch of Origin | Companion Structure |
|---|---|---|
| Inferior parathyroid (PIII) | 3rd pharyngeal pouch (dorsal wing) | Thymus (from ventral wing of 3rd pouch) |
| Superior parathyroid (PIV) | 4th pharyngeal pouch (dorsal wing) | Ultimobranchial body |
Key paradox (important exam point): The inferior parathyroid glands arise from the superiorly positioned 3rd pharyngeal pouch, while the superior parathyroids arise from the inferiorly positioned 4th pharyngeal pouch. The inferior glands travel a longer distance (with the thymus), so end up below - hence the name "inferior" despite arising from a higher pouch.
Migration of Inferior Parathyroid (PIII)
- The inferior glands migrate caudally alongside the thymus as it descends into the thorax
- The inferior parathyroid normally detaches from the thymus and settles at the lower pole of the thyroid
- If it fails to detach, it may descend further into the mediastinum - a common source of ectopic parathyroid
- Due to this longer migratory path, inferior glands are more variable in final position
Migration of Superior Parathyroid (PIV)
- The superior glands have a shorter, more predictable migratory path
- They remain in close relation to the posterior surface of the upper thyroid lobe
- Consequently, they are more constant in anatomical position (>80% in a predictable 2 cm zone)
Clinical Significance of Embryology
Ectopic glands arise from aberrant migration. The most common ectopic locations for inferior glands (in order of frequency): intrathymic/mediastinal, carotid sheath, retroesophageal, and even the submandibular region. Superior glands, if ectopic, descend into the tracheoesophageal groove or retroesophageal space.
GROSS ANATOMY (5 marks)
Number and General Features
- Usually four in number (two superior, two inferior), but supernumerary glands occur in ~5% of the population
- ~13% of people have some abnormality in parathyroid tissue configuration
- Shape: Oval or lenticular ("Portland brick" shaped)
- Size: 5 × 3 × 1 mm
- Weight: ~30 mg each (combined ~120-140 mg total)
- Colour: Yellow-brown (similar color to fat; described as "Portland brick" color)
- Each gland lies within a halo of fat and is freely mobile over the thyroid capsule - this distinguishes parathyroid glands from thyroid nodules, which cannot move freely
Position of Superior Parathyroid Glands
- Located at the posterior aspect of the thyroid lobe, in an area 2 cm in diameter
- Centered ~1 cm around the junction of the inferior thyroid artery and the recurrent laryngeal nerve (RLN), close to the cricothyroid junction
- Position is dorsal (deep) to the coronal plane of the RLN
- Covered by pretracheal fascia that envelopes the thyroid and connects to hypopharynx, esophagus, and carotid sheath
- Lies at the level of the cricothyroid junction / upper 2/3 of thyroid lobe
Position of Inferior Parathyroid Glands
- More variable in position (due to longer embryological migration)
- In >50% of cases: at the inferior pole of the thyroid gland (anterior, lateral, or posterior surface)
- Position is ventral (superficial) to the coronal plane of the RLN
- Located ~2.5 cm below the intersection of RLN and inferior thyroid artery
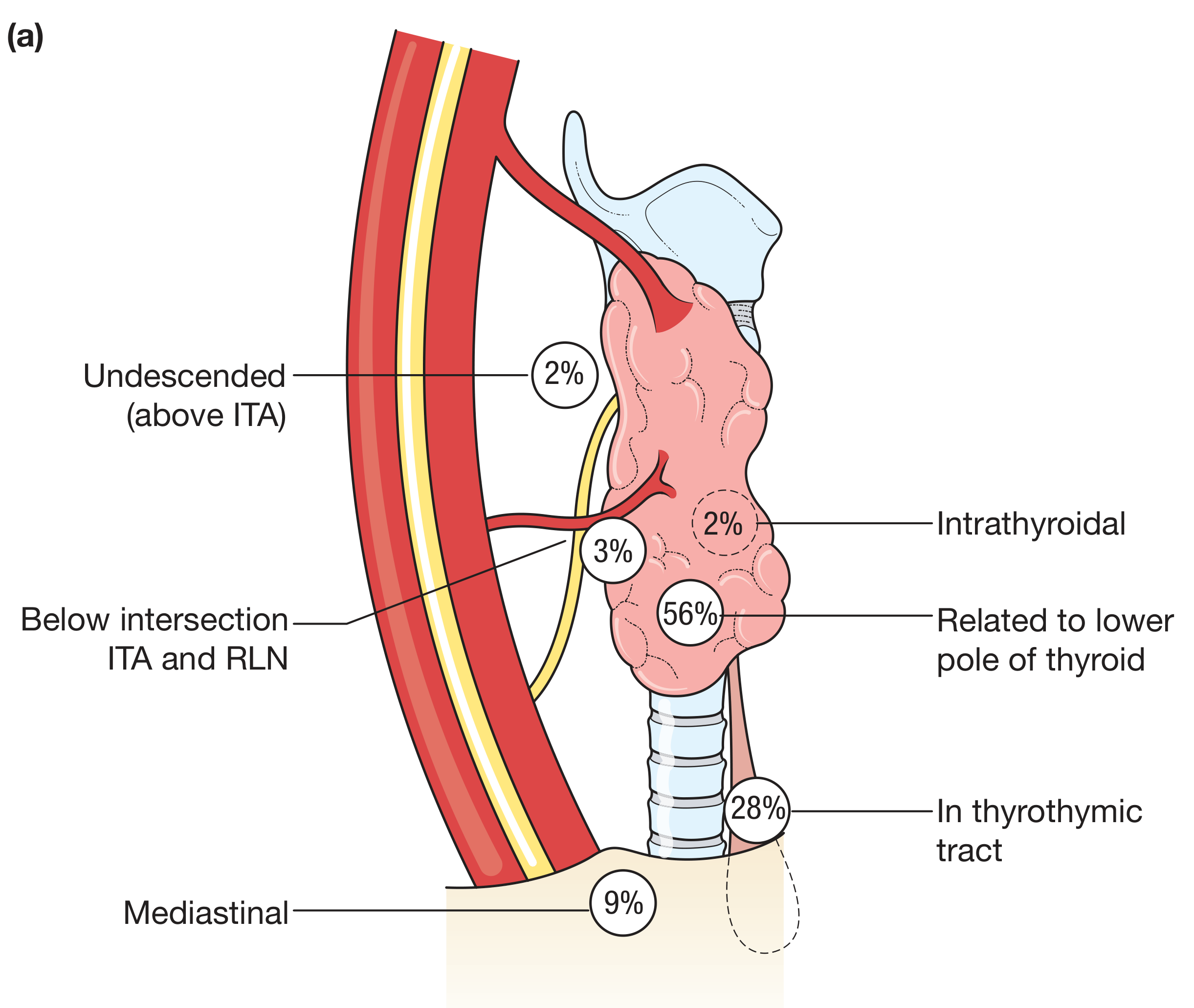
Fig. 2 - Distribution of inferior parathyroid gland positions (Bailey & Love, 28th Ed.) - 56% at lower thyroid pole, 28% in thyrothymic tract, 9% mediastinal, 2-3% intrathyroidal/undescended
Relationship to Recurrent Laryngeal Nerve (RLN)
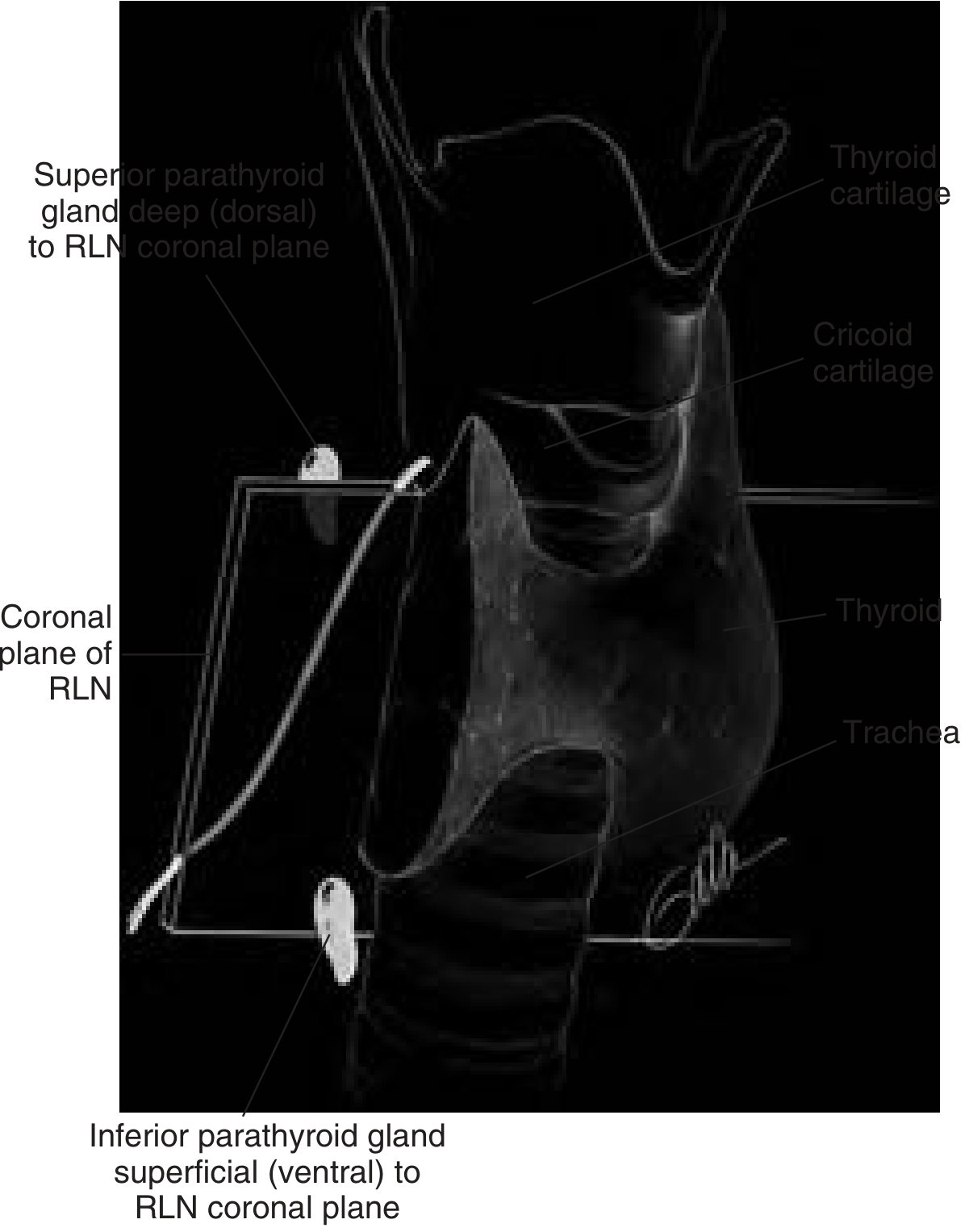
Fig. 3 - Superior glands are dorsal (deep) and inferior glands are ventral (superficial) to the coronal plane of the RLN (Cummings Otolaryngology)
This RLN relationship is the most important surgical landmark:
- Superior PTG - dorsal/posterior to RLN
- Inferior PTG - ventral/anterior to RLN
ECTOPIC POSITIONS (2 marks)
Inferior Parathyroid Ectopia (more common)
| Position | Percentage |
|---|---|
| Related to lower pole of thyroid | 56% |
| In thyrothymic tract / thyrothymic ligament | 28% |
| True mediastinal (within thymus) | 9% |
| Intrathyroidal | 2% |
| Undescended (above inferior thyroid artery) | 2% |
| Carotid sheath, retroesophageal, submandibular | Rare |
- As many as 28% of inferior glands are found within the thymus or thyrothymic ligament
- Intrathyroidal glands are reported in 1-3% and are more common with superior glands
Superior Parathyroid Ectopia (less common)
- Retroesophageal or paraesophageal space (most common ectopic site when enlarged)
- May descend into tracheoesophageal groove at or below mid/inferior thyroid pole
- Color similar to esophagus - non-bloody field essential for identification
BLOOD SUPPLY (2 marks)
Arterial Supply
- Both superior and inferior parathyroid glands are supplied by the inferior thyroid artery, which arises from the thyrocervical trunk
- Abundant anastomoses also exist with:
- Superior thyroid artery
- Laryngeal arteries
- Pharyngeal arteries
- Esophageal arteries
- Tracheal arteries
- 10% of inferior glands derive their dominant arterial supply from a branch of the superior thyroid artery
- These anastomoses explain why ligation of the inferior thyroid artery during thyroid surgery does not always compromise parathyroid blood supply
Clinical Note - Hypoparathyroidism after Thyroidectomy
Transient hypoparathyroidism from ischemia occurs in up to 20% of patients after total thyroidectomy; it usually resolves in a few weeks.
Venous and Lymphatic Drainage
- Venous drainage via the thyroid venous plexus into the internal jugular veins
- Lymphatics drain to the deep cervical nodes and mediastinal nodes
HISTOLOGY (2 marks)
The parathyroid gland is covered by a thin fibrous capsule with internal septa. The parenchymal cells are arranged in nests and cords within a rich capillary network.
Cell Types
| Cell Type | Features | Function |
|---|---|---|
| Chief cells | Small, pale cytoplasm, most numerous | Secrete PTH |
| Oxyphil cells | Larger, eosinophilic, fewer in number, more mitochondria | Function uncertain; uptake Tc-99m sestamibi (used in scanning) |
| Water clear cells | Clear vacuolated cytoplasm | Variant |
| Fat cells | Increase with age | Stromal cells |
- Chief cells are the major parenchymal cells and the primary source of PTH
- Oxyphil cells are fewer and larger, with abundant mitochondria - they concentrate technetium-99m more than other tissues, forming the basis of sestamibi scanning
- Fat content of normal gland increases with age (~50% fat in adults)
NERVE SUPPLY (1 mark)
- Derived from the cervical sympathetic ganglia (vasomotor function only)
- The parathyroid glands have no secretomotor nerve supply - PTH secretion is regulated entirely by serum calcium levels via calcium-sensing receptors (CaSR)
APPLIED ANATOMY / SURGICAL SIGNIFICANCE (1 mark)
- Bilateral neck exploration - knowledge of anatomy guides the surgeon to find all four glands and prevent inadvertent devascularization
- RLN landmark - the plane of the RLN separates superior (dorsal) from inferior (ventral) glands
- Inferior thyroid artery - key surgical landmark; superior PTG is 2.5 cm above and inferior PTG is 2.5 cm below its intersection with the RLN
- Pretracheal fascia relationship - superior glands can "move freely" under this fascia; this mobility distinguishes them from fixed thyroid nodules
- Missing gland protocol - if a gland is not found in its expected location, knowledge of ectopic sites from embryology (mediastinum, carotid sheath, retroesophageal, submandibular) directs further search
- Symmetry - there is a degree of bilateral symmetry in parathyroid position; if one side is difficult, finding the gland on the opposite side first helps guide exploration
SUMMARY TABLE
| Feature | Superior PTG | Inferior PTG |
|---|---|---|
| Embryological origin | 4th pharyngeal pouch | 3rd pharyngeal pouch |
| Companion structure | Ultimobranchial body | Thymus |
| Migration distance | Short | Long |
| Position consistency | High (>80% in 2 cm zone) | Variable |
| Normal position | Posterior thyroid, near cricothyroid junction | Lower pole of thyroid |
| Relation to RLN | Dorsal (deep) | Ventral (superficial) |
| Common ectopic site | Retroesophageal, TEG | Mediastinum, thyrothymic tract |
Sources:
- Cummings Otolaryngology Head & Neck Surgery, Chapter 123
- Bailey and Love's Short Practice of Surgery, 28th Ed., Chapter 56
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1, Chapter 77
- Schwartz's Principles of Surgery, 11th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.