O2 dissosiation curve short notes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I have excellent content and two high-quality diagrams. Let me now compile the comprehensive short notes.
O₂ Dissociation Curve - Short Notes
Definition
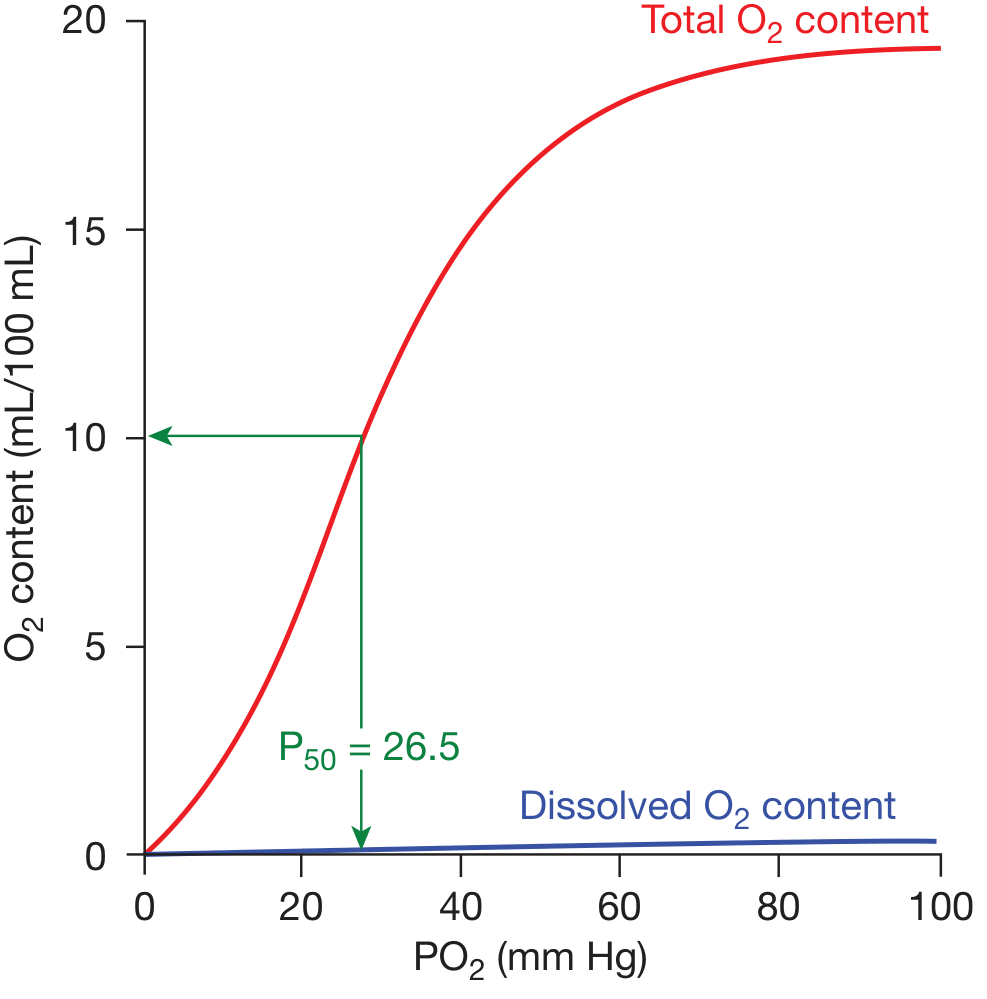
The oxygen dissociation curve (ODC) represents the relationship between the partial pressure of oxygen (PO₂) and the percentage saturation of hemoglobin (Hb) with oxygen. It describes how readily hemoglobin picks up or releases O₂ under different physiological conditions.
Shape of the Curve
The ODC is sigmoid (S-shaped), not hyperbolic. This shape arises from the cooperative binding of O₂ to hemoglobin's four subunits:
- Binding of O₂ to one heme group causes a conformational change (T-form → R-form) that increases the affinity of the remaining heme groups for O₂.
- The net result: affinity for the last O₂ bound is ~300× greater than for the first.
- In contrast, myoglobin (monomeric) has a hyperbolic curve and maximum affinity throughout - it cannot efficiently deliver O₂ to tissues.
(Lippincott Illustrated Reviews Biochemistry, 8th ed)
Standard Conditions
The curve is plotted at: pH 7.40, temperature 37°C, atmospheric pressure 760 mmHg.
| Point on curve | PO₂ (mmHg) | SpO₂ (%) | Notes |
|---|---|---|---|
| Lung (arterial) | 95-100 | ~97% | Hb nearly fully saturated |
| Mixed venous (rest) | ~40 | ~75% | Only 25% O₂ extracted at rest |
| P₅₀ (half-saturation) | 26.5 | 50% | Standard reference point |
(Fishman's Pulmonary Diseases and Disorders)
Physiological Significance of the S-Shape
Upper flat portion (PO₂ 60-100 mmHg):
- Hb remains highly saturated even when arterial PO₂ drops (e.g., lung disease, altitude).
- As long as PO₂ ≥ 60 mmHg, O₂ content stays near-normal - this is the "safety plateau."
Steep middle portion (PO₂ 20-60 mmHg):
- Small drops in PO₂ release large amounts of O₂ to tissues.
- This facilitates efficient O₂ unloading at the tissue capillary level.
Shifts of the ODC
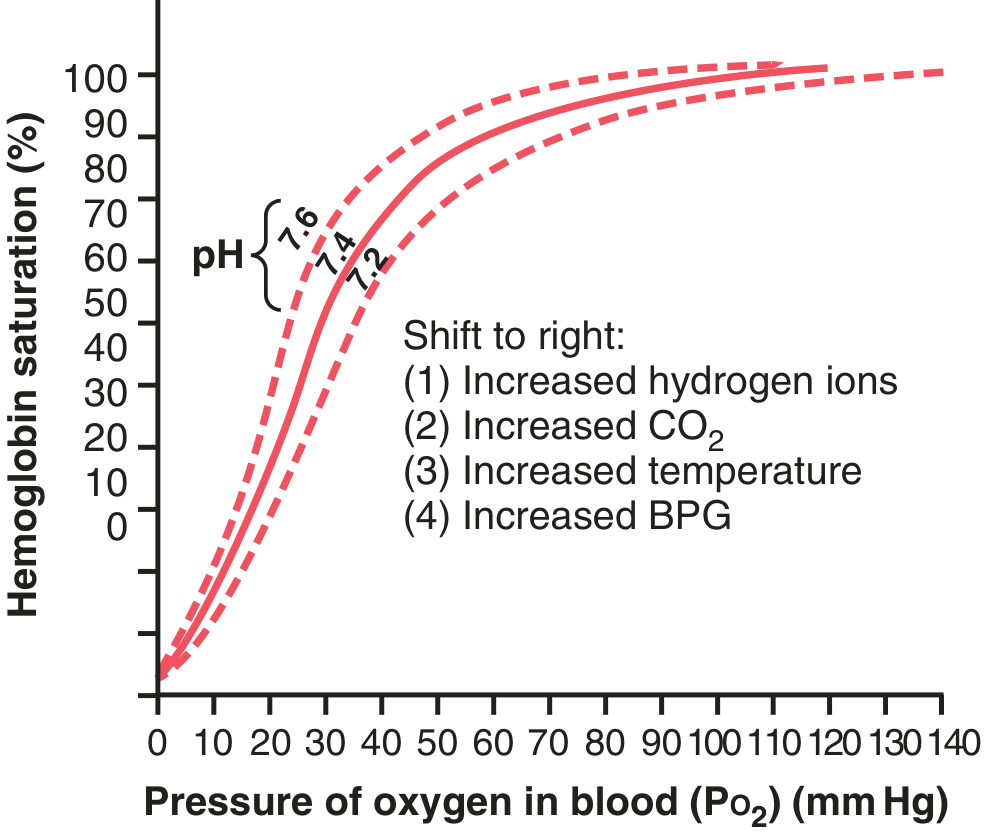
Right Shift (↑ P₅₀, decreased O₂ affinity → more O₂ released to tissues)
| Cause | Mechanism |
|---|---|
| ↑ H⁺ (↓ pH) | Bohr effect - protonation stabilizes deoxy-Hb |
| ↑ CO₂ | Direct + via H⁺ production |
| ↑ Temperature | Favors T-form (deoxy) |
| ↑ 2,3-BPG | Binds deoxy-Hb, lowers O₂ affinity |
Mnemonic: CADET - CO₂, Acidosis (↓pH), DPG (2,3-BPG), Exercise, Temperature↑
Right shift is adaptive in: exercise, fever, anemia, high altitude (chronic), hypoxia.
Left Shift (↓ P₅₀, increased O₂ affinity → Hb holds O₂ tighter, less released)
| Cause | Notes |
|---|---|
| ↓ H⁺ (↑ pH / alkalosis) | Stabilizes oxy-Hb (R-form) |
| ↓ CO₂ | e.g., hyperventilation |
| ↓ Temperature | Hypothermia |
| ↓ 2,3-BPG | Stored blood |
| Fetal Hb (HbF) | HbF binds 2,3-BPG poorly → left shift → picks up O₂ from maternal Hb |
| CO poisoning | Carboxyhemoglobin - high affinity, no O₂ release |
| Methemoglobin | Fe³⁺ form, cannot carry O₂ |
(Guyton & Hall, Lippincott Biochemistry)
The Bohr Effect
When tissues metabolize actively:
- CO₂ diffuses into blood → forms H₂CO₃ → releases H⁺
- ↑ H⁺ protonates histidine residues on Hb → forms salt bridges → stabilizes deoxy-Hb (T-form)
- Reaction: HbO₂ + H⁺ ⇌ HbH + O₂
In the lungs, the reverse occurs: CO₂ diffuses out, pH rises, curve shifts left → facilitates O₂ loading.
This differential is a key physiological mechanism for matching O₂ delivery to metabolic demand.
2,3-BPG (Bisphosphoglycerate)
- Synthesized from 3-phosphoglycerate in the Rapoport-Luebering shunt (a side pathway of glycolysis in RBCs).
- Binds to the central cavity of deoxy-Hb (between the β-subunits), stabilizing the T-form.
- Normal 2,3-BPG keeps the curve shifted slightly right (P₅₀ ~26.5 vs 19 mmHg in its absence).
- Chronic hypoxia → ↑ 2,3-BPG synthesis → further right shift → improves O₂ delivery.
- Stored blood (bank blood): 2,3-BPG depletes within days → left shift → impaired O₂ release.
(Guyton & Hall; Lippincott Biochemistry, 8th ed)
Special Situations
| Condition | Shift | Reason |
|---|---|---|
| High altitude (acute) | Right (mild) | ↑ ventilation → ↑ CO₂ expiration → left initially, but ↑ 2,3-BPG later |
| High altitude (chronic) | Right | ↑ 2,3-BPG predominates |
| Exercise | Right | ↑ CO₂, ↑ H⁺, ↑ temperature, ↑ 2,3-BPG |
| Fetal circulation | Left (HbF) | HbF has γ-chains instead of β → binds 2,3-BPG poorly |
| Carbon monoxide poisoning | Left | CO binds Hb 250× more avidly than O₂ |
| Hypothyroidism/hypothermia | Left | Reduced metabolism |
Key Values to Remember
- P₅₀ (normal): 26.5 mmHg
- At PO₂ = 100 mmHg (arterial): ~97% saturation
- At PO₂ = 40 mmHg (venous rest): ~75% saturation
- At PO₂ = 60 mmHg: ~90% saturation (the critical threshold - below this, saturation drops sharply)
- Each gram of Hb can carry 1.34 mL O₂ when fully saturated (Hüfner's constant)
Summary Table: Factors Affecting ODC
| Factor | Right Shift (↑P₅₀) | Left Shift (↓P₅₀) |
|---|---|---|
| pH | ↓ pH (acidosis) | ↑ pH (alkalosis) |
| CO₂ | ↑ PaCO₂ | ↓ PaCO₂ |
| Temperature | ↑ Temp | ↓ Temp |
| 2,3-BPG | ↑ 2,3-BPG | ↓ 2,3-BPG |
| Hb type | Adult HbA | Fetal HbF, HbH, CO-Hb |
Sources: Fishman's Pulmonary Diseases and Disorders | Guyton & Hall Medical Physiology | Lippincott Illustrated Reviews Biochemistry, 8th ed
Refered pain very short notes easy word
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have all the content and diagrams needed. Here are the short notes:
Referred Pain - Short Notes
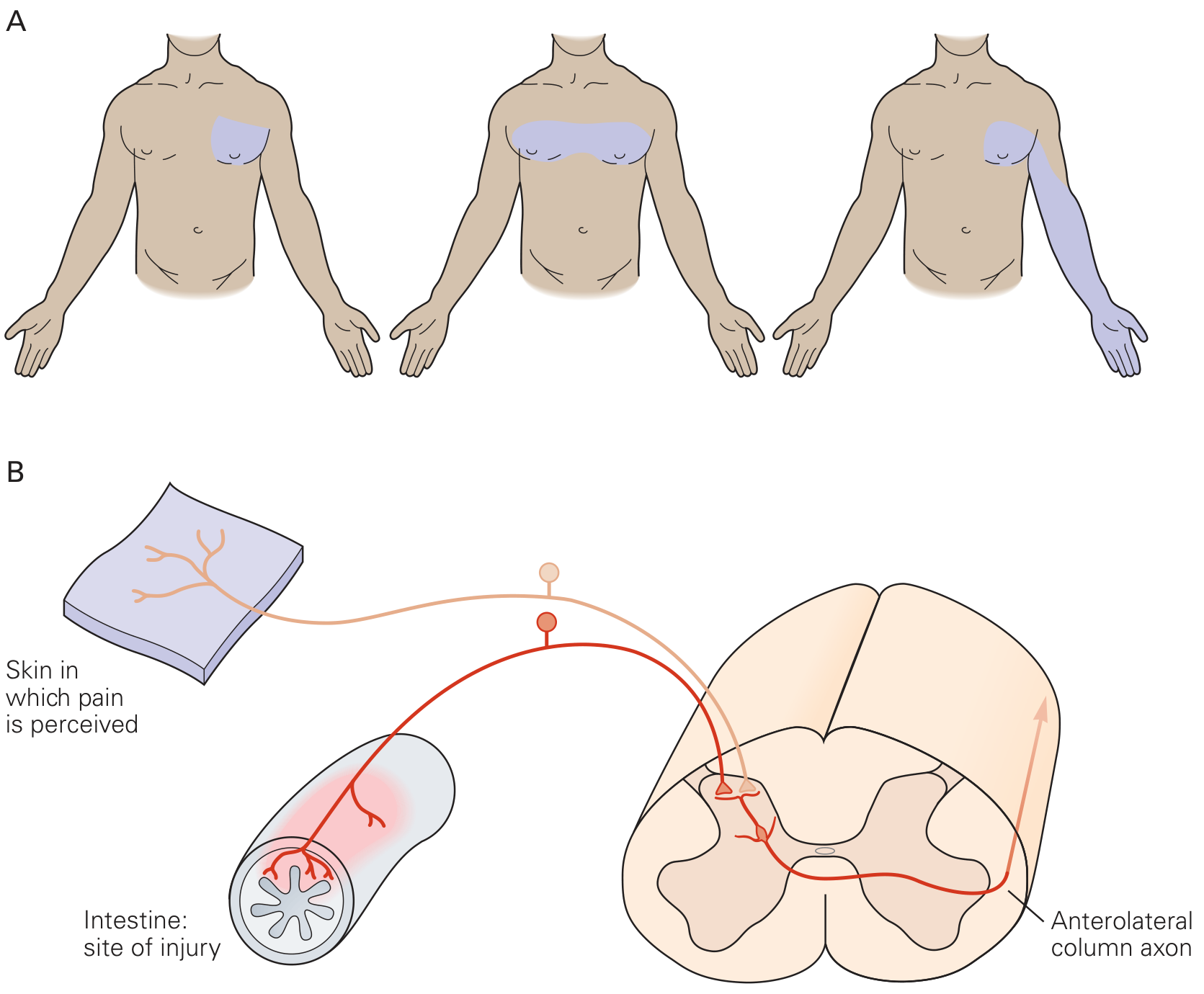
What is it?
Pain felt at a place far from where the actual problem is.
Example: Heart attack → pain felt in left arm and jaw (not just the chest).
Why does it happen? (Mechanism)
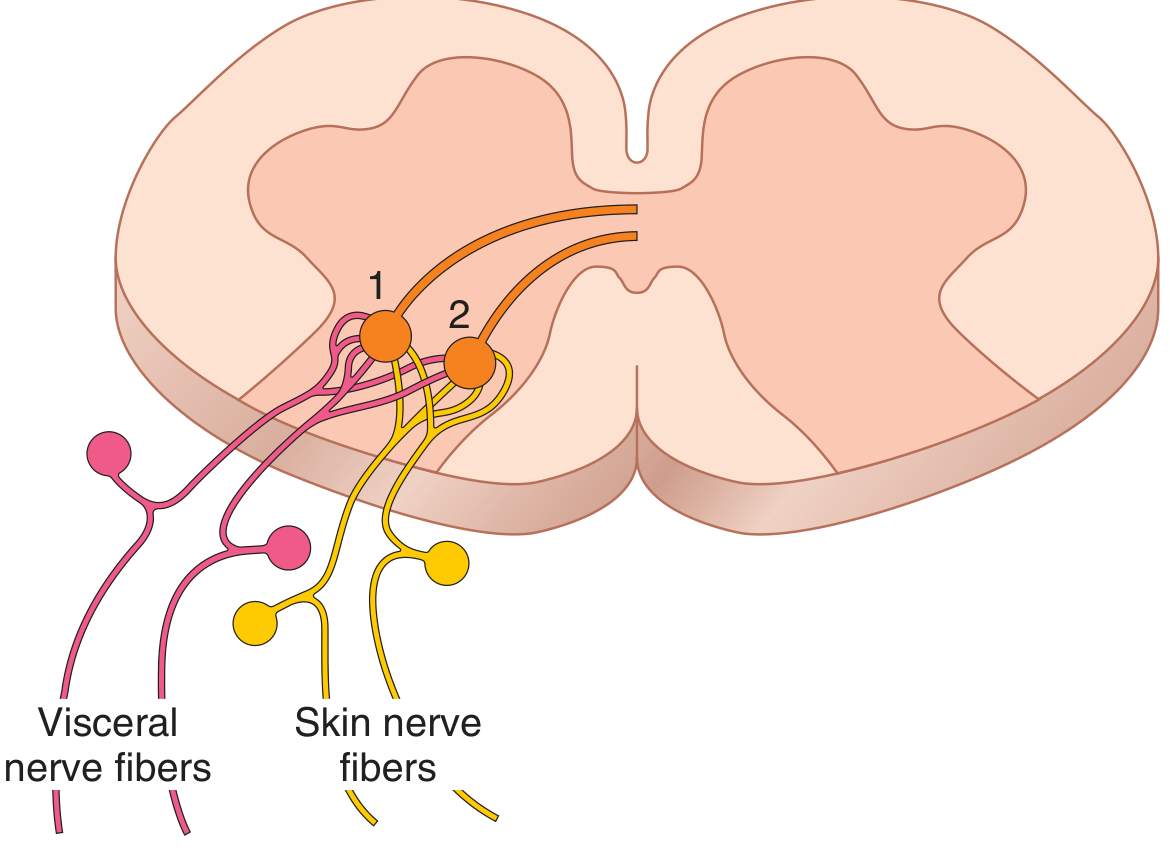
Convergence Theory - the most accepted explanation:
- Visceral (organ) pain fibers and skin pain fibers share the same second-order neurons in the spinal cord dorsal horn.
- The brain cannot tell where the pain really came from - it assumes the pain is from the skin (because skin sends pain signals more often than organs).
- So organ pain gets misread as skin pain at the same spinal level.
(Guyton & Hall Medical Physiology)
(Kandel - Principles of Neural Science, 6th ed)
Simple Rule
Pain is referred from organ (visceral) → to skin (somatic) at the same spinal cord level
Classic Examples (Must Know)
| Organ with Problem | Where Pain is Felt |
|---|---|
| Heart (MI / Angina) | Left arm, jaw, neck, chest |
| Diaphragm (irritation) | Tip of shoulder (C3-C5 via phrenic nerve) |
| Appendix (early) | Umbilical region (T10 dermatome) |
| Gallbladder | Right shoulder / right scapula |
| Kidney / Ureter stone | Groin / testis / inner thigh |
| Pancreas | Back (between shoulder blades) |
| Hip joint disease | Medial knee (via obturator nerve) |
Appendicitis - Classic Teaching Example
Early stage:
- Appendix inflames → visceral fibers → enter spinal cord at T10
- Pain felt at umbilicus (T10 dermatome)
- Pain is diffuse, colicky (comes and goes with peristalsis)
Late stage:
- Appendix touches parietal peritoneum in right iliac fossa
- Now somatic fibers activated → pain shifts to right lower quadrant
- Pain becomes constant and localized
(Gray's Anatomy for Students)
Key Points
- Referred pain is clinically very important - in many organ diseases, it may be the only sign
- Pain travels via slow C fibers (dull, aching type)
- The brain has no "map" for visceral pain, so it uses the skin map instead
- Hyperalgesia (extra sensitivity) can also be referred to the same skin area
Memory Aid
"GALL-HEART-APP-DIA-KID"
| Letter | Organ | Pain felt at |
|---|---|---|
| G | Gallbladder | Right shoulder |
| H | Heart | Left arm/jaw |
| A | Appendix (early) | Umbilicus |
| D | Diaphragm | Shoulder tip |
| K | Kidney/Ureter | Groin/testis |
Sources: Guyton & Hall Medical Physiology | Gray's Anatomy for Students | Kandel Principles of Neural Science, 6th ed
This is a shared conversation. Sign in to Orris to start your own chat.