Management of Hypovolemic shock taking reference from Bailey and Love surgery book
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from Bailey and Love's Surgery 28th Edition. Let me compile the full, detailed answer.
Management of Hypovolemic Shock
Bailey and Love's Short Practice of Surgery, 28th Edition
Definition
Shock is a systemic state of low tissue perfusion that is inadequate for normal cellular respiration. With insufficient delivery of oxygen and glucose, cells switch from aerobic to anaerobic metabolism. If perfusion is not restored in a timely fashion, cell death ensues.
Haemorrhagic/hypovolaemic shock specifically results from loss of circulating blood volume - either from haemorrhage or loss of plasma/fluid - leading to reduced venous return, reduced cardiac output, and tissue hypoperfusion.
Pathophysiology
Cellular Level
- Cells deprived of O2 switch to anaerobic metabolism, producing lactic acid instead of CO2
- Accumulation of lactic acid produces a systemic metabolic acidosis
- As intracellular glucose is exhausted, anaerobic respiration ceases
- Failure of Na+/K+ pumps occurs; intracellular lysosomes release autodigestive enzymes leading to cell lysis
- Intracellular potassium is released into the bloodstream (hyperkalaemia)
Microvascular Level
- Hypoxia and acidosis activate complement and prime leucocytes
- Generation of oxygen free radicals and cytokine release
- Capillary endothelial injury - the endothelium becomes "leaky", fluid escapes into tissues, worsening cellular hypoxia
- Further activation of immune and coagulation cascades
Systemic - Cardiovascular
- Decreased preload and afterload trigger a baroreceptor response
- Increased sympathetic activity and catecholamine release
- Results in tachycardia and systemic vasoconstriction (preserving cerebral and coronary perfusion)
Systemic - Respiratory
- Metabolic acidosis + increased sympathetic response = increased respiratory rate and minute ventilation
- CO2 is excreted more rapidly, producing a compensatory respiratory alkalosis
Systemic - Renal
- Decreased perfusion pressure leads to reduced glomerular filtration and oliguria
- The renin-angiotensin-aldosterone axis is stimulated, causing further vasoconstriction and sodium/water retention
Classification of Shock
Bailey and Love classifies hypovolaemic/haemorrhagic shock by clinical severity:
| Class | Features |
|---|---|
| Mild (Compensated) | Tachycardia, normal BP, cool peripheries, anxiety; compensatory mechanisms intact |
| Moderate | Tachycardia, hypotension, reduced capillary refill, oliguria; compensatory mechanisms struggling |
| Severe | Profound hypotension, cold/clammy/pale skin, confusion, markedly reduced urine output |
| Unresuscitatable | Refractory to resuscitation; physiological exhaustion with coagulopathy, acidosis, hypothermia ("lethal triad") |
Lethal Triad (Physiological Exhaustion)
Bailey and Love emphasises that repeated cycles of volume resuscitation during ongoing haemorrhage leads to:
- Profound coagulopathy
- Acidosis
- Hypothermia
This spirals to death. The priority is always haemorrhage control - not fluid resuscitation.
Haemorrhage: Revealed vs Concealed
- Revealed haemorrhage - obvious external bleeding (arterial wound, haematemesis)
- Concealed haemorrhage - blood contained within a body cavity; must be actively suspected and investigated
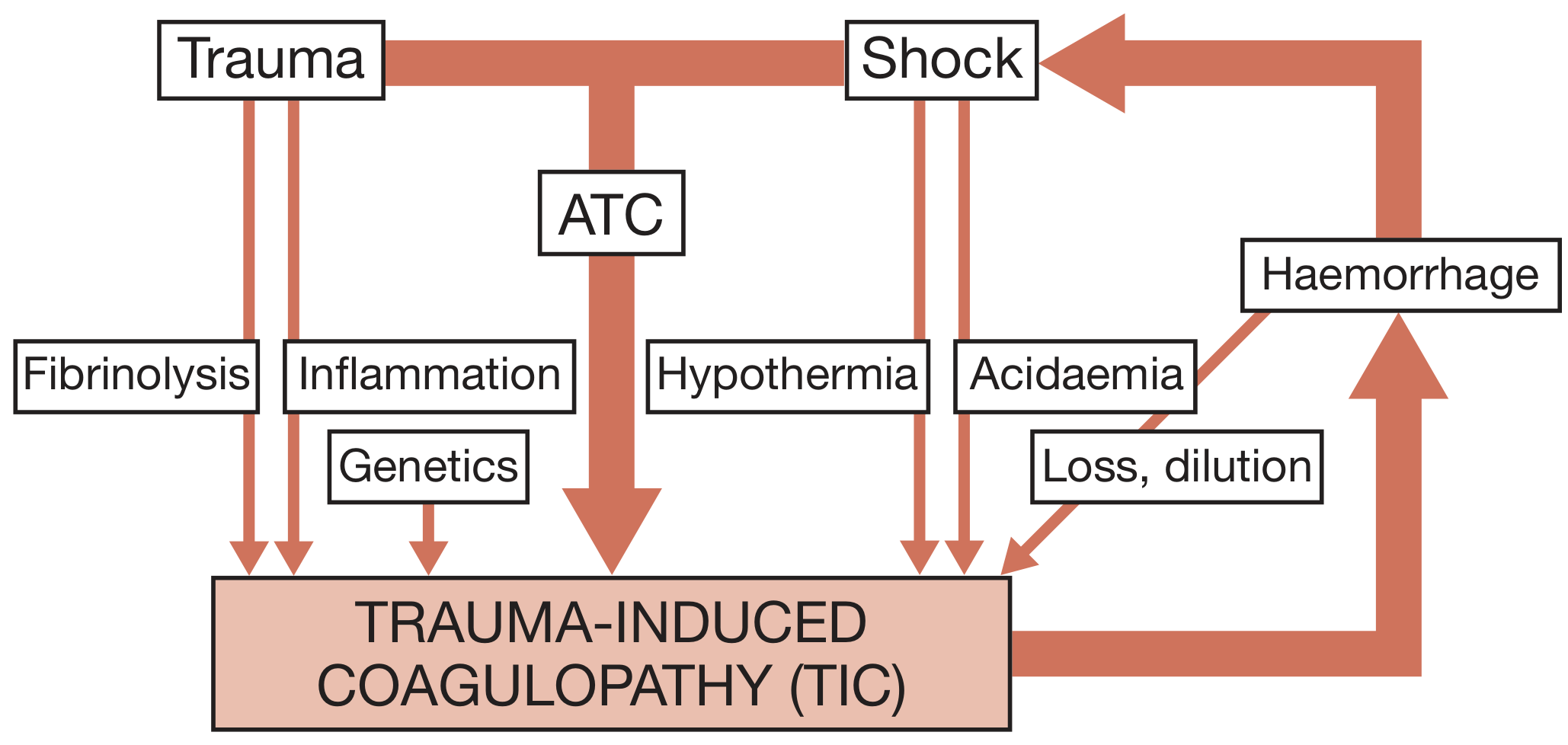
Acute Traumatic Coagulopathy (ATC)
Up to 25% of trauma patients develop ATC within minutes of injury - associated with a fourfold increase in mortality.
ATC is characterised by:
- Systemic hyperfibrinolysis
- Low fibrinogen levels
- Platelet dysfunction
ATC evolves into trauma-induced coagulopathy (TIC) due to further derangements:
- Fluid and RBC transfusions cause dilution of coagulation factors
- Hypothermia (worsened by cold fluids/blood) inhibits coagulation proteases
- Severe acidosis further impairs coagulation function
- These cause more bleeding - completing the downward spiral
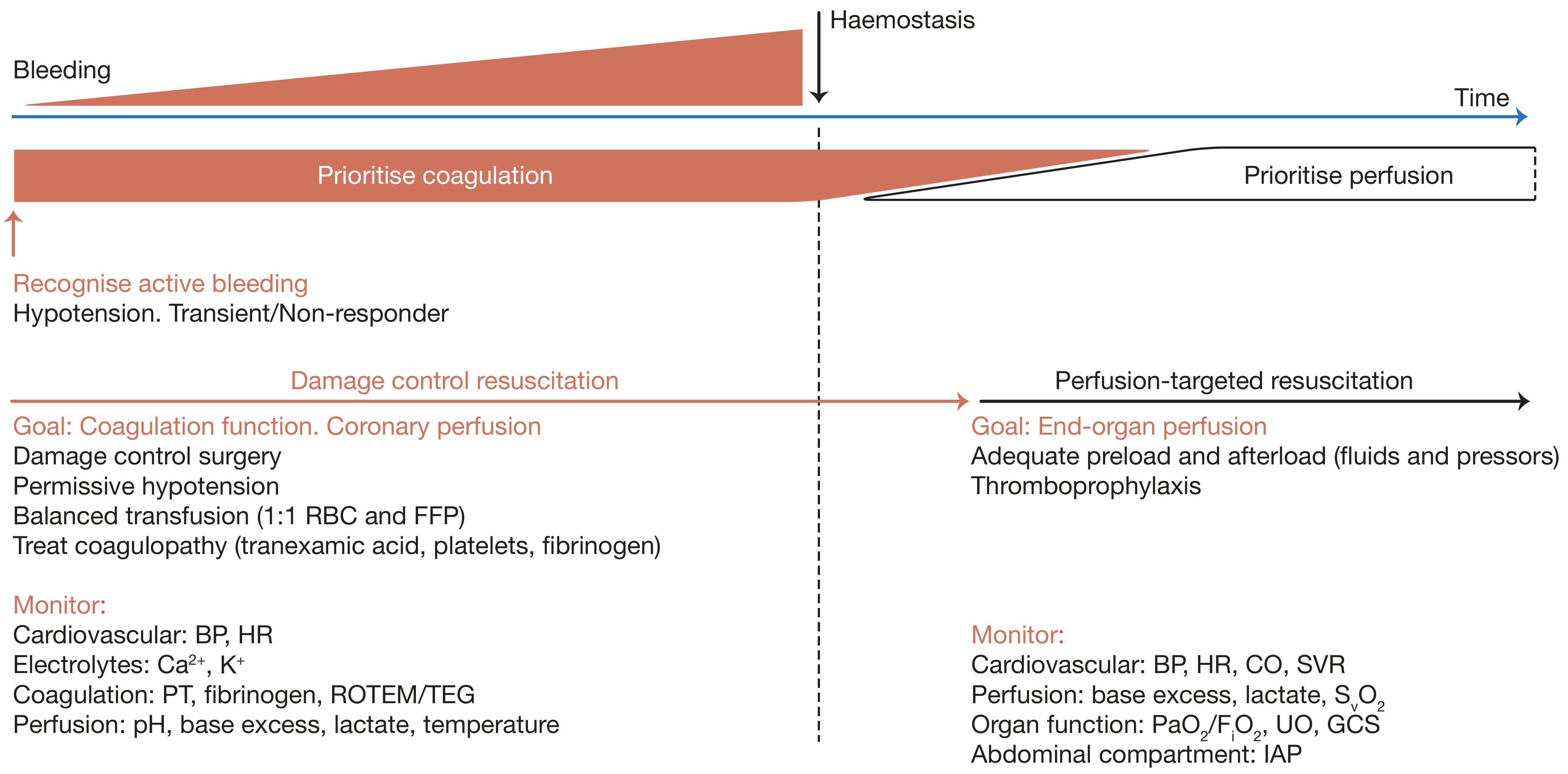
Management: Damage Control Resuscitation (DCR)
DCR is the modern strategy for haemorrhagic shock management. It applies while patients are bleeding and is based on four key principles:
1. Rapid Haemorrhage Control
- Direct pressure over external haemorrhage sites
- Tourniquets, balloon occlusion (e.g. REBOA) or other techniques for temporary control
- Intracavitary haemorrhage: rapid transfer to operating theatre or interventional radiology
- Damage control surgery (DCS): limit surgery to the minimum necessary - stop bleeding, control sepsis; avoid additional tissue damage and physiological stress
- Definitive repairs are delayed until the patient is haemodynamically stable
Summary of Damage Control Surgery:
- Damage control surgery limits operative intervention
- Life-threatening injuries take priority over reconstruction
- Restores physiology before definitive repair
- Used for penetrating, vascular and liver injuries
2. Permissive Hypotension
- During active haemorrhage, targeting a lower-than-normal blood pressure reduces ongoing blood loss
- Allows coronary perfusion without "popping the clot" at the bleeding site
- Bailey and Love stresses this is applied only while bleeding continues - not after haemostasis
3. Avoiding Dilutional Coagulopathy
- Restrict large volumes of crystalloid/colloid which dilute clotting factors
- Prefer blood products over crystalloids
- Balanced transfusion - 1:1 ratio of Red Blood Cells (RBC) to Fresh Frozen Plasma (FFP)
4. Treating Existing Coagulation Deficits
- Tranexamic acid - given early to prevent hyperfibrinolysis (ideally within 1 hour of injury; benefit diminishes after 3 hours)
- Platelets - transfused to correct platelet dysfunction
- Fibrinogen (cryoprecipitate or fibrinogen concentrate) - to correct low fibrinogen
- Coagulation guided by TEG (thromboelastography) or ROTEM (rotational thromboelastometry)
- Correct hypocalcaemia - calcium is essential for coagulation; massive transfusion depletes it
Post-Haemostasis: Perfusion-Targeted Resuscitation
Once haemorrhage is controlled, the strategy transitions from coagulation-focused to end-organ perfusion-focused:
- Adequate preload and afterload (fluids + vasopressors)
- Thromboprophylaxis
Fluid Resuscitation
Bailey and Love covers fluid selection in detail:
- Crystalloids (0.9% NaCl, Hartmann's): inexpensive, widely available, but large volumes cause dilutional coagulopathy, hyperchloraemic acidosis (with 0.9% saline), and pulmonary oedema
- Colloids (albumin, gelatins, starches): remain in the intravascular space longer, but synthetic starches (HES) are associated with renal failure and coagulopathy and are no longer recommended
- Blood products are the resuscitation fluid of choice in haemorrhagic shock - they replace lost blood directly
- 1:1 RBC:FFP balanced transfusion minimises dilutional coagulopathy
Massive Haemorrhage Protocol (MHP): Pre-defined ratios of blood products activated early in severe haemorrhage to deliver balanced transfusion rapidly.
Monitoring in Hypovolaemic Shock
Minimum Monitoring (Summary Box 2.4):
- ECG (continuous heart rate)
- Pulse oximetry
- Blood pressure (non-invasive, then arterial line if not correcting)
- Urine output (aim: 0.5-1 mL/kg/hr)
Additional Modalities:
- Central Venous Pressure (CVP) - assessed dynamically (not as a single value):
- Fluid bolus 250-500 mL over 5-10 min
- Normal response: CVP rises 2-5 cmH2O, drifts back over 10-20 min
- No CVP rise = patient needs more fluid
- Large, sustained CVP rise = volume overload or cardiac insufficiency
- Invasive arterial blood pressure
- Cardiac output monitoring (Doppler, pulse waveform analysis, indicator dilution) - helps distinguish shock types; pulmonary artery catheters are less common now
- Base deficit and serum lactate - best markers of adequacy of tissue perfusion and resuscitation endpoint
- During DCR: also monitor electrolytes (Ca2+, K+), PT, fibrinogen, ROTEM/TEG, pH, temperature
Special Considerations
Non-Haemorrhagic Hypovolaemia
Volume loss from other sources (vomiting, diarrhoea, burns, pancreatitis, bowel obstruction) requires fluid replacement targeted to the type of fluid lost (e.g. upper GI loss = Hartmann's or 0.9% NaCl with KCl supplementation).
Permissive Hypotension - When NOT to Use
Bailey and Love notes permissive hypotension is not appropriate in patients with head injuries, where maintaining cerebral perfusion pressure is mandatory (target MAP >80 mmHg in TBI).
Summary of Key Management Principles (Bailey and Love)
- Identify and control the source of haemorrhage FIRST - resuscitation is supportive, not definitive
- Avoid the lethal triad: coagulopathy, acidosis, hypothermia
- Apply Damage Control Resuscitation during active bleeding:
- Haemorrhage control (damage control surgery if needed)
- Permissive hypotension
- Avoid dilutional coagulopathy
- Treat coagulation deficits (tranexamic acid, platelets, fibrinogen, FFP)
- Use balanced 1:1 RBC:FFP transfusion
- Transition to perfusion-targeted resuscitation after haemostasis
- Monitor with minimum ECG, pulse oximetry, BP, urine output; add CVP and arterial line for patients not rapidly responding
- Use lactate and base deficit as end-points of resuscitation
- Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 2 (Shock and Haemorrhage)
Difference between simple pneumothorax and tension pneumothorax
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I have all the content needed from Bailey and Love. Here is the comprehensive comparison:
Simple Pneumothorax vs. Tension Pneumothorax
Bailey and Love's Short Practice of Surgery, 28th Edition
Definitions
Simple (Spontaneous) Pneumothorax
Presence of air in the pleural space outside the lung. Air enters through a breach in the visceral pleura (or chest wall) but there is no positive pressure build-up - pleural pressure remains at or near atmospheric levels. The affected lung partially or completely collapses, but there is no mediastinal shift and no haemodynamic compromise.
Tension Pneumothorax
A condition where a "one-way valve" mechanism allows air to enter the pleural space with each breath but prevents it from escaping. Air accumulates under progressively increasing positive pressure, completely collapsing the affected lung, flattening the diaphragm, distorting the mediastinum, and eventually compressing venous return to the heart - leading to cardiovascular collapse.
Bailey and Love (Ch. 60): "Tension pneumothorax is when (independent of aetiology) there is a build-up of positive pressure within the hemithorax, to the extent that the lung is completely collapsed, the diaphragm is flattened, the mediastinum is distorted and, eventually, the venous return to the heart is compromised."
Comparison Table
| Feature | Simple Pneumothorax | Tension Pneumothorax |
|---|---|---|
| Air entry mechanism | Single breach, air equilibrates | One-way valve - air enters but cannot escape |
| Intrapleural pressure | Atmospheric or slightly negative | Progressively increasing positive pressure |
| Lung collapse | Partial or complete (affected side) | Complete collapse of affected lung |
| Mediastinal shift | Absent | Present - shifted AWAY from the affected side |
| Tracheal deviation | Absent | Present (away from affected side) - late sign |
| Diaphragm | Normal position | Flattened on affected side |
| Haemodynamic status | Stable (no cardiovascular compromise) | Haemodynamic collapse (obstructive shock) |
| Venous return | Preserved | Compressed - drastically reduced |
| Neck veins | Normal | Distended (JVD) - raised CVP |
| Urgency | Semi-urgent / elective depending on size | Immediately life-threatening emergency |
| Diagnosis | Clinical + CXR confirmation acceptable | Clinical diagnosis only - NEVER delay for CXR |
| Breath sounds | Reduced on affected side | Absent on affected side |
| Percussion | Hyper-resonant on affected side | Hyper-resonant on affected side |
Aetiology / Causes
Simple Pneumothorax
Primary Spontaneous (PSP):
- Common in young males (mid-teens to late twenties); tall stature; family history
- Due to rupture of small blebs, vesicles or bullae - typically at the apex of the upper lobe or upper border of lower/middle lobes
- No underlying lung disease
Secondary Spontaneous (SSP):
- Older patients with underlying lung disease (emphysema, TB, cavitating disease, necrotising tumours)
- The pleural leak occurs as part of the underlying disease process
- Less well tolerated due to reduced pulmonary reserve
Traumatic / Iatrogenic:
- Rib fractures, penetrating chest injury
- Central line insertion, positive-pressure ventilation (barotrauma)
Tension Pneumothorax
Bailey and Love identifies four main causes:
- Penetrating chest trauma
- Blunt chest trauma with parenchymal lung injury and air leak that did not spontaneously close
- Iatrogenic (e.g. central venepuncture, positive-pressure ventilation)
- Mechanical positive-pressure ventilation - high airway pressures force air through a small breach
Clinical Features
Simple Pneumothorax
- Sudden onset pleuritic chest pain and breathlessness
- Degree of dyspnoea related to size of pneumothorax and underlying pulmonary reserve
- Reduced chest expansion on affected side
- Hyper-resonance on percussion
- Reduced/absent breath sounds
- Patient is haemodynamically stable
- No tracheal deviation
Tension Pneumothorax
Bailey and Love describes the presentation as dramatic:
- Increasing restlessness
- Tachypnoea and dyspnoea (severe)
- Distended neck veins (raised JVP - similar to pericardial tamponade)
- Hyper-resonance over affected hemithorax
- Decreased or absent breath sounds over affected side
- Tracheal deviation away from affected side - this is a late finding and is not required to confirm the diagnosis
- Haemodynamic collapse - hypotension, tachycardia, cyanosis
- Deteriorating consciousness
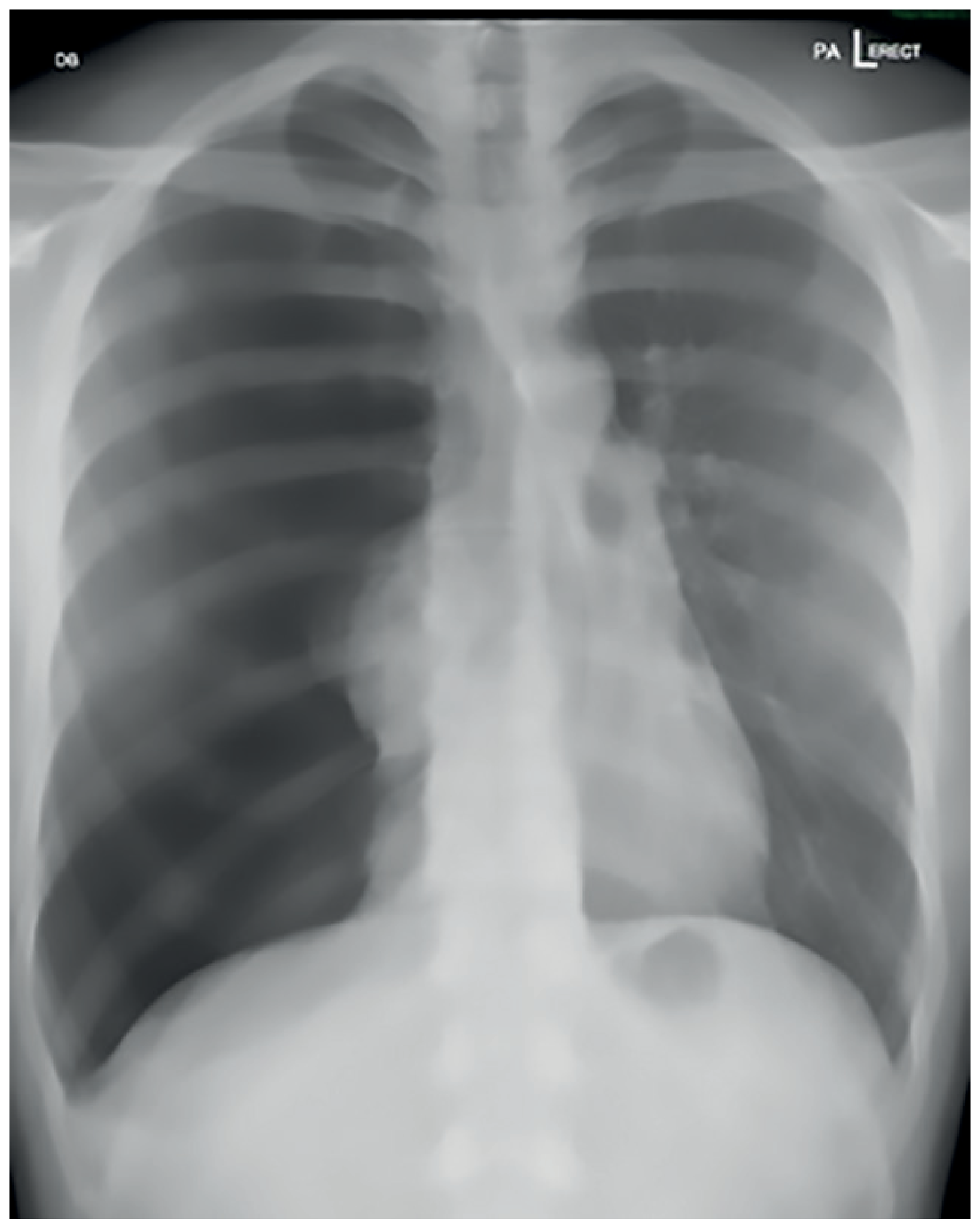
Note the rightward tracheal deviation, complete collapse of the left lung, depressed left hemidiaphragm, and mediastinal shift - classical CXR findings of left-sided tension pneumothorax.
Danger: Tension Pneumothorax vs. Pericardial Tamponade
Both present with distended neck veins + hypotension + tachycardia. Key differentiating features:
| Feature | Tension Pneumothorax | Pericardial Tamponade |
|---|---|---|
| Breath sounds | Absent (one side) | Present bilaterally |
| Hyper-resonance | Yes | No |
| Tracheal deviation | May be present | Absent |
| Heart sounds | Normal | Muffled |
| eFAST | No pericardial fluid | Pericardial fluid visible |
Tension pneumothorax is listed by Bailey and Love as one of the "Deadly Dozen" - six immediately life-threatening chest injuries:
- Airway obstruction
- Tension pneumothorax
- Pericardial tamponade
- Open pneumothorax
- Massive haemothorax
- Flail chest
Treatment
Simple Pneumothorax
Management follows BTS (British Thoracic Society) guidelines based on type and size:
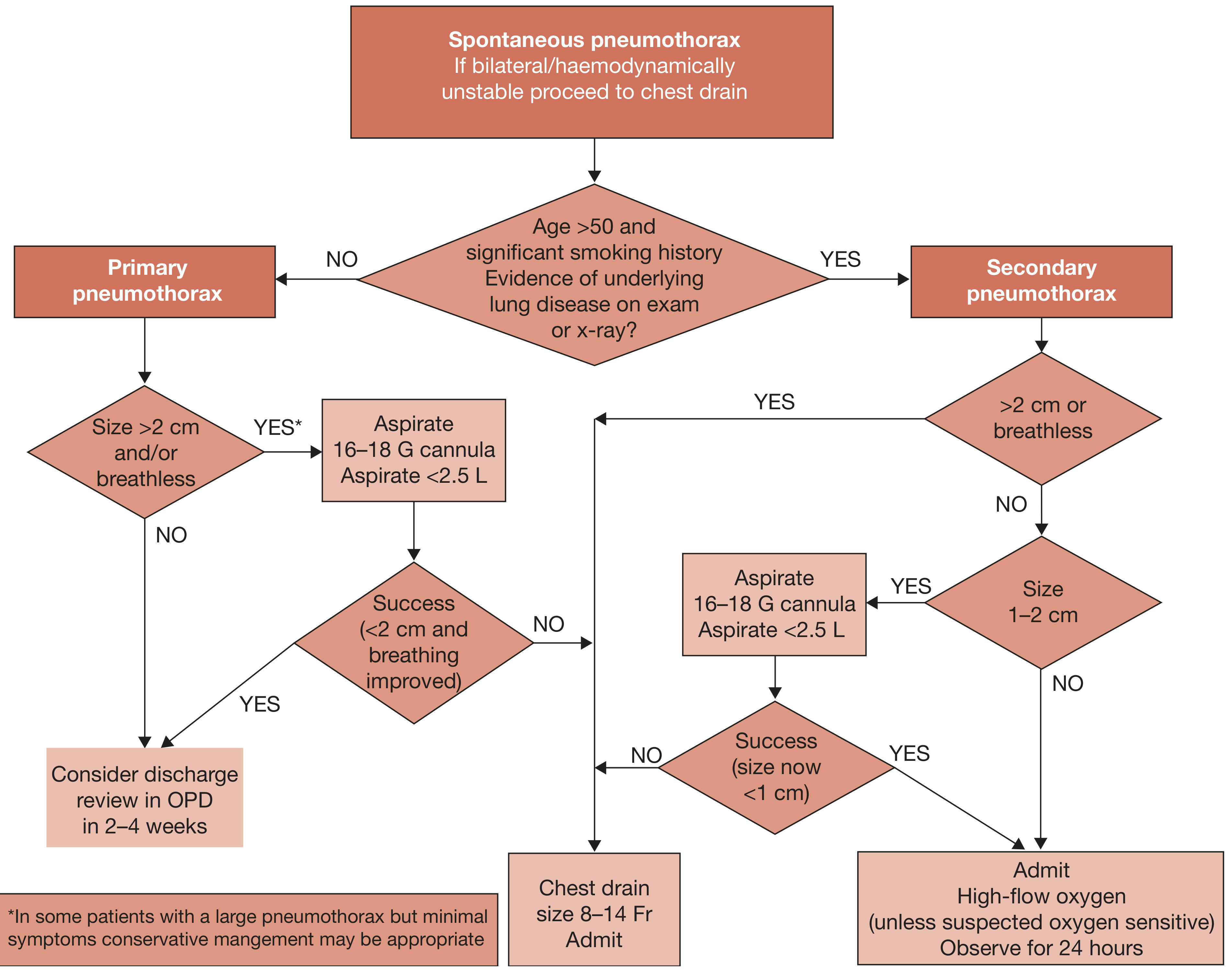
Primary Spontaneous Pneumothorax (PSP):
- Small (<2 cm, not breathless) - conservative management, discharge, OPD review in 2-4 weeks
- Large (>2 cm) or breathless - needle aspiration via 16-18G cannula (aspirate <2.5 L)
- Success (size now <2 cm, breathing improved) - consider discharge
- Failure - chest drain (8-14 Fr), admit
Secondary Spontaneous Pneumothorax (SSP):
-
2 cm or breathless - needle aspiration first; if fails, chest drain + admit
- 1-2 cm - admit, high-flow oxygen (unless O2-sensitive), observe 24 hours
- <1 cm - admit, observe
Surgical indications (Summary Box 60.1):
- Second ipsilateral pneumothorax
- First contralateral pneumothorax
- Bilateral spontaneous pneumothorax
- Pneumothorax failing to settle despite drainage
- Spontaneous haemothorax; professions at risk (pilots, divers)
- Pregnancy
Chest drain insertion site (Bailey and Love "safe triangle"):
- Anterior to the mid-axillary line
- Above the nipple level
- Below and lateral to pectoralis major
- Ideally at the 5th intercostal space; always above the upper border of the lower rib (to avoid neurovascular bundle)
- Current recommendation: small bore (10-14 Fr) Seldinger-type drain, under ultrasound guidance
Tension Pneumothorax - Emergency Treatment
Bailey and Love is explicit:
"Tension pneumothorax is a clinical diagnosis and treatment should NEVER be delayed by waiting for radiological confirmation."
Step 1 - Immediate Decompression:
- Historically: large-bore cannula (14G) into the 2nd intercostal space, mid-clavicular line
- Current preferred approach: direct chest drain insertion into the "safe triangle" (4th/5th ICS, anterior axillary line)
- In extremis (no equipment/time): finger thoracostomy at the same location - finger inserted through the chest wall to allow immediate air escape
Step 2 - Definitive drainage:
- Formal intercostal chest tube (large bore) connected to underwater seal
- Relieves the positive pressure, allows lung to re-expand
Key principle: In a ventilated patient who suddenly deteriorates, tension pneumothorax must be the first diagnosis excluded and treated immediately.
Recurrence
Simple spontaneous pneumothorax has significant recurrence rates:
- After 1st episode: ~30% risk of recurrence
- After 2nd episode: risk rises substantially - surgical management indicated
Tension pneumothorax does not "recur" as such - the underlying air leak source requires definitive treatment.
- Bailey and Love's Short Practice of Surgery, 28th Edition, Chapters 29 (Thoracic Trauma) and 60 (Thoracic Surgery)
This is a shared conversation. Sign in to Orris to start your own chat.