Explain the formation of urine according to renal physiology, Guyton and Hall textbook.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the key content. Here is the complete, detailed explanation of urine formation drawn directly from Guyton and Hall.
Formation of Urine - Guyton and Hall Textbook of Medical Physiology
Overview: The Master Equation
Urine formation is the net result of three fundamental renal processes:
Urinary Excretion = Glomerular Filtration - Tubular Reabsorption + Tubular Secretion
The kidneys filter approximately 180 L of plasma per day, yet excrete only about 1-2 L as urine. This means more than 99% of filtered fluid is reclaimed. Each step is described below.
1. Nephron Structure - The Functional Unit
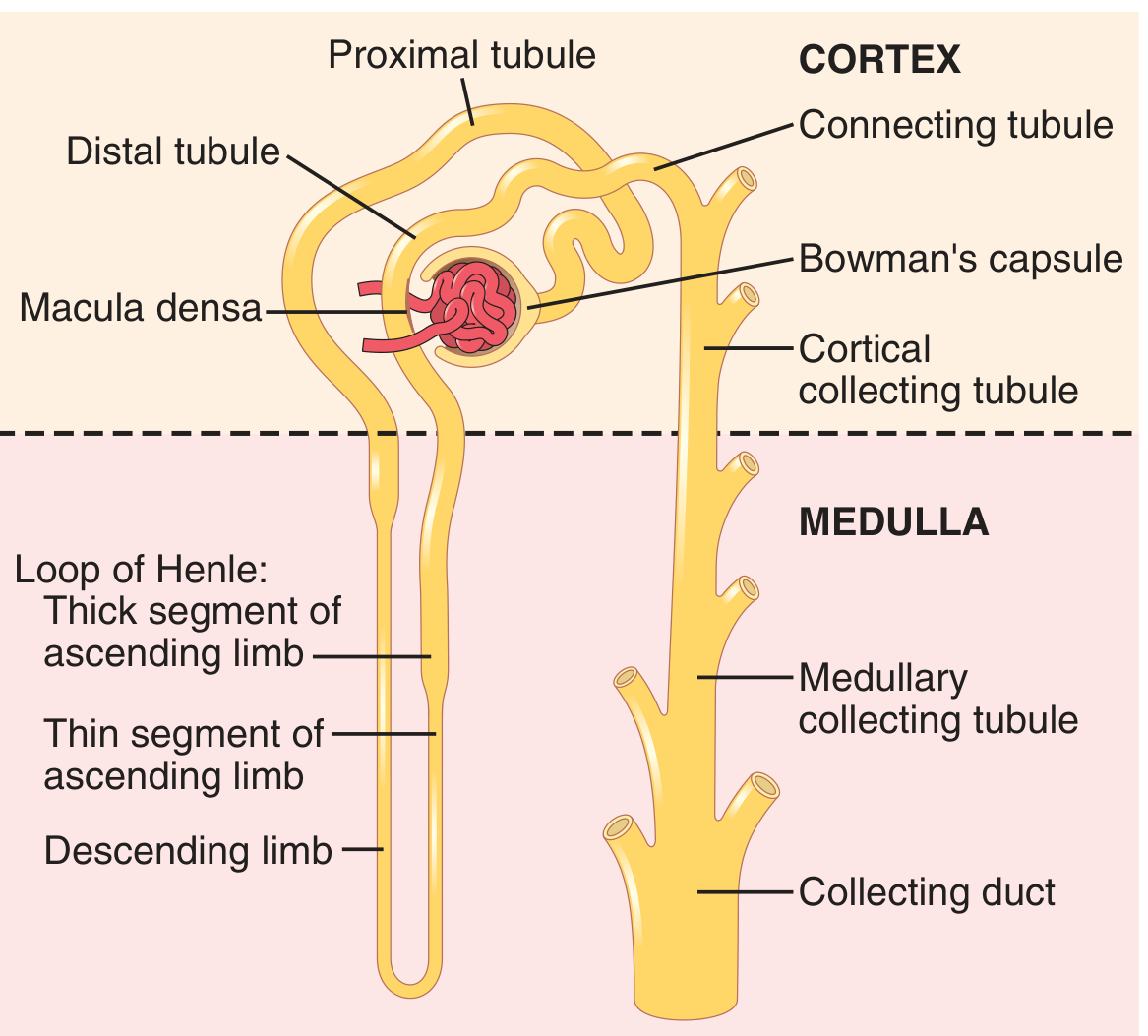
Figure 26.4 - Basic tubular segments of the nephron (Guyton and Hall)
Each kidney contains about 1 million nephrons. Filtrate flows sequentially through:
- Bowman's capsule - receives the glomerular filtrate
- Proximal tubule - lies in the cortex; site of bulk reabsorption
- Loop of Henle - dips into the medulla (thin descending + thin/thick ascending limbs)
- Distal tubule - returns to the cortex; contains the macula densa
- Cortical and medullary collecting ducts - final concentration/dilution of urine
- Renal pelvis - approximately 250 large collecting ducts drain here
Cortical nephrons (~70-80%) have short loops of Henle. Juxtamedullary nephrons (~20-30%) have long loops that penetrate deep into the medulla and are essential for producing concentrated urine.
2. Step 1 - Glomerular Filtration
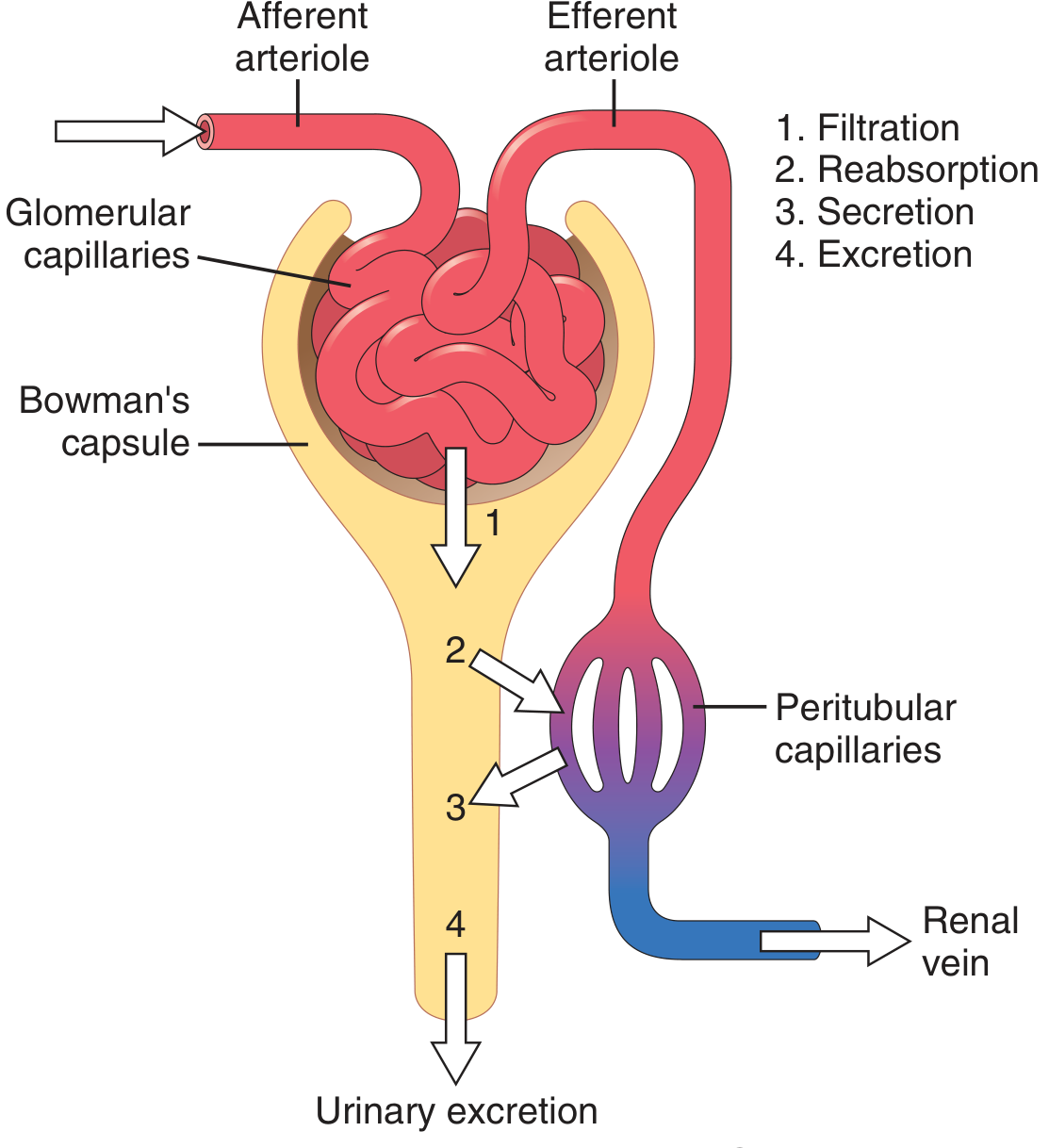
Figure 26.6 - Basic kidney processes that determine the composition of urine (Guyton and Hall)
What is filtered?
The glomerular capillaries are relatively impermeable to proteins. The filtrate is therefore essentially protein-free plasma - containing water, ions, glucose, amino acids, urea, creatinine, and small molecules at concentrations nearly identical to plasma. Substances partially bound to plasma proteins (e.g., ~50% of calcium, most fatty acids) are only partially filtered.
Glomerular Filtration Rate (GFR)
- Normal GFR: ~125 mL/min, or 180 L/day
- The filtration fraction = GFR / Renal plasma flow = ~0.2 (20% of renal plasma flow is filtered)
- GFR is ~10% lower in women than men; it declines substantially with normal aging (~50% reduction from age 18-29 to age 70-75)
Forces Governing GFR - The Starling Forces
GFR is determined by:
GFR = Kf × Net Filtration Pressure
Where net filtration pressure = (Glomerular hydrostatic pressure) - (Bowman's capsule pressure) - (Glomerular colloid osmotic pressure):
| Force | Value | Effect on GFR |
|---|---|---|
| Glomerular capillary hydrostatic pressure (P_G) | ~60 mm Hg | Favors filtration |
| Bowman's capsule hydrostatic pressure (P_B) | ~18 mm Hg | Opposes filtration |
| Glomerular colloid osmotic pressure (πG) | ~32 mm Hg | Opposes filtration |
| Net filtration pressure | ~10 mm Hg | Favors filtration |
The glomerular filtration coefficient (Kf) = permeability × surface area of glomerular capillaries; it is much higher than in most other capillaries.
The Glomerular Capillary Membrane
The filtration barrier has three layers:
- Capillary endothelium - fenestrated (pores ~70-100 nm), prevents passage of blood cells
- Glomerular basement membrane (GBM) - gel of collagen and proteoglycans; negative charges repel anionic proteins
- Podocytes (visceral epithelium) - foot processes with filtration slits (~25-60 nm); negatively charged glycocalyx
This barrier is ~500 times more permeable to water and small solutes than typical muscle capillaries, yet highly restrictive to proteins.
Factors That Reduce GFR
- Decreased Kf (renal disease, diabetes, hypertension, aging)
- Increased Bowman's capsule pressure (urinary tract obstruction, e.g., kidney stones)
- Increased glomerular colloid osmotic pressure (reduced renal blood flow, increased plasma proteins)
- Reduced glomerular hydrostatic pressure (reduced arterial pressure, increased afferent arteriolar resistance from sympathetic activation)
3. Step 2 - Tubular Reabsorption
Scale and Selectivity
Tubular reabsorption is quantitatively massive and highly selective. From the 180 L filtered daily:
| Substance | Filtered/day | Excreted/day | % Reabsorbed |
|---|---|---|---|
| Water | 180 L | 1.8 L | 99% |
| Sodium | 630 g | 3.2 g | 99.5% |
| Glucose | 180 g | 0 g | ~100% |
| Urea | 54 g | 30 g | ~44% |
| Creatinine | ~1.8 g | ~1.8 g | ~0% |
Glucose and amino acids are almost completely reabsorbed (virtually none in urine normally). Waste products like urea and creatinine are poorly reabsorbed and efficiently excreted.
Mechanisms of Reabsorption
Primary Active Transport - uses energy directly from ATP hydrolysis. The Na⁺-K⁺-ATPase pump on the basolateral side of tubular cells is the central driver: it pumps Na⁺ out of cells into the interstitium, maintaining a low intracellular Na⁺ concentration that creates the gradient for luminal Na⁺ entry.
Secondary Active Transport - coupled indirectly to energy via ion gradients. Glucose reabsorption is the classic example: Na⁺-glucose co-transporters (SGLT2 in the proximal tubule) use the Na⁺ gradient generated by the Na⁺-K⁺-ATPase to drive glucose against its concentration gradient.
Transport Maximum (Tm) - carrier systems become saturated at high filtered loads:
- Glucose Tm: ~375 mg/min (threshold ~200 mg/100 mL plasma; above this, glucosuria occurs)
- Amino acids Tm: ~1.5 mmol/min
- Phosphate Tm: ~0.10 mmol/min
Passive transport - water is always reabsorbed passively by osmosis following active solute reabsorption. Urea and some ions diffuse passively down concentration gradients.
Pathways of Reabsorption
- Transcellular - through the tubular cell (apical membrane entry, basolateral exit)
- Paracellular - between cells via tight junctions and intercellular spaces (important for bulk Na⁺, water, and divalent ions in the proximal tubule)
Segment-by-Segment Reabsorption
Proximal tubule: Reabsorbs ~65% of filtered Na⁺, water, and Cl⁻; essentially 100% of glucose and amino acids; most bicarbonate (via H⁺ secretion and carbonic anhydrase). Isosmotic reabsorption - fluid osmolarity does not change.
Loop of Henle (descending limb): Permeable to water but NOT to solutes - water is drawn out by the hypertonic medullary interstitium, concentrating the tubular fluid.
Loop of Henle (thick ascending limb): Actively transports Na⁺, K⁺, Cl⁻ (via NKCC2 co-transporter) but is impermeable to water - this dilutes the tubular fluid and creates/maintains the medullary osmotic gradient. This is the site of action of loop diuretics (furosemide).
Distal tubule and collecting duct: Fine-tuning of Na⁺, K⁺, acid-base, and water. Aldosterone increases Na⁺ reabsorption and K⁺ secretion here. ADH (vasopressin) inserts aquaporin-2 channels in collecting duct principal cells, making them permeable to water for final concentration of urine.
4. Step 3 - Tubular Secretion
Secretion moves substances from peritubular capillary blood into the tubular lumen, adding to the urinary load beyond what was filtered. Key secreted substances:
- H⁺ ions - secreted throughout the tubule (proximal, distal, collecting duct); critical for acid-base regulation
- K⁺ ions - secreted by principal cells of the collecting duct under aldosterone control; accounts for most urinary K⁺ excretion
- Organic anions and cations - including drugs (penicillin, PAH), toxins, and metabolites secreted by active transporters in the proximal tubule
- Creatinine - has a small secreted component
Secretion also has transport maximums:
- Creatinine Tm: ~16 mg/min
- Para-aminohippuric acid (PAH) Tm: ~80 mg/min (PAH is used to estimate renal plasma flow)
5. Excretion and the Final Urine
After filtration, reabsorption, and secretion, the final urine flows:
- Collecting ducts → Renal calyces → Renal pelvis
- Urine composition is not changed as it passes through the calyces and ureters
- Peristaltic contractions (initiated by pacemaker activity in the calyces) propel urine through the ureters (25-35 cm long) to the bladder
- The oblique entry of ureters through the detrusor muscle prevents vesicoureteral reflux
Urinary Excretion Summary
A 10% decrease in tubular reabsorption (from 178.5 to 160.7 L/day) could increase urine volume nearly 13-fold (from 1.5 to 19.3 L/day) if GFR remained constant - illustrating why tight coordination between filtration and reabsorption is physiologically essential.
Summary Table
| Process | Location | Key Features |
|---|---|---|
| Glomerular filtration | Glomerulus / Bowman's capsule | 180 L/day; protein-free; driven by hydrostatic pressure (~10 mm Hg net) |
| Proximal tubular reabsorption | Proximal tubule | 65% of Na⁺/water; 100% glucose/amino acids; isosmotic |
| Loop concentration | Loop of Henle | Creates medullary gradient; thick ascending limb impermeable to water |
| Distal/collecting duct regulation | Distal tubule + collecting duct | Aldosterone (Na⁺/K⁺); ADH (water); fine-tuning |
| Tubular secretion | Throughout tubule | H⁺, K⁺, drugs, organic acids |
| Urinary excretion | Collecting duct → ureter → bladder | ~1.5 L/day final urine |
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 26 (The Urinary System: Functional Anatomy and Urine Formation) and Chapter 27-28 (Glomerular Filtration, Renal Blood Flow; Renal Tubular Reabsorption and Secretion).
Explain the countercurrent multiplier and concentration gradient in the loop of Henle
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have all the content and diagrams needed. Here is the full, detailed explanation.
Countercurrent Multiplier and Concentration Gradient in the Loop of Henle
The Core Requirement: Why a Gradient Is Needed
Before the mechanism itself, Guyton and Hall establish the context clearly:
"The basic requirements for forming a concentrated urine are (1) a high level of ADH... and (2) a high osmolarity of the renal medullary interstitial fluid, which provides the osmotic gradient necessary for water reabsorption to occur."
- Normal body interstitial fluid osmolarity: ~300 mOsm/L
- Renal medullary interstitial osmolarity: progressively increasing from 300 mOsm/L at the corticomedullary junction to 1200-1400 mOsm/L at the papillary tip
This hyperosmotic medullary interstitium is generated and maintained by the countercurrent multiplier mechanism, which depends critically on the anatomical arrangement of juxtamedullary nephrons.
Anatomical Prerequisites
The countercurrent multiplier requires three parallel structures running in a U-shaped arrangement into the medulla:
- Loop of Henle (of juxtamedullary nephrons, ~20-25% of all nephrons) - some extend all the way to the papillary tips
- Vasa recta - specialized peritubular capillaries that parallel the loops of Henle
- Collecting ducts - pass through the hyperosmotic medulla on their way to the renal pelvis
The key is that fluid in the descending limb flows downward (cortex → medulla) while fluid in the ascending limb flows upward (medulla → cortex) - flowing in opposite directions in adjacent channels. This countercurrent arrangement is the anatomical basis of the mechanism.
Differential Permeability Properties - The Functional Basis
The ascending and descending limbs have opposite transport properties, which is essential:
| Segment | Water Permeability | Solute Transport |
|---|---|---|
| Descending limb (thin) | High - water freely moves out | Low - largely impermeable to NaCl |
| Thin ascending limb | Near zero - impermeable to water | Passive NaCl reabsorption |
| Thick ascending limb | Near zero - impermeable to water | Active NaCl transport out (NKCC2) |
The thick ascending limb is the engine of the system. It actively pumps Na⁺, K⁺, and Cl⁻ out via the NKCC2 co-transporter (the target of loop diuretics like furosemide) but water cannot follow - so solute accumulates in the interstitium without dilution.
"This pump is capable of establishing about a 200 mOsm/L concentration gradient between the tubular lumen and interstitial fluid."
This ~200 mOsm/L difference between lumen and interstitium at any given level is called the "single effect" - the basic unit that gets multiplied along the length of the loop.
How the Gradient Is Built: Step-by-Step
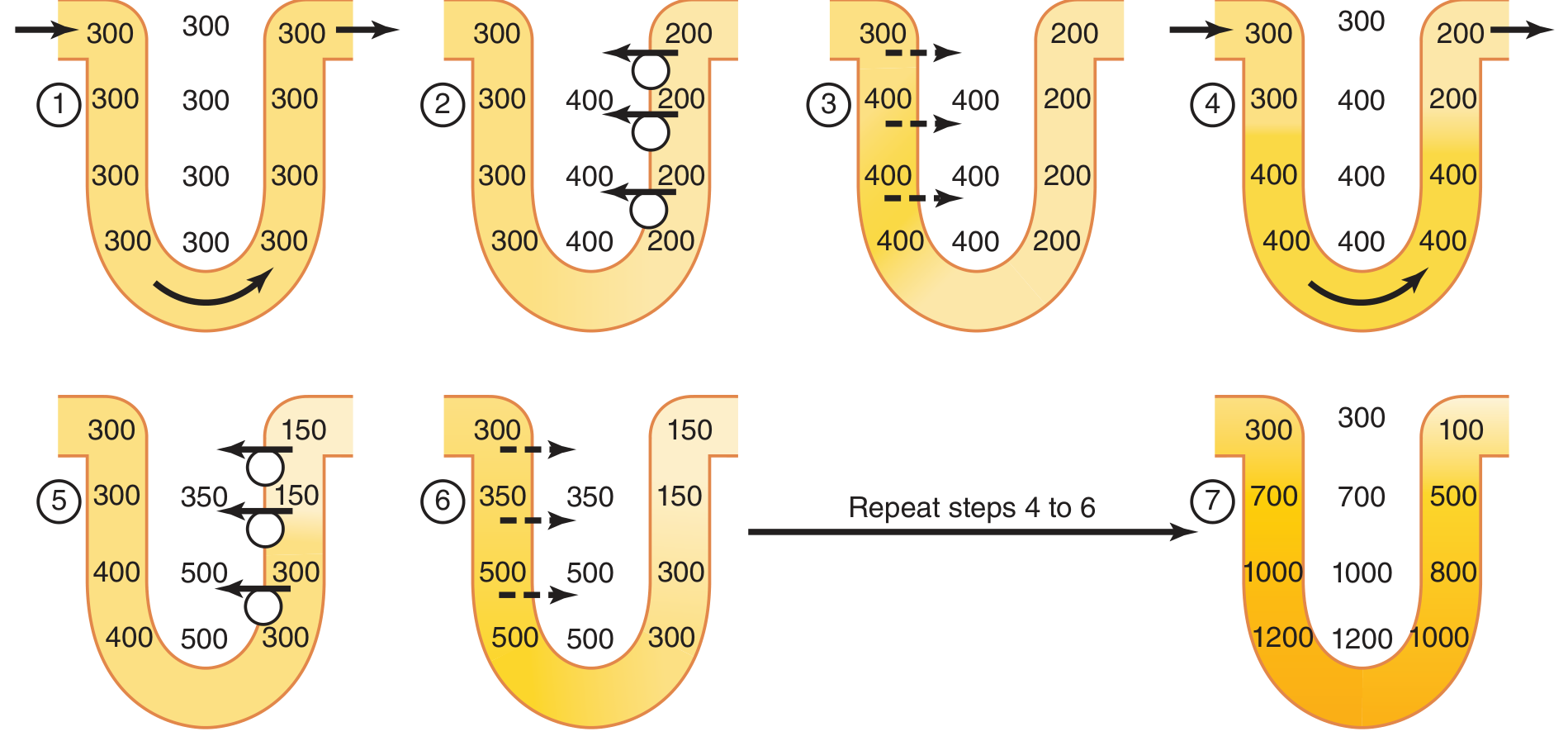
Figure 29.4 - Countercurrent multiplier system in the loop of Henle (Guyton and Hall). Each cycle repeats steps 4-6 until the final gradient of 1200 mOsm/L is achieved at the papillary tip.
The mechanism unfolds in repeating cycles (as shown in the diagram above):
Step 1: Initially, all fluid throughout the loop is isotonic at 300 mOsm/L.
Step 2 (The Single Effect): The thick ascending limb pumps NaCl into the interstitium, creating a 200 mOsm/L gradient - the ascending limb lumen drops to 200, the interstitium rises to 400. Because the ascending limb is water-impermeable, no water follows.
Step 3: The interstitium is now hyperosmotic. Water is drawn osmotically out of the descending limb (which IS water-permeable), concentrating the fluid in the descending limb to equilibrate with the interstitium.
Step 4: New isosmotic fluid (300 mOsm/L) from the proximal tubule pushes the concentrated descending limb fluid further down toward the bend, shifting the gradient downward.
Steps 5-6: The ascending limb again pumps out another 200 mOsm/L increment, this time from an already more concentrated starting point. The descending limb again equilibrates with the higher interstitial osmolarity.
Step 7 (Steady State): After repeating this cycle many times, a progressive axial osmotic gradient is established:
- Corticomedullary junction: ~300 mOsm/L
- Mid-medulla: ~600-700 mOsm/L
- Papillary tip: ~1200 mOsm/L
The key insight is that while the pump can only generate a 200 mOsm/L gradient at any single horizontal level, the countercurrent arrangement multiplies this single effect along the entire length of the loop, ultimately producing a gradient many times larger (1200 mOsm/L) from corticomedullary border to papillary tip. This is why it is called a multiplier.
What Leaves the Loop of Henle
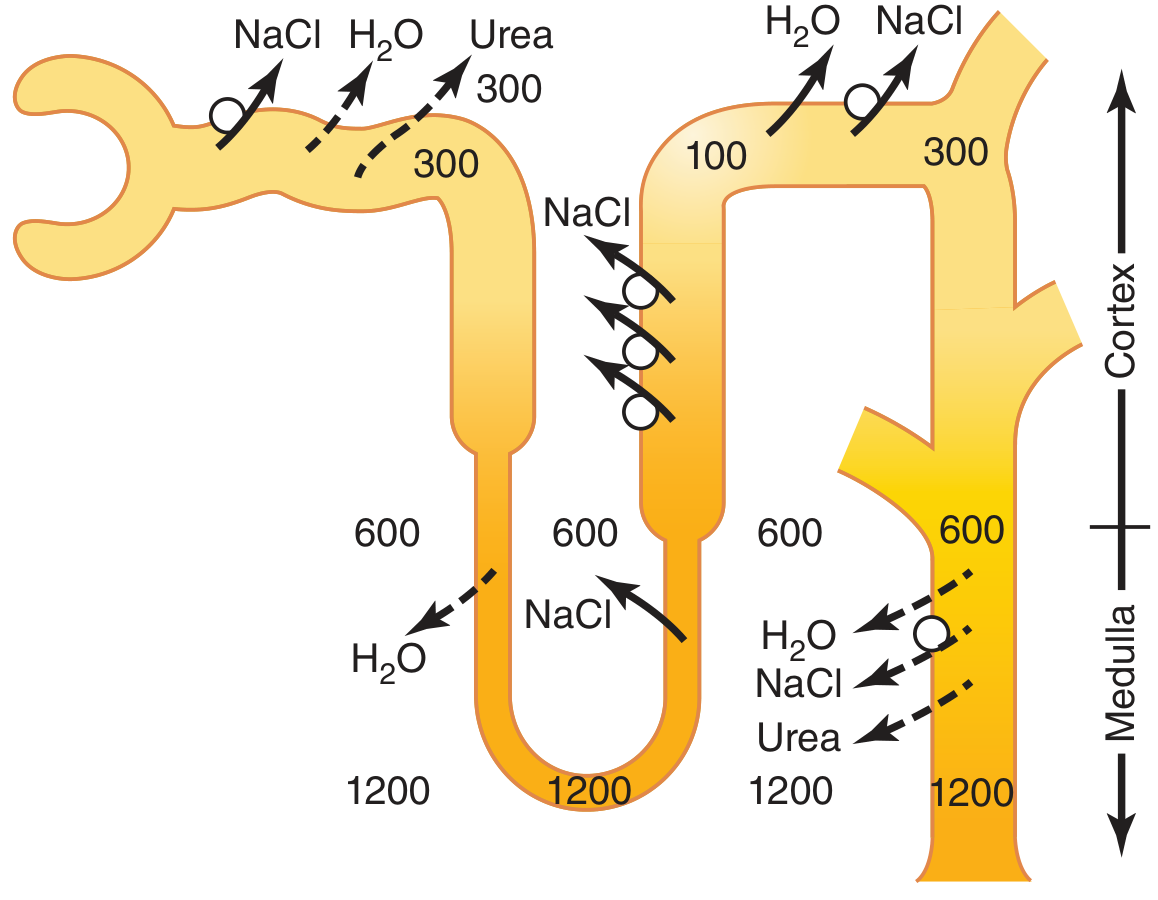
Figure 29.5 - Formation of concentrated urine when ADH levels are high (Guyton and Hall). Numbers are osmolarity values in mOsm/L.
Paradoxically, the fluid leaving the ascending limb at the macula densa is actually dilute - about 100 mOsm/L. This is because the ascending limb has been actively pumping solutes out but water cannot follow. The medulla has been enriched, while the ascending limb fluid has been depleted of solute.
This dilute fluid (100 mOsm/L) then enters the distal tubule and cortical collecting duct. What happens next depends on ADH levels:
- High ADH (water deficit): Collecting ducts become permeable to water via aquaporin-2 insertion. As the collecting duct descends through the hyperosmotic medullary gradient (300 → 600 → 1200 mOsm/L), water is drawn out by osmosis at each level. The final urine equilibrates with the papillary interstitium at ~1200 mOsm/L - maximally concentrated.
- Low/absent ADH (water excess): Collecting ducts remain impermeable to water. Dilute fluid passes through unchanged, producing a dilute urine of 50-100 mOsm/L.
Urea's Contribution (~40-50% of Medullary Osmolarity)
NaCl alone cannot account for all 1200 mOsm/L. Urea contributes 500-600 mOsm/L (~40-50%) to the medullary gradient through a recycling mechanism:
- Urea is concentrated in the cortical collecting duct as water is reabsorbed under ADH (urea cannot follow - low urea permeability here)
- Highly concentrated urea enters the inner medullary collecting duct, which has urea transporters (UT-A1 on the apical membrane, UT-A3 on the basolateral membrane) - both upregulated by ADH
- Urea diffuses passively down its concentration gradient into the medullary interstitium
- Some urea re-enters the thin descending limb of the loop of Henle and recirculates (urea recycling)
"Malnutrition is associated with a low urea concentration in the medullary interstitium and considerable impairment of urine-concentrating ability." - This confirms urea's functional importance.
The Vasa Recta - Countercurrent Exchanger (Preservation, Not Creation)
The vasa recta do not create the medullary gradient - they prevent it from being washed away. Two protective features:
- Low blood flow - less than 5% of total renal blood flow, minimizing solute washout
- Countercurrent exchange geometry - blood descends and picks up solutes (becomes hyperosmotic at 1200 mOsm/L at the tip), then ascends and returns solutes to the interstitium
"Although large amounts of fluid and solute are exchanged across the vasa recta, there is little net dilution of the concentration of the interstitial fluid at each level of the renal medulla because of the U shape of the vasa recta capillaries."
The vasa recta carry away only as much solute and water as is reabsorbed from the medullary tubules - the gradient is preserved at steady state.
Summary: The Complete Picture
| Feature | Key Value/Fact |
|---|---|
| Single effect (pump gradient) | ~200 mOsm/L per horizontal level |
| Final papillary osmolarity | ~1200-1400 mOsm/L |
| Descending limb | Permeable to water; fluid becomes concentrated |
| Thick ascending limb | Impermeable to water; actively pumps NaCl (NKCC2) |
| Fluid leaving ascending limb | ~100 mOsm/L (dilute) |
| NaCl contribution to gradient | ~600-700 mOsm/L |
| Urea contribution to gradient | ~500-600 mOsm/L (~40-50%) |
| ADH effect | Opens aquaporin-2; collecting duct water reabsorption |
| Max urine concentration with ADH | ~1200 mOsm/L |
| Vasa recta function | Countercurrent exchange - preserves gradient |
The elegance of the system is that the same tubule that generates a hyperosmotic medulla (by losing solute in the ascending limb) also concentrates itself on the way down (by losing water in the descending limb). The two limbs cooperate in opposite directions - hence "countercurrent" - and the combined effect is multiplied along the entire corticomedul lary axis.
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 29 (Urine Concentration and Dilution; Regulation of Extracellular Fluid Osmolarity and Sodium Concentration), pp. 373-378.
This is a shared conversation. Sign in to Orris to start your own chat.