Symblepharon
Reading File
Finding Sources
Finding Sources
Searching PubMed
symblepharon
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from both the Wills Eye Manual and Kanski's Clinical Ophthalmology. Let me compose the full answer.
Symblepharon
Definition: Symblepharon (plural: symblephara) is the adhesion - fibrous fusion - between the palpebral (tarsal) conjunctiva of the eyelid and the bulbar conjunctiva overlying the eyeball. It can be partial (band-like strands) or total (complete obliteration of the fornix).
Causes (Differential Diagnosis)
Symblepharon is a non-specific finding resulting from cicatrizing conjunctivitis or injury. Key causes include:
| Category | Examples |
|---|---|
| Autoimmune / cicatrizing | Mucous membrane pemphigoid (MMP)/Ocular cicatricial pemphigoid (OCP) - most classic and progressive cause |
| Stevens-Johnson syndrome / TEN | Acute onset; precipitated by sulfa drugs, penicillin, phenytoin, herpes, Mycoplasma |
| Chemical injury | Alkali burns > acid burns |
| Trauma / radiation | Direct mechanical or radiation-induced scarring |
| Membranous conjunctivitis | Post-adenoviral or beta-hemolytic Streptococcal |
| Atopic keratoconjunctivitis | Chronic allergic inflammation |
| Drugs (topical) | Pilocarpine, phospholine iodide, antiviral agents |
| Iatrogenic | Post-surgical scarring |
| Congenital | Rare |
Key note: Symblepharon following a single insult (burn, SJS) tends to be stable, while that associated with MMP/OCP is typically progressive.
- The Wills Eye Manual, p. 401; p. 356
- Kanski's Clinical Ophthalmology 10th ed., p. 648
Staging (in the context of MMP/OCP)
Foster's Classification (most widely used)
| Stage | Features |
|---|---|
| I | Chronic conjunctivitis with tear dysfunction and subepithelial fibrosis |
| II | Forniceal shortening (especially inferior) |
| III | Symblepharon formation |
| IV | Surface keratinization and cicatricial ankyloblepharon (lid fused to globe) |
Mondino's Classification (based on inferior forniceal depth loss)
| Stage | Forniceal depth loss |
|---|---|
| I | Up to 25% |
| II | 25-50% |
| III | 50-75% |
| IV | >75% |
- Kanski's Clinical Ophthalmology 10th ed., p. 621-638
Clinical Features
Symptoms (insidious onset, bilateral): dryness, redness, foreign body sensation, burning, blepharospasm, photophobia, decreased vision. Typically occurs in patients >55 years. Course: remissions and exacerbations.
Signs:
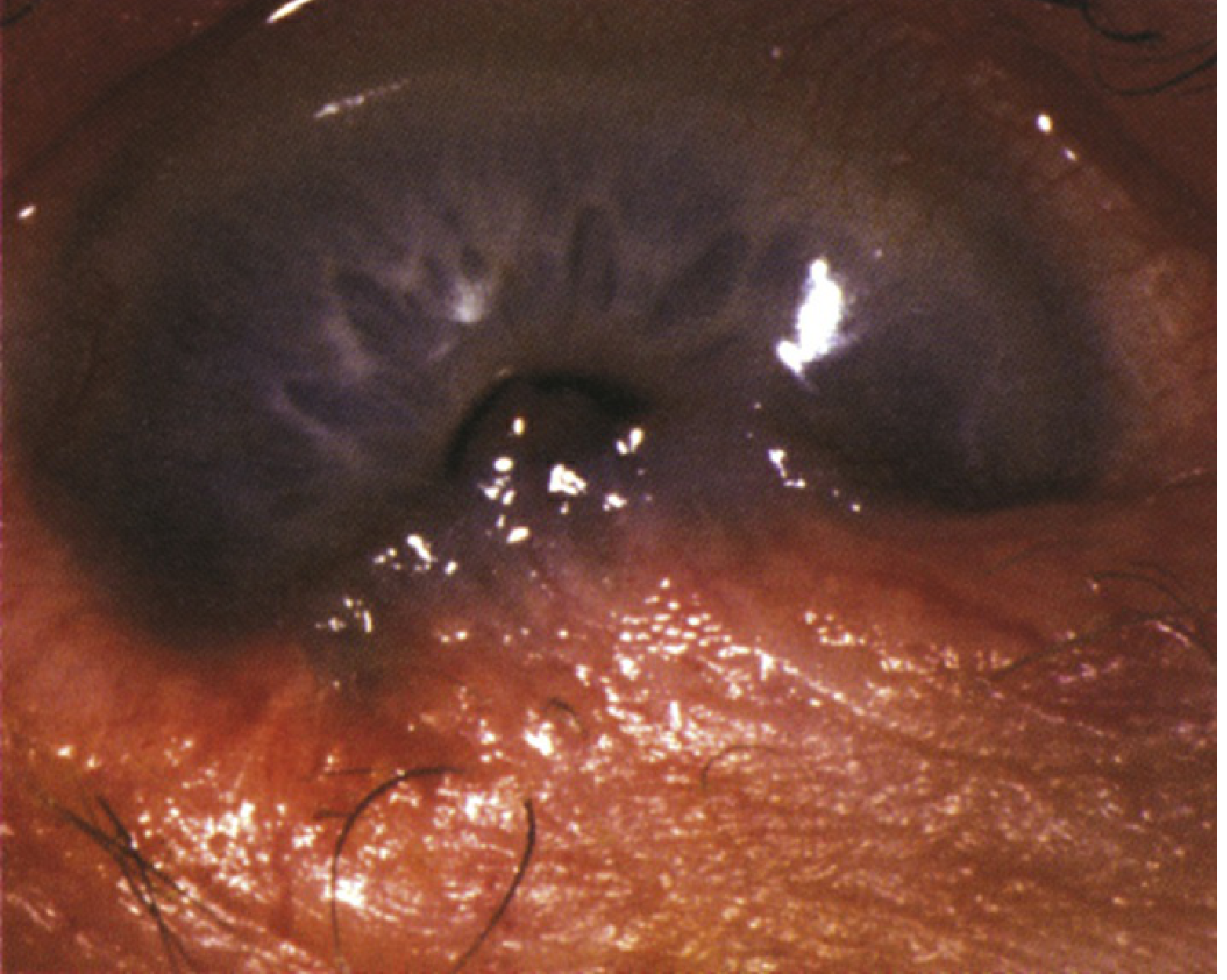
- Critical: Inferior symblepharon - linear conjunctival folds connecting palpebral to bulbar conjunctiva; best seen by pulling down the lower lid during upgaze
- Foreshortening and tightening of the inferior fornix
- Palpebral conjunctival scarring on eyelid eversion
- Secondary: SPK (superficial punctate keratopathy), bacterial conjunctivitis, corneal ulcer
Later/End-stage findings:
- Severe dry eye (goblet cell and lacrimal gland destruction)
- Entropion, trichiasis, distichiasis
- Corneal opacification with pannus and neovascularization
- Ankyloblepharon (upper and lower lids fused at the outer canthus)
- Limitation of ocular motility
- Total symblepharon with corneal opacification (end-stage)
Systemic features (in MMP): mucous membrane vesicles and scarring (oropharynx, esophagus, vagina, urethra, anus); desquamative gingivitis; cutaneous bullae.
- The Wills Eye Manual, pp. 355-357
- Kanski's Clinical Ophthalmology 10th ed., pp. 648-675
Workup
- History - long-term topical medications? acute systemic illness? recent systemic drug use?
- Skin and mucous membrane examination
- Slit-lamp exam - check inferior fornix depth, evert lids for palpebral scarring, check IOP
- Gram stain and culture if secondary bacterial infection suspected
- Conjunctival biopsy (using Michel's transport medium) for:
- Direct immunofluorescence: linear IgG, IgA, or C3 at the basement membrane zone (confirmatory for MMP)
- Indirect immunofluorescence for circulating antibodies
- Multidisciplinary consults as appropriate (dermatology, oculoplastics, ENT, GI, pulmonology)
Treatment
Supportive / Ocular Surface
- Preservative-free artificial tears 4-10x/day; ointment b.i.d.-q.i.d. and at night; autologous serum drops 20-50%
- Scleral lenses to maintain ocular surface integrity
- Moisture chamber goggles
- Punctal occlusion (if puncta not already scarred closed)
- Treat blepharitis: lid hygiene, warm compresses, topical erythromycin; oral doxycycline for anti-inflammatory effect
Medical (Immunosuppression)
- Topical steroids - for acute flares only; use with caution (risk of corneal melting)
- Systemic steroids (prednisone 60 mg/day) - for acute exacerbations; most effective combined with immunomodulators
- Immunosuppressives (for progressive disease): mycophenolate mofetil, methotrexate, cyclophosphamide, rituximab, IV immunoglobulin
- Dapsone - start 25 mg/day; increase by 25 mg every 4-7 days; target 100-150 mg/day; maintain for months then taper slowly
- Caution: check G-6-PD before starting; monitor CBC weekly during dose escalation (hemolysis risk)
Surgical
- Entropion correction; cryotherapy or electrolysis for trichiasis - only when inflammation is absent
- Mucous membrane grafts (buccal or amniotic membrane) to reconstruct fornices
- Keratoprosthesis for end-stage disease with good posterior segment function (guarded long-term prognosis)
Follow-up
-
Every 1-2 weeks during acute exacerbations
-
Every 1-6 months during remission
-
The Wills Eye Manual, pp. 357-358
Recent evidence note: A 2024 systematic review and meta-analysis on ocular MMP (PMID 39074301) provides updated data on the clinical characteristics of this condition, the most common cause of progressive symblepharon.
Symblepharon
Reading File
Finding Sources
Finding Sources
Searching PubMed
symblepharon treatment cicatrizing conjunctivitis
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - both images are now available. Here is the complete, comprehensive answer.
Symblepharon
Definition: Symblepharon (plural: symblephara) is a fibrous adhesion between the palpebral (tarsal) conjunctiva of the eyelid and the bulbar conjunctiva covering the eyeball. It represents the end result of conjunctival scarring from any cicatrizing process. It may be partial (band-like strands tethering the surfaces) or total (complete obliteration of the fornix).
Causes / Differential Diagnosis
Symblepharon is a non-specific sign - it can follow any severe conjunctival inflammation or injury. Key causes:
| Cause | Notes |
|---|---|
| Mucous membrane pemphigoid (MMP) / Ocular cicatricial pemphigoid (OCP) | Most classic; typically progressive and bilateral |
| Stevens-Johnson syndrome (SJS) / Toxic epidermal necrolysis (TEN) | Acute onset; drugs (sulfa, penicillin, phenytoin) or infections (herpes, Mycoplasma) |
| Chemical injury | Alkali > acid burns |
| Trauma / radiation | Single-event scarring; usually stable |
| Epidemic keratoconjunctivitis | Post-membranous conjunctivitis scarring (also beta-hemolytic Streptococcus) |
| Atopic keratoconjunctivitis | Chronic allergic cicatrization |
| Chronic topical medications | Pilocarpine, phospholine iodide, antiviral agents, glaucoma drops |
| Iatrogenic / post-surgical | Following conjunctival procedures |
| Congenital | Rare |
Key clinical point: Symblepharon following a single acute insult (burn, SJS) tends to be stable. Symblepharon in MMP/OCP is typically progressive and requires aggressive systemic immunosuppression.
- The Wills Eye Manual, p. 401; p. 356
- Kanski's Clinical Ophthalmology 10th ed., p. 648
Staging Systems (in MMP/OCP)
Foster's Classification (most widely used)
| Stage | Features |
|---|---|
| I | Chronic conjunctivitis + tear dysfunction + subepithelial fibrosis |
| II | Forniceal shortening (especially inferiorly) |
| III | Symblepharon formation |
| IV | Surface keratinization + cicatricial ankyloblepharon |
Mondino's Classification (based on inferior forniceal depth loss)
| Stage | Forniceal loss |
|---|---|
| I | Up to 25% |
| II | 25-50% |
| III | 50-75% |
| IV | >75% |
- Kanski's Clinical Ophthalmology 10th ed., p. 621-638
Clinical Features
Symptoms
Insidious onset (usually in patients >55 years); bilateral; relapsing-remitting course:
- Dryness, redness, foreign body sensation, burning
- Blepharospasm, photophobia, tearing
- Decreased vision
Ocular Signs
Critical findings:
- Inferior symblepharon - linear conjunctival folds connecting palpebral to bulbar conjunctiva (best seen by pulling down the lower lid during upgaze)
- Foreshortening and tightness of the inferior fornix
- Palpebral conjunctival scarring on eyelid eversion
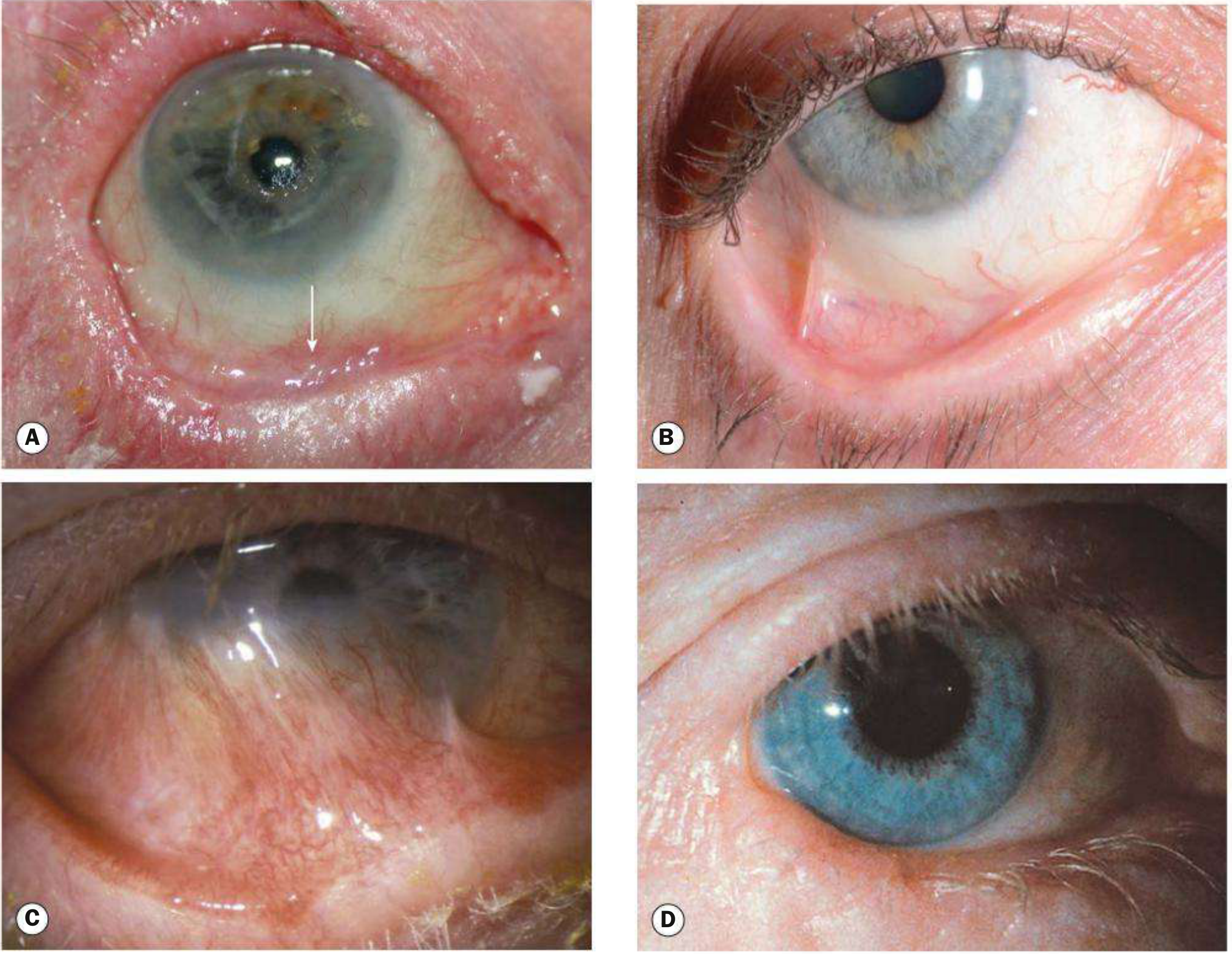
Later/progressive findings:
- Conjunctiva: papillary conjunctivitis, goblet cell destruction → severe dry eye; flattening of plica; caruncular keratinization
- Eyelids: entropion, trichiasis/distichiasis, aberrant lashes, blepharitis, keratinization of lid margin
- Cornea: SPK, epithelial defects, peripheral vascularization, keratinization, conjunctivalization (stem cell failure), stromal ulcers, opacification
- End-stage: total symblepharon, ankyloblepharon (lid-to-lid fusion), limitation of ocular motility, corneal opacification
Systemic Features (in MMP)
-
Mucous membrane blistering: oral (most common - desquamative gingivitis), oropharynx, esophagus, vagina, urethra, anus
-
Oesophageal and laryngeal strictures (severe)
-
Skin lesions (less common, ~25%): tense blisters and erosions of head/neck, groin, extremities
-
The Wills Eye Manual, pp. 354-358
-
Kanski's Clinical Ophthalmology 10th ed., pp. 644-740
Workup
- History - long-term topical medications? past acute systemic illness? recent drug exposure (sulfa, phenytoin, penicillin)?
- Full skin and mucous membrane examination
- Slit-lamp exam - forniceal foreshortening, inferior symblepharon (lower lid traction during upgaze), evert lids for palpebral scarring; check IOP
- Gram stain and culture if secondary bacterial infection suspected
- Conjunctival/mucous membrane biopsy for:
- Direct immunofluorescence: linear IgG, IgA, or C3 at basement membrane zone (confirmatory for MMP)
- Indirect immunofluorescence for circulating antibodies
- Use Michel's transport medium for specimen transport
- Multidisciplinary consults: dermatology, oculoplastics, ENT, gastroenterology, pulmonology
Treatment
Ocular Surface / Supportive
- Preservative-free artificial tears 4-10x/day; high-viscosity ointment at night; autologous serum drops 20-50% q.i.d.
- Scleral lenses to maintain ocular surface integrity
- Moisture chamber goggles/glasses
- Punctal occlusion (if not already scarred)
- Treat blepharitis: lid hygiene, warm compresses, erythromycin ointment t.i.d.; oral doxycycline for anti-inflammatory effect
- Topical ciclosporin or tacrolimus as adjuncts; retinoic acid to reduce keratinization
Medical (Immunosuppression for MMP/OCP)
| Drug | Role | Key Notes |
|---|---|---|
| Dapsone 100-150 mg/day | First-line for mild-moderate disease (~70% respond) | Start 25 mg; increase by 25 mg every 4-7 days; check G-6-PD first; contraindicated in G-6-PD deficiency; monitor CBC weekly (hemolysis risk) |
| Sulfasalazine | Alternative to dapsone if better tolerated | - |
| Antimetabolites (mycophenolate mofetil, methotrexate, azathioprine) | Mild-moderate disease; long-term therapy | Use if dapsone contraindicated/ineffective |
| Cyclophosphamide | Severe or refractory disease | - |
| Systemic steroids (prednisolone 1-1.5 mg/kg) | Rapid disease control; acute exacerbations | Adverse effects limit long-term use; monitor IOP |
| Rituximab / IVIg | Severe/refractory disease | Remission reported with combination regimens |
"Any detectable inflammatory activity should be suppressed." - Kanski's, p. 686
Surgical (only when inflammation is controlled)
- Entropion correction; cryotherapy or electrolysis for trichiasis
- Subconjunctival mitomycin C and/or steroid injection (temporizing measure)
- Mucous membrane grafts (buccal mucosa or amniotic membrane) to reconstruct fornices and prevent further symblepharon
- Contact lens use (with caution) to protect cornea from aberrant lashes
- Keratoprosthesis for end-stage eyes with good posterior segment function (prognosis guarded)
Important: Even seemingly trivial surgical intervention can trigger disease exacerbation in active OCP. Surgery should only be performed under systemic steroid cover when inflammation is absent.
Follow-up
- Every 1-2 weeks during acute exacerbations
- Every 1-6 months during remission
The Wills Eye Manual, pp. 357-358 | Kanski's Clinical Ophthalmology 10th ed., pp. 686-740
This is a shared conversation. Sign in to Orris to start your own chat.