Fast
Parotitis according to s das and manipal in detail
Parotitis - Detailed Account (S Das - A Manual on Clinical Surgery, 13th Edition)
Note: The Manipal textbook of surgery is not available in this library's collection. The answer below is drawn primarily from S Das - A Manual on Clinical Surgery (13th Edition), supplemented by Pye's Surgical Handicraft (22nd ed.) and Tintinalli's Emergency Medicine for completeness.
Anatomy Reminder (S Das)
Classification of Parotitis
1. Acute Suppurative Parotitis
- Infection reaches the gland from the mouth (ascending infection via Stensen's duct)
- Rarely blood-borne
- Predisposing factors: dehydration, poor oral hygiene, debilitated/elderly patients, postoperative state (denied oral fluids), immunosuppression
- Brawny oedematous swelling over the parotid region
- All cardinal signs of inflammation - pain, swelling, redness, warmth, tenderness
- Fluctuation is a late feature - owing to the presence of the strong parotid fascia overlying the gland
- Gentle pressure over the gland causes purulent saliva to exude from the orifice of the duct (important clinical sign - S Das)
- Clinical
- Gentle pressure over the gland and observing Stensen's duct orifice for pus
- Culture of saliva/pus
- Conservative first:
- Correct dehydration
- Obtain saliva by milking the gland - send for culture
- Appropriate antibiotic therapy
- Oral hygiene care
- Sialogue (chewing gum, citrus fruit) to stimulate flow
- If no resolution within 24 hours → Incision and Drainage
- Do not wait for fluctuation - it is a late sign
- Vertical incision from zygomatic arch to angle of jaw, ~1 cm in front of the ear
- Incise only the skin
- Approach parotid fascia by blunt dissection and incise transversely in 2-3 places - to avoid the facial nerve
- Seek pus with sinus forceps
- Loosely approximate skin edges over a corrugated rubber drain brought out inferiorly
2. Viral Parotitis (Mumps - Epidemic Parotitis)
- Paramyxovirus (most common)
- Less commonly: influenza, parainfluenza, coxsackie viruses, echoviruses, lymphocytic choriomeningitis virus, HIV
- Most common in children under 15 years
- Spread by airborne droplets; 2-3 week incubation in upper respiratory tract then systemic spread
- Nonsuppurative condition
- May be unilateral to start with, becomes bilateral within a few days
- Associated with constitutional disturbances and other manifestations of mumps
- Gland is tense and painful; erythema and warmth are notably absent
- No pus expressed from Stensen's duct (distinguishes from suppurative)
- Orchitis - unilateral, 20-30% of post-pubertal males (risk in males ≥8 years)
- Oophoritis - 5% of females
- Pancreatitis
- Aseptic meningitis
- Sensorineural hearing loss
- Myocarditis, polyarthritis, hemolytic anaemia, thrombocytopenia, mastitis

3. Subacute and Chronic Parotitis (S Das)
- May be unilateral or bilateral
- Patient complains of recurrent swelling of the parotid gland
- Swelling is particularly seen during meals (meal-related parotid swelling)
- Gland feels firmer, slightly tender, and rubbery
- Diagnosis confirmed when purulent or watery saliva is ejected from the duct opening on gentle pressure over the gland
4. Recurrent Parotitis of Childhood (Juvenile Recurrent Parotitis)
- Symptoms commence in infancy
- Attacks of painful swelling of the parotid gland, often with fever
- Some patients show allergy to certain foodstuffs
- Usually one gland involved
- Diagnosis confirmed by sialography
Key Clinical Points from S Das - History Taking
| Feature | Significance |
|---|---|
| Sudden bilateral parotid enlargement in dehydrated patient with poor oral hygiene + pain | Acute parotitis |
| Brawny oedematous swelling + all signs of inflammation | Parotid abscess |
| Swelling that increases, becomes tense and painful during meals | Obstruction of duct (stone/stricture) |
| Slow-growing painless tumour for months/years | Pleomorphic adenoma |
| Slow-growing tumour that suddenly becomes rapidly growing and painful | Malignant transformation of mixed tumour |
| Throbbing / excruciating pain + slight swelling + redness | Parotid abscess |
| Watery discharge from sinus during meals | Parotid fistula |
| Generalized enlargement of all major salivary + lacrimal glands | Mikulicz's syndrome |
| Above + dry eyes + generalized arthritis | Sjogren's syndrome |
Examination of the Parotid (S Das)
- Retract cheek with spatula; inspect Stensen's duct orifice opposite upper 2nd molar
- In suppurative parotitis - purulent saliva expressed on gentle pressure
- In malignancy - blood expressed on pressure
- Terminal duct palpated bidigitally (index finger inside mouth, thumb over cheek)
- Not involved in benign tumours
- Involved in malignant growths
- Always test facial nerve integrity in parotid examination
Complication: Auriculotemporal (Frey's) Syndrome (S Das)
- Follows injury to the auriculotemporal nerve while incising for suppurative parotitis
- At meal times: parotid region + cheek become red, hot, painful - then beads of perspiration (gustatory sweating)
- Cutaneous hyperaesthesia over the area (evident while shaving)
Calculus in Parotid
- Rarely formed in the parotid gland - because its secretion is watery (as opposed to submandibular gland which has mucous, viscid secretion)
Differential Diagnosis of Salivary Gland Swelling (Tintinalli)
| Disorder | Onset | Key Features |
|---|---|---|
| Viral parotitis (mumps) | Gradual | Prodromal illness, tense unilateral swelling, no warmth/erythema |
| Suppurative parotitis | Rapid | Buccal swelling, fever, pus from Stensen's duct |
| Masseter space abscess | Gradual | Trismus, dental infection history |
| TB | Gradual | Chronic crusting plaques |
| Sjogren's syndrome | Gradual | Dry mouth, dry eyes, sclerosis |
| Neoplasm | Gradual | No erythema or warmth |
| Sialolithiasis | Gradual | Meal-related swelling, no infection signs |
- S Das - A Manual on Clinical Surgery, 13th Edition, pp. 359-364 (Chapter 25 - The Parotid Gland)
- Pye's Surgical Handicraft, 22nd Edition - Acute Suppurative Parotitis
- Tintinalli's Emergency Medicine: A Comprehensive Study - Viral & Suppurative Parotitis
Regarding Manipal: The Manipal Manual of Surgery is not available in this textbook library. The content above from S Das covers the same clinical topics that Manipal addresses. Key points from Manipal that align with S Das include: dehydration as a predisposing factor, ascending infection route, importance of not waiting for fluctuation before I&D, and Frey's syndrome as a post-drainage complication.
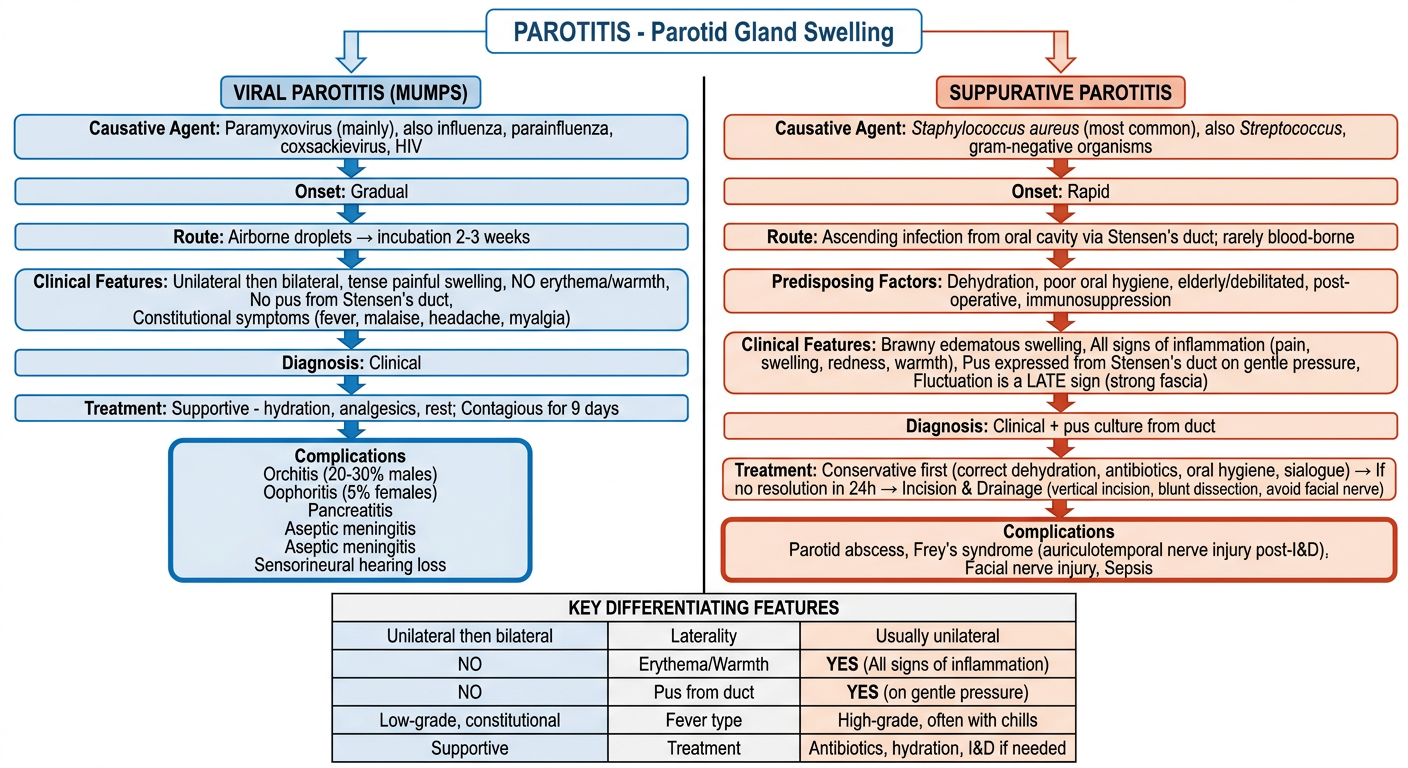
Create a clinical flowchart comparing viral vs suppurative parotitis
A detailed clinical flowchart comparing Viral Parotitis (Mumps) vs Suppurative Parotitis. The flowchart starts at the top with a box labeled "PAROTITIS - Parotid Gland Swelling" then splits into two parallel columns side by side. LEFT COLUMN - VIRAL PAROTITIS (MUMPS) in blue theme: - Causative Agent: Paramyxovirus (mainly), also influenza, parainfluenza, coxsackievirus, HIV - Onset: Gradual - Route: Airborne droplets → incubation 2-3 weeks - Clinical Features: Unilateral then bilateral, tense painful swelling, NO erythema/warmth, No pus from Stensen's duct, Constitutional symptoms (fever, malaise, headache, myalgia) - Diagnosis: Clinical - Treatment: Supportive - hydration, analgesics, rest; Contagious for 9 days - Complications box: Orchitis (20-30% males), Oophoritis (5% females), Pancreatitis, Aseptic meningitis, Sensorineural hearing loss RIGHT COLUMN - SUPPURATIVE PAROTITIS in red/orange theme: - Causative Agent: Staphylococcus aureus (most common), also Streptococcus, gram-negative organisms - Onset: Rapid - Route: Ascending infection from oral cavity via Stensen's duct; rarely blood-borne - Predisposing Factors: Dehydration, poor oral hygiene, elderly/debilitated, post-operative, immunosuppression - Clinical Features: Brawny edematous swelling, All signs of inflammation (pain, swelling, redness, warmth), Pus expressed from Stensen's duct on gentle pressure, Fluctuation is a LATE sign (strong fascia) - Diagnosis: Clinical + pus culture from duct - Treatment: Conservative first (correct dehydration, antibiotics, oral hygiene, sialogue) → If no resolution in 24h → Incision & Drainage (vertical incision, blunt dissection, avoid facial nerve) - Complications box: Parotid abscess, Frey's syndrome (auriculotemporal nerve injury post-I&D), Facial nerve injury, Sepsis At the bottom, a KEY DIFFERENTIATING FEATURES comparison table with rows: Laterality, Erythema/Warmth, Pus from duct, Fever type, Treatment Clean, professional medical flowchart style with clear boxes, arrows, color coding, readable fonts, white background
| Feature | Viral (Mumps) | Suppurative |
|---|---|---|
| Onset | Gradual | Rapid |
| Laterality | Bilateral (unilateral at start) | Usually unilateral |
| Erythema/Warmth | Absent | Present |
| Pus from Stensen's duct | No | Yes (pathognomonic) |
| Fluctuation | Absent | Late sign (don't wait for it) |
| Treatment | Supportive | Antibiotics ± I&D within 24h |