Cscr
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Searching PubMed
"central serous chorioretinopathy" treatment
Central Serous Chorioretinopathy (CSCR)
Overview
Central serous chorioretinopathy (CSCR, also abbreviated CSR) is an idiopathic disorder characterized by a localized serous detachment of the sensory retina at the macula, secondary to leakage from the choriocapillaris through one or more hyperpermeable RPE (retinal pigment epithelium) sites. It is classified within the pachychoroid spectrum of disorders — in eyes with unilateral CSCR, almost two-thirds of fellow eyes show signs of pachychoroid pigment epitheliopathy.
Epidemiology & Risk Factors
| Feature | Detail |
|---|---|
| Typical patient | Young to middle-aged White male |
| Sex ratio | Male:Female = 3:1; women tend to be older at presentation |
| Laterality | Usually unilateral, but can be bilateral |
Risk factors and associations:
- Corticosteroid use (any route — oral, inhaled, nasal spray, topical skin creams, endogenous Cushing syndrome) — strongly linked
- Type A personality / psychological stress
- Systemic hypertension
- Pregnancy (women)
- Lupus (SLE)
- Helicobacter pylori infection
- Renal dialysis
- Sleep apnoea syndrome
- A SNP in the complement factor H gene (chromosome 1) predisposes to the chronic form in White individuals
Presentation
Symptoms:
- Unilateral blurred or dim vision
- Metamorphopsia (distortion) and micropsia (objects appear smaller)
- Central scotoma
- Mild dyschromatopsia (faded colors)
- May be asymptomatic
Signs:
- VA typically 6/9–6/18 (20/30–20/60); improves with a low-strength convex/plus lens (acquired hypermetropia from retinal elevation)
- Round or oval serous detachment of the neurosensory retina at the macula — sloping margins that merge gradually into the attached retina
- Subretinal fluid (clear or turbid); precipitates may be on the posterior retinal surface
- One or more depigmented RPE foci or small PEDs within the detachment
- FAF imaging reveals RPE atrophy/hyperplasia from prior episodes; gravitational tract visible in chronic cases
Fundus Appearance

Investigations
- Amsler grid — documents area of field distortion
- Slit-lamp biomicroscopy — rule out concurrent CNV; examine optic disc for pit
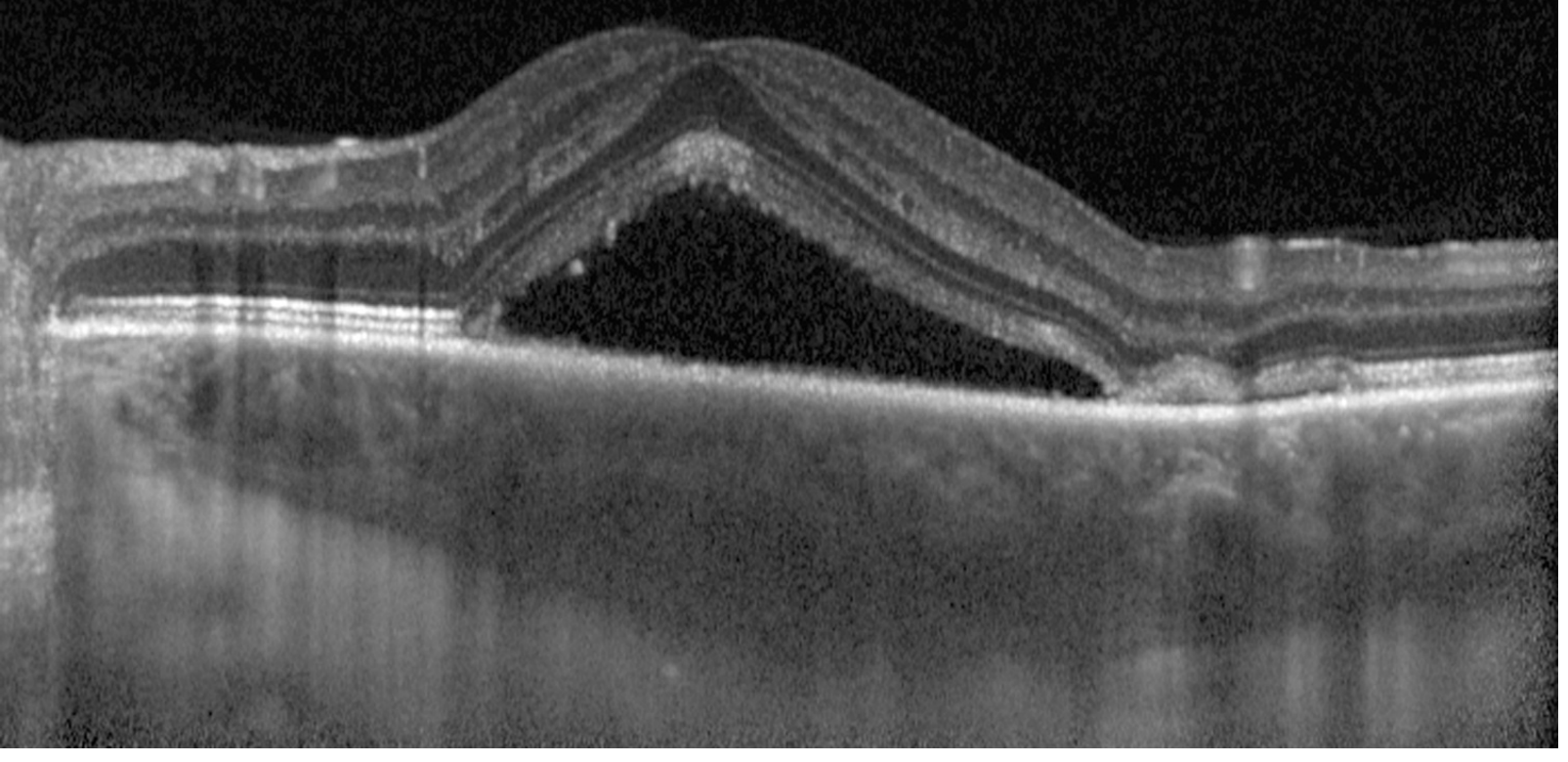
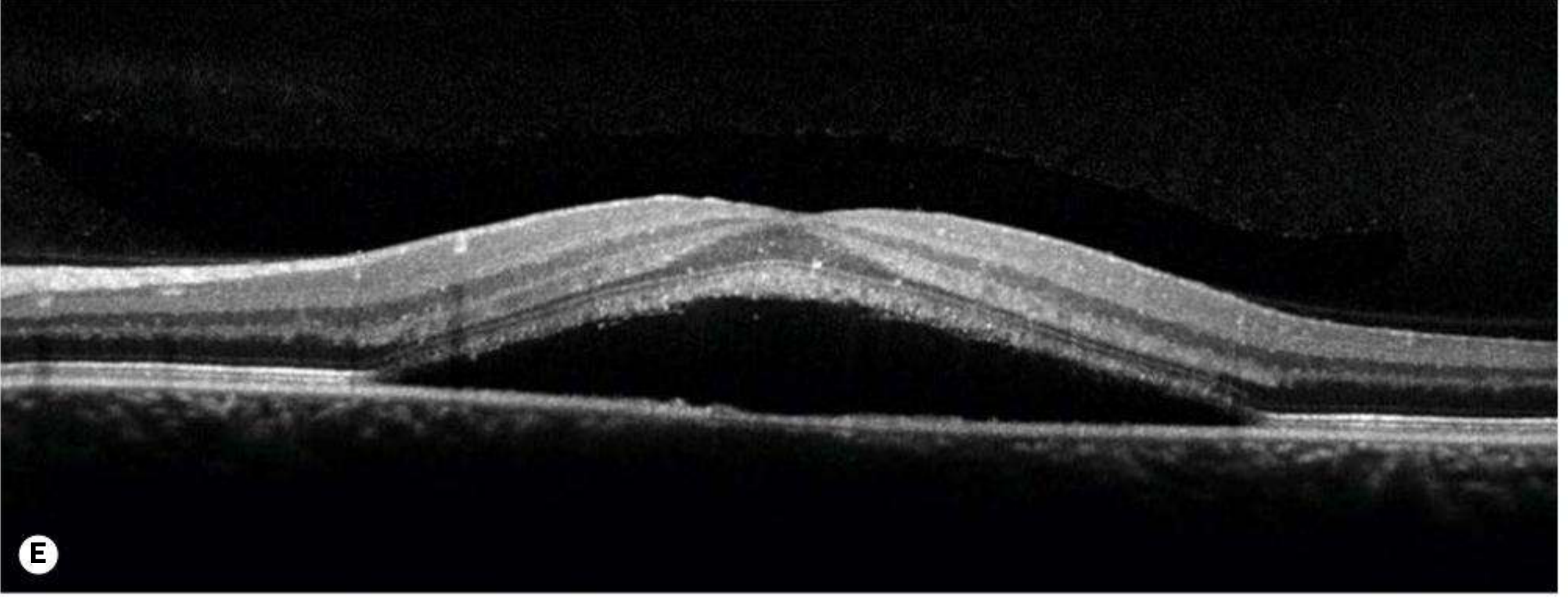
- OCT (enhanced-depth imaging) — gold standard for demonstrating subretinal fluid, PEDs, and choroidal thickening (pachychoroid)
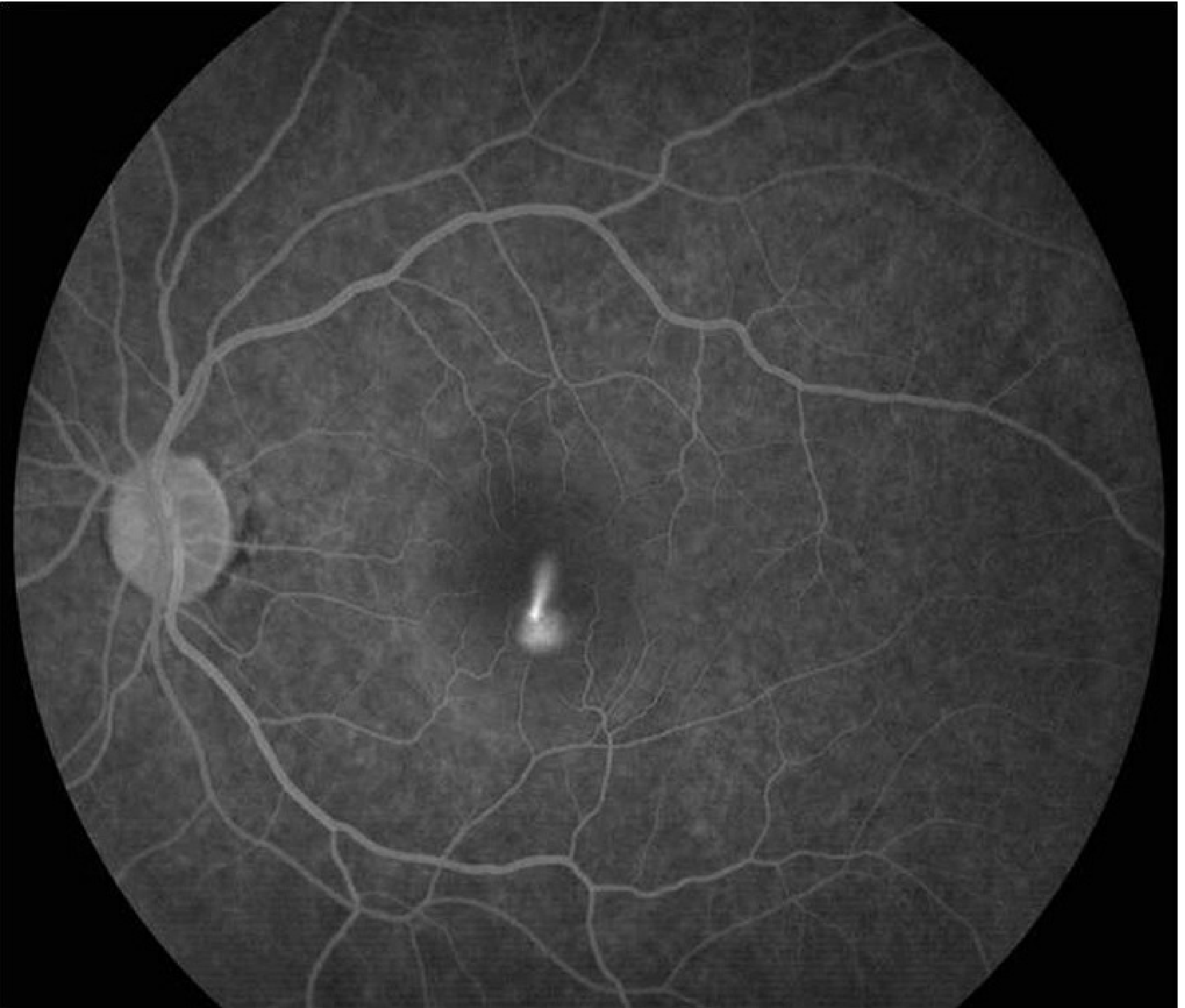
- IVFA (fluorescein angiography) — nearly pathognomonic "smoke-stack" pattern of dye leakage in 10–20% of cases; "ink blot" pattern in others
- ICGA (indocyanine green angiography) — choroidal artery/choriocapillaris filling delays; multifocal hyperfluorescent patches in early phase
- For chronic CSCR: systemic workup including cortisol levels and renal function
Course & Prognosis
| Form | Description |
|---|---|
| Acute | Self-resolving within 3–6 months; near-normal vision in ~80% |
| Recurrent | Up to 50% recurrence rate |
| Chronic | ~15% follow a course >12 months; associated with photoreceptor and RPE degeneration and permanently reduced vision |
Differential Diagnosis
- AMD — patient usually ≥50 years, drusen, often bilateral, may have CNV
- Optic pit — contiguous serous RD with the optic disc
- Rhegmatogenous retinal detachment / macular hole
- Choroidal tumor (hemangioma, melanoma)
- Hypertensive retinopathy
- PED — more distinct, elevated margins (may accompany CSCR or AMD)
- Uveal effusion syndrome, inflammatory choroidal disorders, chronic renal failure
Management
1. Observation
- First-line for acute CSCR — usually self-limited with good visual prognosis.
2. Stop Corticosteroids
- Discontinue all forms if possible (oral, topical, nasal, inhaled).
Key tip (Kanski): All forms of corticosteroid treatment should be discontinued in patients with chronic or recurrent CSCR.
3. Laser Photocoagulation
- May accelerate visual recovery but long-term benefit is unclear and may increase CNV risk.
- Consider when:
- Detachment persists for several months
- Recurrence with residual visual deficit
- Contralateral eye involvement after a prior episode
- Occupational necessity for prompt visual recovery
4. Photodynamic Therapy (PDT)
- Useful for chronic CSCR.
- Half-dose PDT may be considered for rapid SRF resolution in acute CSCR.
5. Mineralocorticoid Receptor Antagonists
- Eplerenone and spironolactone — associated with improved anatomic and visual outcomes in chronic CSCR.
- A 2025 meta-analysis (PMID: 40513762) specifically evaluated both agents for chronic CSCR.
6. Anti-VEGF Therapy
- If choroidal neovascularization (CNV) develops as a complication.
Sources: Kanski's Clinical Ophthalmology 10th ed., p. 617–618 | Wills Eye Manual, §11.15 | Harrison's Principles of Internal Medicine 22E
Cscr for 20 marks
Checking Date & Time
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive 20-mark answer on Central Serous Chorioretinopathy (CSCR):
Central Serous Chorioretinopathy (CSCR)
Definition
Central serous chorioretinopathy (CSCR, also termed CSR) is an idiopathic condition characterized by a localized serous detachment of the neurosensory retina at the macula, secondary to leakage from the choriocapillaris through one or more hyperpermeable RPE (retinal pigment epithelium) sites. It belongs to the pachychoroid disease spectrum.
Epidemiology
- Typically affects young to middle-aged males (20–45 years)
- Male : Female = 3:1 (females tend to present at an older age)
- Usually unilateral, though bilateral cases occur (more common in older patients)
- In unilateral CSCR, ~two-thirds of fellow eyes show signs of pachychoroid pigment epitheliopathy
Pathogenesis
The underlying mechanism involves choroidal hyperpermeability (pachychoroid):
- Dilated outer choroidal (Haller layer) vessels → increased hydrostatic pressure in choriocapillaris
- Impaired RPE pump function → breakdown of the outer blood-retinal barrier
- Fluid accumulates in the subretinal space → neurosensory detachment
Role of corticosteroids: Steroids upregulate mineralocorticoid receptors in the choroid → vasodilatation and increased permeability → this explains the strong link with exogenous and endogenous steroid excess.
Genetic factor: A SNP in the complement factor H gene (chromosome 1) predisposes to the chronic form in White individuals.
Risk Factors / Associations
| Category | Examples |
|---|---|
| Exogenous steroids | Oral, IV, inhaled, nasal spray, topical skin |
| Endogenous steroids | Cushing syndrome, adrenal adenoma |
| Personality / stress | Type A personality, psychological stress |
| Systemic | Hypertension, pregnancy (♀), SLE/lupus |
| Infections | Helicobacter pylori infection |
| Others | Sleep apnoea, renal dialysis |
Clinical Features
Symptoms
- Unilateral blurred or dim vision
- Metamorphopsia (distortion of straight lines)
- Micropsia (objects appear smaller)
- Central scotoma
- Mild dyschromatopsia (faded colours)
- Occasional acquired hypermetropia (retinal elevation shifts focal point forward)
Signs
| Feature | Detail |
|---|---|
| Visual acuity | Typically 6/9–6/18 (20/30–20/60); improves with +1.00 D convex lens |
| Fundus | Round/oval serous detachment of neurosensory retina at macula; sloping margins merging gradually with attached retina |
| Subretinal fluid | Clear (early) or turbid; precipitates on posterior retinal surface |
| RPE changes | Depigmented foci/small PEDs within the detachment; RPE atrophy/hyperplasia at sites of prior episodes |
| Chronic form | Gravitational tract (fluid tracks inferiorly); can progress to bullous CSCR |
Fundus Photograph
Investigations
1. Amsler Grid
Confirms metamorphopsia and relative central scotoma corresponding to the neurosensory detachment.
2. Slit-Lamp Biomicroscopy (with 90D/contact lens)
- Identifies the macular serous detachment
- Rules out CNV or optic disc pit
3. Optical Coherence Tomography (OCT) — Investigation of Choice
- Optically empty (black) space beneath elevated neurosensory retina = subretinal fluid
- May show associated RPE detachments (PEDs)
- Enhanced depth imaging (EDI-OCT): demonstrates choroidal thickening (pachychoroid) — key diagnostic feature
4. Fundus Fluorescein Angiography (FFA/IVFA)
Two pathognomonic patterns of dye leakage:
| Pattern | Description | Frequency |
|---|---|---|
| "Ink blot" | Early hyperfluorescent spot that gradually enlarges | More common |
| "Smoke stack" | Vertical column of dye that mushrooms at top | 10–20% of cases |
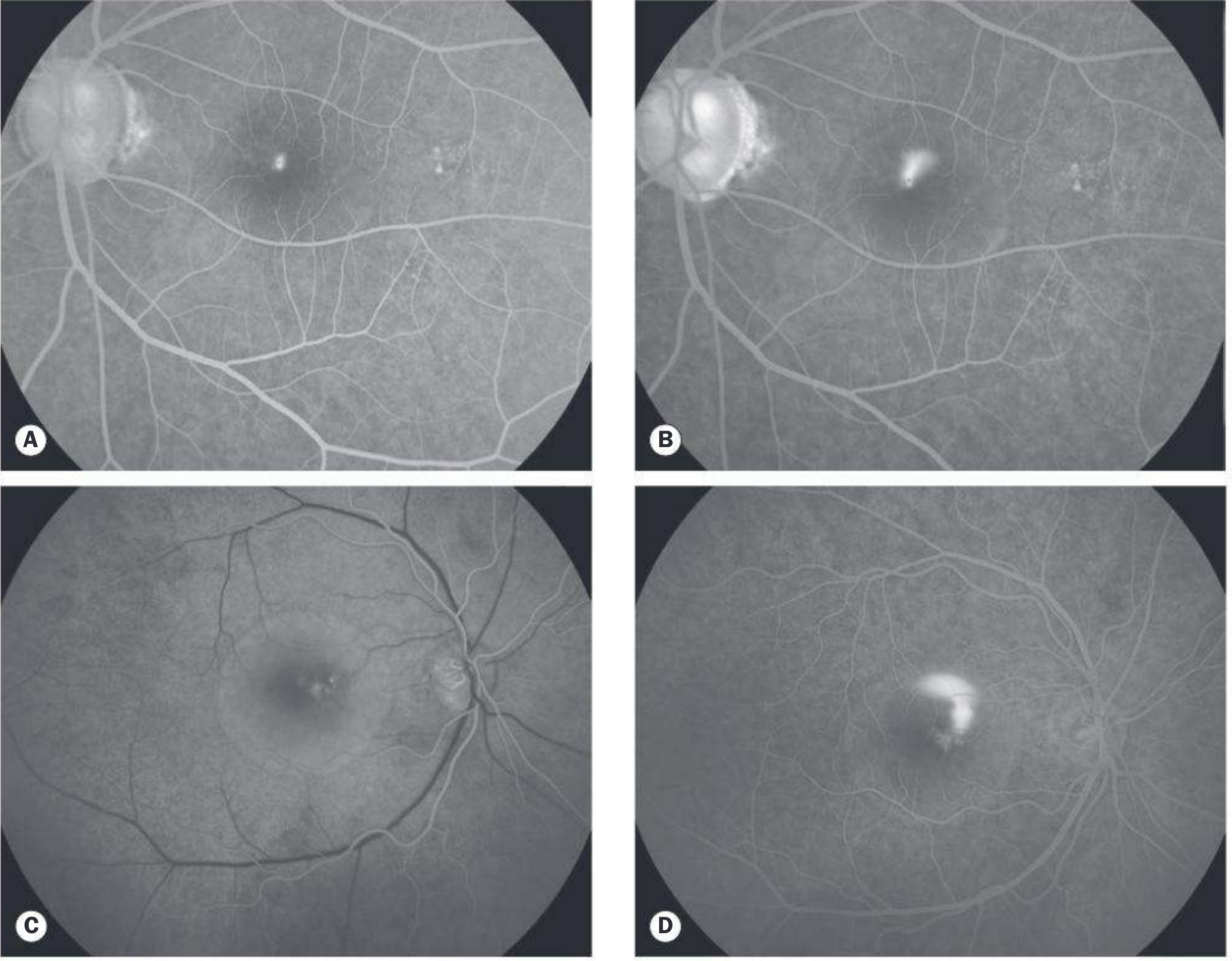
5. Indocyanine Green Angiography (ICGA)
- Early phase: dilated/compromised choroidal vessels; choriocapillaris filling delay
- Mid-phase: multifocal hyperfluorescent patches from choroidal hyperpermeability
- Subclinical foci commonly visible; essential for guiding PDT
6. Fundus Autofluorescence (FAF)
- Hypoautofluorescence at leakage site and old lesions (RPE loss)
- Hyperautofluorescence = RPE lipofuscin accumulation
- Reveals gravitational tracts in chronic cases
7. Systemic Workup (chronic CSCR)
- Serum/24-hour urinary cortisol (exclude Cushing syndrome)
- Renal function tests
Course & Prognosis
| Form | Time Course | Outcome |
|---|---|---|
| Acute | Self-resolves in 3–6 months | Near-normal vision in ~80% |
| Recurrent | Episodes with incomplete recovery | Up to 50% recurrence rate |
| Chronic | Persists >12 months (~15% of patients) | Gradual photoreceptor and RPE degeneration; permanent visual loss |
Complications: CMO (cystoid macular oedema), macular neovascularization (MNV), RPE tears (may occur spontaneously or after treatment).
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| AMD | Age ≥50, drusen, bilateral, may have CNV |
| Optic pit | Serous RD contiguous with optic disc |
| Rhegmatogenous RD | Retinal break identifiable |
| Choroidal tumour (hemangioma/melanoma) | Elevated choroidal mass on USG |
| Hypertensive retinopathy | Hypertension, AV changes |
| PED | More distinct/steep margins; RPE elevated |
| Vogt-Koyanagi-Harada (VKH) | Bilateral, inflammatory, systemic features |
Management
1. Observation (First-line for Acute CSCR)
- Most acute cases resolve spontaneously within 3–6 months
- Monitor with OCT; reassure patient
2. Eliminate Risk Factors
- Stop all corticosteroids (systemic, topical, nasal, inhaled) — mandatory in chronic/recurrent cases
Key tip: "All forms of corticosteroid treatment should be discontinued if possible in patients with chronic or recurrent CSCR." — Kanski
3. Laser Photocoagulation
- Conventional laser: May accelerate visual recovery but long-term benefit uncertain; carries risk of CNV formation
- Subthreshold micropulse diode laser to the RPE leakage site: Better safety profile — good results in several studies; significantly less retinal damage on OCT
- Indications:
- Persistence >3–4 months
- Recurrence with residual visual deficit
- Occupational necessity for prompt visual recovery
- Contralateral eye involvement after prior vision loss
4. Photodynamic Therapy (PDT) with Verteporfin
- Treatment of choice for chronic CSCR
- Half/reduced dose PDT (30–50% standard dose + 50% light intensity): Complete SRF resolution including severe chronic cases; significantly lower risk of choroidal ischaemia than full-dose regimens
- Half-dose PDT may also accelerate resolution in acute CSCR
5. Mineralocorticoid Receptor Antagonists
- Spironolactone (40 mg BD) and Eplerenone — associated with faster SRF resorption and improved visual outcomes in both acute and chronic CSCR
- Mechanism: block mineralocorticoid receptors in choroidal vasculature → reduce hyperpermeability
- Supported by a 2025 systematic review and meta-analysis (PMID: 40513762)
6. Anti-VEGF Therapy
- Bevacizumab alone is not effective in pure CSCR (no CNV)
- Indicated if macular neovascularization (MNV/CNV) develops as a complication
- Often used in combination with PDT
7. Others (Limited Evidence)
- Aspirin, beta-blockers, mifepristone — case reports suggest benefit; controlled data lacking
Summary Table
| Feature | Detail |
|---|---|
| Definition | Serous detachment of neurosensory retina at macula |
| Pathology | Pachychoroid → choriocapillaris hyperpermeability → RPE dysfunction |
| Typical patient | Young adult male, 20–45 years |
| Key symptom | Metamorphopsia + micropsia + central scotoma |
| Key sign | Serous macular detachment; improved VA with +1 D lens |
| Best investigation | OCT (subretinal fluid + choroidal thickening) |
| Pathognomonic FA | "Ink blot" / "smoke stack" leakage pattern |
| Acute treatment | Observation; stop steroids |
| Chronic treatment | Reduced-dose PDT; mineralocorticoid antagonists |
| Complication | MNV, RPE degeneration, permanent vision loss |
Sources: Kanski's Clinical Ophthalmology 10th ed. (pp. 617–620) | Wills Eye Manual §11.15 | Harrison's Principles of Internal Medicine 22E
Eales disease
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Searching PubMed
"Eales disease" retina
Here is a comprehensive answer on Eales Disease suitable for a 20-mark question:
Eales Disease
Definition
Eales disease is an idiopathic occlusive peripheral periphlebitis (inflammation of retinal veins and perivascular tissue) predominantly affecting young South Asian males. It is characterized by three overlapping stages: inflammatory → occlusive → proliferative (neovascular), and is diagnosed principally by clinical examination. It is a diagnosis of exclusion after ruling out other causes of retinal vasculitis.
Named after British physician Henry Eales (1852–1913), who described recurrent vitreous haemorrhage in young men.
Epidemiology
- Most common in young males aged 20–35 years
- Particularly prevalent in the Indian subcontinent (South Asia) — important cause of visual morbidity there
- Rare in White populations
- Usually bilateral, though often asymmetrical
Aetiology & Pathogenesis
The exact aetiology is unknown (idiopathic), but several hypotheses exist:
1. Tubercular Hypersensitivity (Most favoured)
- Mycobacterium tuberculosis protein hypersensitivity → immune-mediated retinal periphlebitis
- Evidence: tuberculin skin test positivity, positive QuantiFERON-TB, PCR for M. tuberculosis DNA in vitreous samples in some cases
- However, evidence is conflicting — some patients may have active tubercular vasculitis, others only hypersensitivity
2. Oxidative Stress
- Increased free radicals and decreased antioxidant enzymes demonstrated in patients
3. Autoimmune Mechanism
- Molecular mimicry: retinal S-antigen may trigger autoimmune response
4. Other associations
- Helicobacter pylori, focal sepsis, metabolic disorders — reported but unconfirmed
Pathological sequence:
Perivenous inflammatory infiltrate → endothelial damage → venous occlusion → retinal ischaemia → VEGF upregulation → neovascularization → vitreous haemorrhage
Stages of Eales Disease
| Stage | Pathology | Features |
|---|---|---|
| Stage I — Inflammatory | Periphlebitis of peripheral retinal veins | Venous sheathing, perivascular infiltrates, superficial haemorrhages |
| Stage II — Occlusive | Branch retinal vein occlusion (BRVO) | Retinal ischaemia, capillary non-perfusion, microaneurysms, vascular shunts |
| Stage III — Proliferative | Retinal neovascularization | New vessels at junction of perfused/non-perfused retina; recurrent vitreous haemorrhage |
(Stages overlap and may coexist in different areas of the same fundus)
Clinical Features
Symptoms
- Floaters — due to vitreous haemorrhage
- Sudden painless visual loss — vitreous haemorrhage (most common presentation)
- Positive family history may be present
- Systemic neurological features have been reported (rare)
Signs
Anterior Segment
- Mild anterior uveitis often present
- Keratic precipitates (fine)
- Flare and cells in anterior chamber
Posterior Segment (Fundus)
The condition is typically bilateral but asymmetrical:
Inflammatory stage:
- Peripheral periphlebitis — venous sheathing (white cuffing around veins), superficial retinal haemorrhages, cotton-wool spots
- Pigmented chorioretinal scars at sites of resolved lesions
Occlusive stage:
- Branch retinal vein occlusion (BRVO) of peripheral veins
- Peripheral capillary non-perfusion
- Microaneurysms, venous tortuosity, vascular shunts
Proliferative stage:
- Peripheral retinal neovascularization at the junction of perfused and non-perfused retina
- Disc new vessels (neovascularization of disc — NVD) can sometimes develop
- Recurrent vitreous haemorrhage — occurs in ~one-third of eyes; typically limited, absorbs over weeks but can persist
Macular involvement: Rare; carries poor prognosis
Fundus Photographs


Complications
- Tractional retinal detachment (from fibrovascular proliferation)
- Macular epiretinal membrane
- Neovascular glaucoma (NVG) — from anterior segment neovascularization
- Cataract
- Persistent vitreous haemorrhage
- Permanent visual loss
Investigations
Ocular
| Investigation | Findings |
|---|---|
| FFA (Fundus Fluorescein Angiography) | Peripheral capillary non-perfusion, retinal vasculitis, neovascularization; wide-field imaging especially helpful |
| OCT | Useful for macular assessment — macular oedema, ERM |
| B-scan USG | When vitreous haemorrhage obscures fundus — detect TRD |
Systemic (to rule out other causes)
| Test | Purpose |
|---|---|
| Mantoux / Tuberculin skin test | TB hypersensitivity |
| QuantiFERON-TB Gold | Latent TB |
| Chest X-ray / HRCT chest | Active TB, sarcoidosis |
| Serum ACE, calcium | Sarcoidosis |
| FBC, peripheral smear, Hb electrophoresis | Haemoglobinopathy (sickle cell) |
| VDRL/TPHA | Syphilis |
| ANA, ANCA | Autoimmune vasculitis |
| Serum glucose, lipids | Systemic metabolic disorders |
| HIV serology | Viral retinitis |
Key point: Eales disease is a diagnosis of exclusion — all secondary causes of retinal vasculitis and peripheral neovascularization must be ruled out.
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Sarcoidosis | "Candlewax" exudates; raised ACE; systemic features |
| Tuberculosis | Positive Mantoux/QuantiFERON; chest X-ray changes |
| Syphilis | Positive VDRL/TPHA; multisystem involvement |
| Sickle cell retinopathy | Hb electrophoresis; sea-fan neovascularization |
| Pars planitis | "Snowbanking" at pars plana; younger age group |
| Behçet disease | Occlusive arteritis; oral/genital ulcers; uveitis |
| BRVO | Usually single vessel, not bilateral/peripheral |
| Diabetic retinopathy | Central/posterior distribution; systemic DM |
| Multiple sclerosis | Neurological signs; MRI changes |
Management
1. Corticosteroids (Inflammatory Stage)
- Periocular, systemic, topical and intravitreal steroids are helpful in the inflammatory/active periphlebitis stage
- Reduce venous inflammation and prevent progression to occlusion
2. Anti-Tubercular Treatment (ATT)
- Controversial but strongly advocated by many authorities, especially in endemic regions
- Indications to consider ATT (combined with steroids):
- Strongly positive tuberculin skin test or QuantiFERON
- Severe ocular inflammatory signs
- To prevent reactivation of prior TB infection
- Standard 4-drug ATT regimen: Isoniazid + Rifampicin + Pyrazinamide + Ethambutol
3. Scatter (Panretinal) Photocoagulation (PRP)
- Treatment of choice for non-perfused retina — reduces neovascular stimulus (VEGF)
- Applied to areas of capillary non-perfusion to induce regression of new vessels
- Cryotherapy is an alternative if laser is not accessible
4. Intravitreal Anti-VEGF Agents
- Commonly used in the neovascular/proliferative stage
- Induces regression of retinal new vessels
- May be used as adjunct before vitrectomy to reduce intraoperative bleeding
5. Vitrectomy
Indicated for:
- Persistent non-clearing vitreous haemorrhage
- Tractional retinal detachment
- Macular epiretinal membrane
Prognosis
- Generally good in the majority of cases — most patients retain useful vision
- Worse prognosis with:
- Macular involvement
- Dense persistent vitreous haemorrhage
- Tractional retinal detachment
- Neovascular glaucoma
Summary
| Feature | Detail |
|---|---|
| Definition | Idiopathic occlusive peripheral periphlebitis |
| Typical patient | Young South Asian male, 20–35 years |
| Laterality | Bilateral, asymmetrical |
| Aetiology | Idiopathic; TB hypersensitivity most favoured |
| Stages | Inflammatory → Occlusive → Proliferative |
| Key symptom | Sudden painless visual loss / floaters (vitreous haemorrhage) |
| Key sign | Peripheral periphlebitis → capillary non-perfusion → neovascularization |
| Key investigation | FFA (wide-field) — non-perfusion and NVE |
| Diagnosis | Exclusion of other causes |
| Treatment | Steroids (inflammatory) + PRP (proliferative) + ATT (if TB suspected) + Anti-VEGF + Vitrectomy (complications) |
| Prognosis | Good in majority |
Sources: Kanski's Clinical Ophthalmology 10th ed. (pp. 570–571) | Wills Eye Manual | Kanski's Clinical Ophthalmology §13 (Retinal Vascular Disease)
This is a shared conversation. Sign in to Orris to start your own chat.