OSA in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
"obstructive sleep apnea" AND management
Reading File
Reading File
Finding Sources
Searching PubMed
"obstructive sleep apnea" AND treatment
Reading File
Finding Sources
Searching PubMed
"sleep apnea" AND "hypoglossal nerve stimulation"
Reading File
Reading File
Reading File
Finding Sources
Searching PubMed
"obstructive sleep apnea" AND "tirzepatide OR semaglutide"
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading Article
PMID: 38912654
OBSTRUCTIVE SLEEP APNEA (OSA)
20-Mark Comprehensive Answer | RGUHS ENT
1. DEFINITION
Obstructive Sleep Apnea (OSA) is a sleep-related breathing disorder characterized by repetitive episodes of partial or complete upper airway obstruction during sleep, resulting in oxygen desaturation and sleep fragmentation, despite continued respiratory effort.
- Each apnea/hypopnea episode lasts at least 10 seconds
- Commonly accompanied by oxygen desaturation of 3-4%
- Terminated by brief, unconscious arousals from sleep
- Cummings Otolaryngology Head and Neck Surgery, 7th ed., Ch. 15
2. EPIDEMIOLOGY
| Parameter | Data |
|---|---|
| Prevalence (adults) | 2-4% in women; 4-9% in men |
| Peak age | Middle-aged adults (40-65 years) |
| Male:Female ratio | ~2:1 (gap narrows post-menopause) |
| Obesity correlation | 70% of OSA patients are obese |
| Underdiagnosis | Especially in women (present atypically) |
- Young T et al. (1993, NEJM) - Wisconsin Sleep Cohort Study: First population-based prevalence data (Scott-Brown's Otorhinolaryngology H&N Surgery, Vol 2)
- Prevalence of severe OSA in children ~1%, peak between 3-6 years (Scott-Brown's Vol 2, Ch. 27)
3. CLASSIFICATION / SEVERITY
Based on Apnea-Hypopnea Index (AHI):
┌─────────────────────────────────────────────────────┐
│ AHI SEVERITY CLASSIFICATION │
│ (AASM Criteria) │
├─────────────────────┬───────────────────────────────┤
│ Normal │ AHI < 5 events/hour │
│ Mild OSA │ AHI 5–14 events/hour │
│ Moderate OSA │ AHI 15–30 events/hour │
│ Severe OSA │ AHI > 30 events/hour │
└─────────────────────┴───────────────────────────────┘
Indexes of Sleep-Disordered Breathing (Table 15.2, Cummings):
| Index | Definition |
|---|---|
| Apnea Index (AI) | Apneas per hour of sleep |
| Hypopnea Index (HI) | Hypopneas per hour of sleep |
| AHI | Apneas + Hypopneas per hour |
| RERA Index | Respiratory effort-related arousals per hour |
| RDI | Apneas + Hypopneas + RERAs per hour |
4. PATHOPHYSIOLOGY
Four Key Phenotypic Traits (Cummings, Fig. 15.1):
┌─────────────────────────────────────────────────────────────────────┐
│ PATHOPHYSIOLOGY OF OSA - FOUR PHENOTYPES │
│ │
│ 1. IMPAIRED UPPER AIRWAY ANATOMY │
│ └── Narrow/collapsible pharynx │
│ (obesity, soft tissue hypertrophy, retrognathia) │
│ ↓ │
│ 2. INADEQUATE UPPER AIRWAY DILATOR MUSCLE RESPONSE │
│ └── Genioglossus fails to maintain patency during sleep │
│ (reduced neuromuscular compensation) │
│ ↓ │
│ 3. LOW AROUSAL THRESHOLD │
│ └── Awakens too easily → prevents deep sleep → unstable │
│ pharyngeal dilator response │
│ ↓ │
│ 4. HIGH LOOP GAIN (Unstable Respiratory Control) │
│ └── Oversensitive to CO₂ → over-ventilation → airway collapse │
│ │
│ RESULT: Repetitive pharyngeal collapse → Apnea/Hypopnea │
└─────────────────────────────────────────────────────────────────────┘
Anatomic Sites of Obstruction (Fujita Classification):
- Type I - Retropalatal collapse only
- Type II - Both retropalatal AND retrolingual collapse
- Type III - Retrolingual collapse only
Studies show: 100% retropalatal + 77% retrolingual obstruction in confirmed OSA patients (Steinhart et al., 2000).
Critical Closing Pressure (Pcrit):
- OSA patients: Pcrit above atmospheric pressure
- Normal individuals: Pcrit below -5 cm H₂O
- Genioglossus is the most important airway dilator muscle
5. ETIOLOGY / RISK FACTORS
┌─────────────────────────────────────────────────────┐
│ RISK FACTORS FOR OSA │
├─────────────────────────────────────────────────────┤
│ MODIFIABLE │ NON-MODIFIABLE │
│ ───────────────── │ ─────────────────────────── │
│ • Obesity (BMI>30) │ • Age (>40 years) │
│ • Alcohol use │ • Male sex │
│ • Sedative use │ • Positive family history │
│ • Nasal congestion │ • Craniofacial: retrognathia│
│ • Smoking │ micrognathia │
│ • Supine sleeping │ • Racial: Asian patients │
│ • Hypothyroidism │ (smaller craniofacial) │
│ • Acromegaly │ • Postmenopause (females) │
└─────────────────────┴──────────────────────────────┘
6. CLINICAL FEATURES
Nocturnal Symptoms:
- Loud snoring (most common partner complaint)
- Witnessed apnea, choking, gasping episodes
- Restless sleep, night sweats
- Nocturia, nocturnal enuresis
- Nocturnal headaches
Daytime Symptoms (Box 15.1, Cummings):
- Excessive daytime somnolence (present in ~50%)
- Morning fatigue, unrefreshing sleep
- Memory loss, decreased cognitive function
- Depression, personality changes
- Decreased libido and impotence
Physical Examination Findings (Box 15.4, Cummings):
Nasal: Septal deviation, turbinate hypertrophy, nasal valve collapse, adenoid hypertrophy
Oropharyngeal: Large soft palate, tonsillar hypertrophy, macroglossia, posterior pharyngeal wall banding
Hypopharyngeal: Lateral pharyngeal wall collapse, omega-shaped epiglottis, lingual tonsillar hypertrophy, retrognathia/micrognathia
7. DIAGNOSIS
FLOWCHART: DIAGNOSTIC APPROACH TO OSA
┌──────────────────────────────────┐
│ CLINICAL SUSPICION OF OSA │
│ (Snoring + EDS + witnessed apnea)│
└──────────────┬───────────────────┘
│
┌──────────────▼───────────────────┐
│ SCREENING TOOLS │
│ • Epworth Sleepiness Scale (ESS) │
│ Score >10 = suspicious │
│ • STOP-BANG Questionnaire │
│ Score ≥5 = High risk │
│ • Berlin Questionnaire │
└──────────────┬───────────────────┘
│
┌────────────────────┼────────────────────┐
│ │ │
┌─────────▼──────┐ ┌─────────▼──────┐ ┌────────▼───────┐
│ PHYSICAL EXAM │ │ FLEXIBLE │ │ INVESTIGATIONS│
│ BMI, BP, neck │ │ NASOENDOSCOPY │ │ CBC, TFT, │
│ circumference │ │ Mullär maneuver│ │ blood glucose │
│ Mallampati score│ │ DISE │ │ ECG │
└────────────────┘ └────────────────┘ └────────────────┘
│
┌──────────────▼───────────────────┐
│ POLYSOMNOGRAPHY (PSG) │
│ "Gold Standard Diagnosis" │
│ (In-lab or Home Sleep Apnea │
│ Test - HSAT) │
└──────────────┬───────────────────┘
│
┌────────────────────┼────────────────────┐
│ │ │
┌─────────▼──────┐ ┌─────────▼──────┐ ┌────────▼───────┐
│ AHI < 5 │ │ AHI 5-14 │ │ AHI ≥ 15 │
│ (Normal or │ │ (Mild) + │ │ (Moderate/ │
│ re-evaluate) │ │ symptoms/ │ │ Severe OSA) │
│ │ │ comorbidities │ │ │
└────────────────┘ └────────────────┘ └────────────────┘
Epworth Sleepiness Scale (ESS):
(Fig. 15.2, Cummings Otolaryngology)
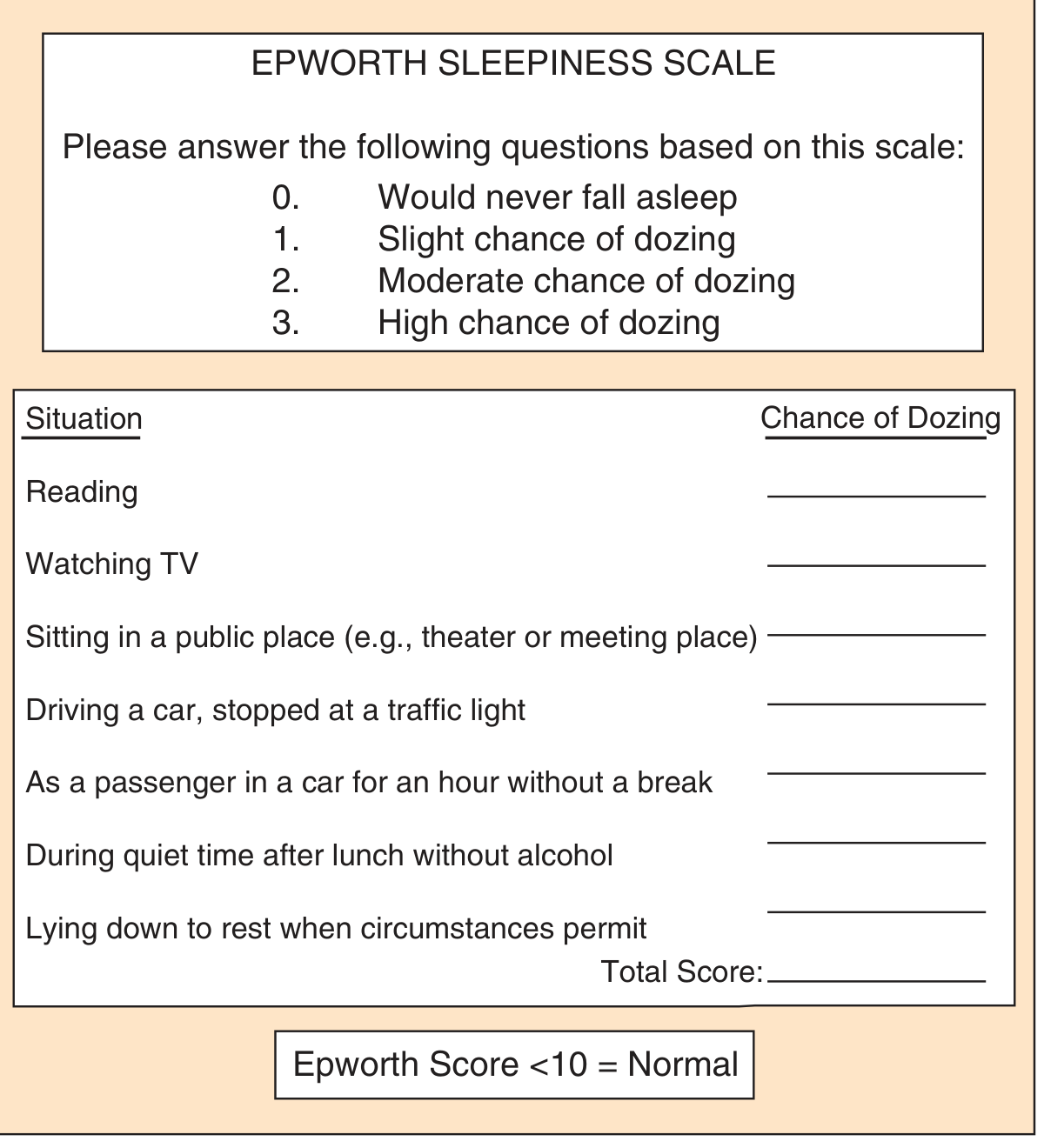
- Score 0-10: Normal
- Score >10: Excessive daytime sleepiness - investigate for OSA
STOP-BANG Questionnaire (Box 15.2, Cummings):
| Letter | Question |
|---|---|
| S | Do you Snore loudly? |
| T | Do you feel Tired/fatigued during day? |
| O | Has anyone Observed you stop breathing during sleep? |
| P | Do you have high blood Pressure? |
| B | BMI > 35 kg/m²? |
| A | Age ≥ 50 years? |
| N | Neck circumference >40 cm (F) or >43 cm (M)? |
| G | Are you male (Gender)? |
- Score ≥ 3: High risk; Score 5-8: High probability of moderate-severe OSA
Polysomnography (PSG) - Gold Standard:
Records: EEG, EOG, EMG, airflow, respiratory effort, pulse oximetry, ECG, body position, limb movements
Diagnostic criteria (AASM ICSD-3):
- AHI ≥ 5 + symptoms/comorbidities, OR
- AHI ≥ 15 (regardless of symptoms)
8. DRUG-INDUCED SLEEP ENDOSCOPY (DISE)
A newer technique using fiberoptic nasopharyngoscopy during pharmacologically-induced sleep to dynamically evaluate sites of collapse. A meta-analysis found DISE changed surgical planning in >50% of cases, especially for hypopharyngeal/laryngeal structures. (Cummings, 7th ed.)
Fiberoptic View of Hypopharyngeal Collapse (Müller Maneuver):
(From Cummings Otolaryngology, Fig. 15.6)

9. COMPLICATIONS / CONSEQUENCES
┌──────────────────────────────────────────────────────────────┐
│ CONSEQUENCES OF UNTREATED OSA │
├────────────────────┬─────────────────────────────────────────┤
│ CARDIOVASCULAR │ Systemic hypertension (most common) │
│ │ Pulmonary hypertension │
│ │ Arrhythmias (atrial fibrillation) │
│ │ Coronary artery disease │
│ │ Congestive heart failure │
│ │ Stroke / TIA │
│ │ 3× risk of fatal CV events │
├────────────────────┼─────────────────────────────────────────┤
│ METABOLIC │ Insulin resistance / Type 2 DM │
│ │ Metabolic syndrome │
│ │ GERD (higher prevalence) │
├────────────────────┼─────────────────────────────────────────┤
│ NEUROCOGNITIVE │ Impaired attention, working memory │
│ │ Executive dysfunction │
│ │ Depression, mood changes │
├────────────────────┼─────────────────────────────────────────┤
│ MORTALITY │ AI >20: 63% survival at 8 years │
│ │ vs 96% in treated patients │
│ │ 2.5× risk of motor vehicle accidents │
└────────────────────┴─────────────────────────────────────────┘
- He et al. (retrospective study, cited in Cummings); Goldman-Cecil Medicine, 27th ed.
10. MANAGEMENT
FLOWCHART: MANAGEMENT OF OSA
┌────────────────────────────────────────────────────────────────┐
│ CONFIRMED OSA ON PSG │
└──────────────────────────────┬─────────────────────────────────┘
│
┌──────────────────┼──────────────────┐
│ │ │
┌────────▼────────┐ ┌──────▼──────┐ ┌───────▼───────┐
│ MILD OSA │ │ MODERATE │ │ SEVERE OSA │
│ (AHI 5-14) │ │ OSA │ │ (AHI ≥ 30) │
│ │ │ (AHI 15-30) │ │ │
└────────┬────────┘ └──────┬──────┘ └───────┬───────┘
│ │ │
┌────────▼────────┐ │ ┌───────▼───────┐
│ Lifestyle + │ │ │ CPAP (first │
│ Positional Rx │ │ │ line) ALWAYS │
│ ± OAT if CPAP │ │ │ │
│ refused │ │ └───────┬───────┘
└─────────────────┘ ┌──────▼──────┐ │
│ CPAP First │ ┌────────▼──────┐
│ Line │ │ CPAP FAILURE/ │
│ + Lifestyle │ │ REFUSAL? │
└─────────────┘ └────────┬──────┘
│
┌───────────────────┼──────────────────┐
│ │ │
┌─────────▼──────┐ ┌────────▼──────┐ ┌───────▼──────┐
│ ORAL APPLIANCE│ │ POSITIONAL │ │ SURGERY │
│ THERAPY (OAT) │ │ THERAPY │ │ (staged) │
│ MAD/MRD │ │ │ │ │
└────────────────┘ └───────────────┘ └──────────────┘
A. Lifestyle/Conservative Measures:
- Weight loss (10% weight reduction → ~26% AHI reduction)
- Avoid alcohol, sedatives, smoking
- Positional therapy (avoid supine position)
- Regular exercise
B. Non-Surgical: CPAP (Continuous Positive Airway Pressure)
First-line treatment for moderate-severe OSA
- Acts as a "pneumatic splint" maintaining airway patency
- Reduces AHI, blood pressure (~10 mmHg reduction), CV events
- Improves neurocognitive function and quality of life
- Variants: Auto-CPAP (APAP), BiPAP/BPAP for complex OSA
C. Oral Appliance Therapy (OAT):
- Mandibular Advancement Device (MAD)/Mandibular Repositioning Device
- Alternative for mild-moderate OSA, CPAP-intolerant patients
- Mechanism: Protrudes mandible forward, enlarges pharyngeal airway
D. Surgical Options (Box 15.7, Cummings):
┌──────────────────────────────────────────────────────────────────┐
│ SURGICAL TREATMENT OPTIONS (STAGED) │
├──────────────────────┬───────────────────────────────────────────┤
│ NASAL SURGERY │ Septoplasty │
│ │ Inferior turbinate reduction │
├──────────────────────┼───────────────────────────────────────────┤
│ PALATAL SURGERY │ UPPP (Uvulopalatopharyngoplasty) │
│ (Retropalatal) │ Laser-assisted UP (LAUP) │
│ │ Palatal implants (Pillar procedure) │
│ │ Lateral pharyngoplasty │
│ │ Expansion sphincter pharyngoplasty │
├──────────────────────┼───────────────────────────────────────────┤
│ TONGUE BASE / │ Tongue base reduction (coblation, │
│ HYPOPHARYNGEAL │ radiofrequency) │
│ │ Lingual tonsillectomy │
│ │ TORS (Transoral Robotic Surgery) │
│ │ Genioglossus advancement │
│ │ Hyoid suspension (hyoidthyroidpexy) │
├──────────────────────┼───────────────────────────────────────────┤
│ SKELETAL SURGERY │ Maxillomandibular advancement (MMA) │
│ │ Distraction osteogenesis │
├──────────────────────┼───────────────────────────────────────────┤
│ LAST RESORT │ Tracheostomy (definitive, curative) │
└──────────────────────┴───────────────────────────────────────────┘
Surgical Indications (Box 15.6, Cummings):
- AHI >5 and <14 with symptoms or comorbidities
- AHI ≥15
- Oxyhemoglobin desaturation <90%
- Failed or refused medical therapy
- Medically stable for recommended procedure
E. Hypoglossal Nerve Stimulation (HNS):
- Implantable neurostimulator activating genioglossus and tongue muscles during sleep
- Approved for moderate-severe OSA with BMI <32, CPAP failure
- Systematic review (Alrubasy et al., Resp Med 2024, PMID 39401661): significant AHI reduction; STAR trial results sustained at long-term follow-up
11. TORS (Transoral Robotic Surgery) FOR OSA
- Allows precise lingual tonsillectomy, tongue base resection, epiglottectomy
- Multiinstitutional study (2015): 293 procedures - mean AHI decrease of 24; success rate (AHI<20 + 50% reduction) demonstrated; complication rate 20.7% but no life-threatening events
- Best results when BMI <30
- (Cummings Otolaryngology, Ch. 28)
12. SPECIAL POPULATIONS
Pediatric OSA (Scott-Brown's Vol 2, Ch. 27):
- Prevalence ~1%; peak 3-6 years, equal sex ratio
- Cause: Adenotonsillar hypertrophy (most common)
- Features: Hyperactive behaviour, poor academic performance, neurobehavioural morbidity
- Treatment: Adenotonsillectomy is first-line - results in IGF-1 rise and growth spurt
- PSG scores improve significantly post-adenoidectomy
OSA in Women (Cummings):
- Under-diagnosed due to atypical presentation
- More likely to report insomnia, palpitations, ankle edema
- Prevalence increases post-menopause
13. COMORBIDITIES
From Goldman-Cecil Medicine (2024 ed.):
- Cardiovascular: Heart failure, systemic/pulmonary hypertension, AF, CAD, stroke
- Respiratory: COPD overlap syndrome, asthma
- Metabolic: Metabolic syndrome, Type 2 DM
- COVID-19: OSA independently increases risk of severe SARS-CoV-2 infection
- Surgical risk: Untreated severe OSA increases adverse cardiocerebrovascular events within 30 days of major non-cardiac surgery
14. PERIOPERATIVE MANAGEMENT
(Cummings, Box 15.6 + Miller's Anesthesia)
- Stepwise airway management algorithm
- Avoid paralytics until mask ventilation confirmed
- Oropharyngeal airway ready
- Consider awake fiberoptic intubation
- Counsel patient about possible tracheostomy
- Pre-op cardiovascular evaluation mandatory
15. RECENT ADVANCES (2024-2026)
1. Tirzepatide for OSA (SURMOUNT-OSA Trial - NEJM 2024)
- Phase 3, double-blind RCT (Malhotra A et al., NEJM 2024, PMID 38912654)
- Participants: Moderate-severe OSA + obesity (mean AHI ~51 events/hr, mean BMI ~39)
- Results:
- Trial 1 (PAP-naive): Mean AHI reduction -25.3 events/hr with tirzepatide vs -5.3 with placebo (difference -20.0, p<0.001)
- Trial 2 (PAP users): Mean AHI reduction -29.3 vs -5.5 (difference -23.8, p<0.001)
- Also reduced: Body weight, hypoxic burden, hsCRP, systolic BP, sleep impairment scores
- Significance: First GLP-1/GIP receptor agonist proven effective for OSA; FDA approved tirzepatide (Zepbound) for OSA in 2024
2. Bilateral HNS (2025 Clinical Trial, PMID 40702817)
- Bilateral hypoglossal nerve stimulation shown safe and effective in non-randomized clinical trial (Woodson et al., J Clin Sleep Med 2025)
3. Precision/Phenotype-Based Treatment
- Treatment tailored to individual OSA phenotype (anatomy, arousal threshold, loop gain, muscle responsiveness) - "precision medicine" approach described in Cummings (7th ed.)
- Pharmacological targeting of individual phenotypic traits under active investigation
4. Hypoglossal Nerve Stimulation Meta-Analysis (2024)
- Alrubasy et al., Respir Med 2024 (PMID 39401661) - Updated meta-analysis confirming AHI reduction and safety of HNS; Inspire device FDA approved
5. DISE-Guided Surgery
- Drug-induced sleep endoscopy now recommended to guide surgical planning; changes management in >50% of patients
6. Home Sleep Apnea Testing (HSAT)
- Validated for moderate-severe OSA diagnosis in uncomplicated patients; reduces cost and improves access to diagnosis
SUMMARY FLOWCHART: OSA - "COMPLETE PICTURE"
PREDISPOSING FACTORS
(Obesity, retrognathia, adenotonsillar hypertrophy,
male sex, age, alcohol)
│
▼
ANATOMIC NARROW PHARYNX + NEUROMUSCULAR FAILURE
│
▼
PHARYNGEAL COLLAPSE DURING SLEEP
│
▼
APNEA/HYPOPNEA (≥10 sec) → ↓SpO₂ → Arousal
│
┌────┴────┐
│ SLEEP │ ← Fragmented, non-restorative sleep
│ CYCLE │
│DISRUPTED│
└────┬────┘
│
┌────┴────────────────────┐
│ CLINICAL CONSEQUENCES │
│ EDS, cognitive deficit │
│ HTN, CV disease, DM │
└────┬────────────────────┘
│
┌────▼────────────────────────────────────┐
│ DIAGNOSIS │
│ Screening: ESS, STOP-BANG │
│ Confirmation: PSG (AHI) / HSAT │
│ Localization: DISE, Muller maneuver │
└────┬────────────────────────────────────┘
│
┌────▼────────────────────────────────────┐
│ TREATMENT │
│ 1st Line: CPAP (moderate-severe) │
│ Alternatives: OAT, Positional therapy │
│ Surgical: UPPP, MMA, TORS, HNS │
│ NEW: Tirzepatide (SURMOUNT-OSA, 2024) │
└─────────────────────────────────────────┘
REFERENCES (RGUHS-Relevant Textbooks)
| Textbook | Chapter/Reference |
|---|---|
| Cummings Otolaryngology Head & Neck Surgery, 7th ed. | Chapter 15: Sleep-Disordered Breathing; Ch. 28: TORS |
| Scott-Brown's Otorhinolaryngology H&N Surgery, 8th ed. | Vol 2 - Ch. 27: Paediatric OSA; Sleep-disordered breathing |
| Goldman-Cecil Medicine, 27th ed. | Chapter 374: Obstructive Sleep Apnea |
| Miller's Anesthesia, 10th ed. | Ch. 11: OSA perioperative management |
| Dhingra's Diseases of Ear, Nose & Throat | Ch: Snoring and Sleep apnea |
| Hazarika's ENT | OSA and Snoring chapter |
Recent Articles:
- Malhotra A et al. Tirzepatide for OSA and Obesity. NEJM 2024 (PMID 38912654) - SURMOUNT-OSA Phase 3 RCT
- Alrubasy WA et al. HNS for OSA - Updated Systematic Review. Resp Med 2024 (PMID 39401661)
- Woodson BT et al. Bilateral HNS for OSA. J Clin Sleep Med 2025 (PMID 40702817)
- Platon AL et al. An Update on OSAS - Literature Review. Medicina 2023 (PMID 37629749)
RGUHS Exam Tip: For 20 marks, write all sections above. For 10 marks, focus on: Definition, Classification (AHI), Pathophysiology (4 phenotypes), Diagnosis (ESS + STOP-BANG + PSG), Treatment (CPAP as first line + surgical options), and one Recent Advance (Tirzepatide/HNS). Diagrams of the STOP-BANG table, AHI classification box, and the Flowchart for Management are highly scoring.
This is a shared conversation. Sign in to Orris to start your own chat.