Awake craniotomy in details
Reading File
Finding Sources
Finding Sources
Searching PubMed
"awake craniotomy" technique outcomes
Awake craniotomy in details anaesthesia implications with more elaborate way
Reading File
Reading File
Reading File
Searching PubMed
"awake craniotomy" anesthesia technique
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
I now have comprehensive material from both Miller's and Barash to write a thorough, well-organized answer. Let me compose the full response.
Awake Craniotomy - Anesthesia Implications in Detail
1. Definition and Rationale
Awake craniotomy is a neurosurgical procedure performed under monitored anesthesia care (MAC) in which the patient remains conscious - either throughout or during a critical phase - allowing real-time neurological testing. It is indicated when a lesion (tumor, epileptic focus, vascular malformation) lies adjacent to or within eloquent cortex controlling:
- Motor function (primary motor cortex, corticospinal tract)
- Speech/language (Broca's area, Wernicke's area - usually left hemisphere)
- Sensory function (primary somatosensory cortex)
- Memory (mesial temporal structures)
The key advantage is that intraoperative cortical and subcortical mapping in a cooperative patient allows more aggressive tumor resection with simultaneous preservation of neurological function - something surrogate testing under general anesthesia cannot replicate for language. Recent meta-analysis (PMID: 41398134, 2025) confirms awake mapping improves extent of resection and neurological outcomes in low-grade gliomas.
2. Patient Selection and Preoperative Assessment
Patient cooperation is the single most important determinant of success. The anesthesiologist's preoperative role is as critical as the intraoperative one.
Ideal candidate:
- Psychologically motivated and non-claustrophobic
- Able to understand and follow instructions
- No severe anxiety disorder or cognitive impairment
- No uncontrolled movement disorder (tremor, dyskinesia)
- No morbid obesity or known difficult airway
- No language barriers that complicate testing
Preoperative workup includes:
- Thorough neuropsychological baseline assessment (speech, motor, sensory)
- Detailed explanation of each phase of the procedure: duration, what the patient will feel, what they will be asked to do, and what their limitations on movement will be
- Discussion of potential uncomfortable phases: pin fixation, craniotomy, dural manipulation (especially subtemporal dura - painful)
- If intraoperative electrocorticography (ECoG) is planned, anticonvulsants are often reduced by half or discontinued to avoid suppressing seizure activity needed for localization
- Benzodiazepine premedication is contraindicated if EEG localization of seizure foci is intended, as they suppress the abnormal EEG activity being sought
- Anxiolytics may still be used in non-EEG cases with caution
"A motivated patient is critical to the success of the procedure. Preoperative assessment should include a detailed explanation of the anesthetic so as to ensure cooperation and allay anxiety." - Barash Clinical Anesthesia 9e
3. Anesthetic Techniques
There are three recognized approaches, each with specific implications:
A. Monitored Anesthesia Care (MAC) Throughout
The patient is lightly sedated for the entire procedure. Sedation must be titrated carefully - deep enough for patient comfort during skull fixation and craniotomy, light enough for neurological testing throughout.
B. Asleep-Awake-Asleep (AAA) Technique (most commonly used)
- Phase 1 (Asleep): General anesthesia or deep sedation for positioning, head fixation, scalp infiltration, craniotomy, and dural opening. A supraglottic airway device (LMA/SLMA) is typically used. Some groups use an endotracheal tube with a custom design.
- Phase 2 (Awake): The airway device is removed once the brain surface is exposed. The patient is woken and cooperative testing (language, motor, sensory) is conducted.
- Phase 3 (Asleep): Airway device is reinserted and anesthesia re-induced for tumor resection and closure.
"Awake craniotomy can be performed with the patient sedated for the duration of the procedure, or with an 'asleep-awake-asleep' technique employing a supraglottic airway device." - Barash 9e
C. Conscious Sedation Throughout
Light sedation during all phases; the patient is never fully anesthetized. This requires near-perfect local anesthesia.
4. The Local Anesthetic Technique - The Foundation
"The essential element of an anesthetic for an awake craniotomy is the local anesthetic technique. Sedation cannot compensate for inadequate anesthesia of the scalp." - Miller's Anesthesia 10e
Scalp Nerve Block
Six nerves innervate the scalp and relevant structures and must be blocked:
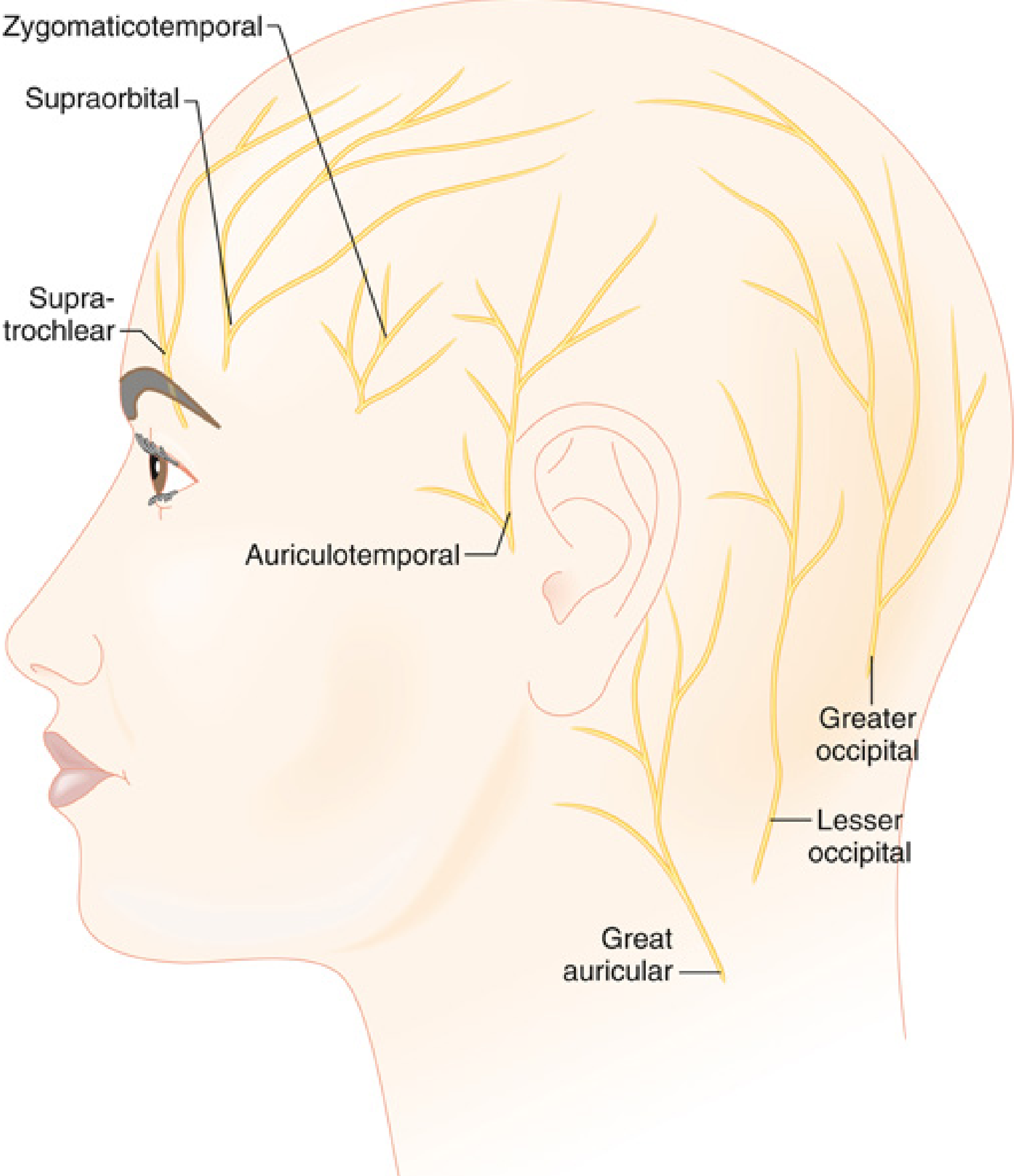
| Nerve | Territory |
|---|---|
| Supratrochlear | Medial forehead |
| Supraorbital | Lateral forehead, anterior scalp |
| Zygomaticotemporal | Temple |
| Auriculotemporal | Temporal region, pre-auricular |
| Lesser occipital | Posterior scalp, lateral |
| Greater occipital | Posterior scalp, medial |
The block may be performed unilaterally or bilaterally. Additionally, pin sites must be infiltrated with local anesthetic - this is one of the most painful stimuli during the procedure.
Agents used:
- Short procedures: 1% mepivacaine
- Prolonged procedures: 0.75% ropivacaine
- Epinephrine-containing solutions are preferred for vasoconstriction and prolongation of block
Key hazard: Local anesthetic toxicity (LAST). The volumes used for scalp blocks plus surgical infiltration of the dura and incision lines are substantial. The anesthesiologist must actively track cumulative doses as the surgeon continues to infiltrate throughout the procedure.
"The volume of local anesthetic used to infiltrate pin sites and perform the scalp nerve blocks can be substantial. It is appropriate for the anesthesiologist to keep track of, and provide advice about, the doses of local anesthetics used." - Miller's Anesthesia 10e
5. Sedation Agents - Detailed Pharmacology
Propofol
- Most widely used; provides titratable, predictable sedation
- Rapid awakening facilitates quick transition to the awake phase
- Must be discontinued at least 15 minutes before EEG recording - leaves a residual high-frequency, high-amplitude beta activity footprint on the EEG that obscures abnormal seizure activity
- When seizures occur during cortical stimulation, small boluses of propofol (0.5-1.0 mg/kg IV, or 20 mg bolus) are used to terminate them - but should be withheld briefly to allow spontaneous termination since propofol interferes with subsequent EEG localization
Remifentanil
- Ultra-short-acting opioid; complements propofol for painful phases
- Infusion rate: 0.02-0.05 mcg/kg/min
- Synergistic respiratory depression with propofol - the most significant danger in a patient with a fixed, inaccessible airway (head in pin fixation)
Dexmedetomidine
- Highly selective alpha-2 adrenergic agonist
- Provides sedation + anxiolysis + analgesia with minimal respiratory depression - its key advantage
- Increasingly the preferred agent, especially as a sole or primary drug
- Effective infusion range during testing: 0.1-0.5 mcg/kg/h
- Does not suppress spontaneous seizure activity at lower doses - suitable when ECoG is planned
- Allows satisfactory conditions for brain stimulation speech mapping and ECoG
- Limitation: may cause delays in achieving adequate patient responsiveness (slower onset/offset than propofol)
- Meta-analysis (PMID: 39079421, 2024) confirms dexmedetomidine provides equivalent sedation and mapping conditions with significantly lower rates of respiratory depression compared to propofol-remifentanil
"Dexmedetomidine is the agent of choice for sedation of patients undergoing awake craniotomies." - Morgan & Mikhail Clinical Anesthesiology 7e
Agent Combinations
- Propofol + remifentanil: effective but higher respiratory depression risk
- Propofol + dexmedetomidine: useful combination balancing depth with respiratory safety
- Dexmedetomidine + remifentanil: increasingly used
- Benzodiazepines: generally avoided - highest potential to interfere with EEG recording and seizure focus localization; also long duration
Monitoring Sedation Depth
- Standard ASA monitors
- Capnography is essential - provides breath-by-breath confirmation of airway patency and respiratory drive if deep sedation is used at any phase
- BIS monitoring may help titrate sedation
- An arterial catheter is routinely placed for beat-to-beat hemodynamic monitoring and blood gas sampling
6. Airway Management
The airway is the most unforgiving aspect of awake craniotomy anesthesia, given that:
- The patient's head is turned and fixed in a rigid pin head-holder
- The surgical drape obscures most of the patient's body
- Emergency intubation in this position is extremely difficult
Key principles:
- Positioning optimization is critical before sedation begins: maximize neck flexion and atlanto-occipital extension so the anesthesiologist retains the widest latitude to sedate while maintaining spontaneous ventilation
- The surgical drape must be positioned to allow direct, constant visual access to the patient's face - for airway monitoring AND to present naming/speech test images
- Hypoventilation and hypercapnia are detrimental - CO2 retention causes cerebral vasodilation and brain swelling, worsening surgical exposure
- Apnea requiring emergency intubation in a patient in a rigid head holder is a potentially catastrophic complication
LMA use: Various groups have reported use of the LMA during the asleep phases with spontaneous or controlled ventilation, removed once the brain surface is exposed. Importantly, LMA techniques are most commonly used when the head is not in pin fixation. When pin fixation is used, the LMA must be removed and replaced carefully, and plans for emergency airway management need to be thought through before the case starts.
7. Cortical and Subcortical Mapping - Anesthesia Interface
How mapping works:
The neurosurgeon uses a bipolar or monopolar probe stimulator to electrically stimulate cortical and subcortical areas while a neuropsychologist conducts real-time tests:
- Object naming / picture naming - for language cortex identification
- Counting or reading - speech arrest indicates language involvement
- Limb movement testing - for motor strip mapping
- Sensory responses - for sensory cortex mapping
ECoG (Electrocorticography) for seizure surgery:
- After dural opening, cortical surface EEG is recorded to locate the seizure focus
- If no spontaneous seizure activity is seen, provocative agents may be given:
- Methohexital ~0.3 mg/kg - generally safe and effective
- Etomidate 0.05-0.1 mg/kg - alternative
- Alfentanil 30-50 mcg/kg bolus - used under general anesthesia
- Remifentanil 2.5 mcg/kg bolus - reported effective
- Hyperventilation - also activates seizure foci
Anesthesia implications during mapping:
- No propofol during EEG recording (residual beta footprint)
- Dexmedetomidine can continue at low rates during testing
- Ensure patient is fully responsive, communicating, and understands instructions
- Constant communication between anesthesiologist, surgeon, and neuropsychologist
8. Intraoperative Complications and Management
| Complication | Cause | Management |
|---|---|---|
| Intraoperative seizure | Cortical stimulation, tumor, or spontaneous | Cold saline irrigation of cortex by surgeon (first line); propofol 0.5-1.0 mg/kg IV (hold briefly to allow spontaneous termination); have phenytoin/levetiracetam ready |
| Respiratory depression / apnea | Oversedation, opioid effect, propofol-remifentanil synergy | Reduce/stop infusions; airway repositioning; jaw thrust; emergency LMA/intubation (very difficult in pin fixation - plan ahead) |
| Airway obstruction | Sedation-induced, positional | Airway repositioning maneuvers; consider nasal airway prior to draping |
| Patient non-cooperation / disinhibition | Anxiety, confusion, paradoxical reaction | Reassurance; small propofol bolus; abort awake phase if needed |
| Oversedation | Excessive drug titration | Hold all infusions; stimulation to arouse; airway rescue |
| Intractable brain swelling | Hypercapnia, venous obstruction, tumor edema | Hyperventilate; mannitol/hypertonic saline; dexamethasone; abort awake phase |
| Pain / discomfort | Inadequate local anesthesia, dural traction | Surgeon supplemental LA infiltration; small opioid bolus; adjust position |
| Nausea and vomiting | Opioids, brain manipulation | Anti-emetics (ondansetron, dexamethasone preop); limit opioids |
| LAST (Local anesthetic systemic toxicity) | Excessive LA volume | Track cumulative doses; have Intralipid 20% immediately available; ACLS |
"Seizures should be treated with cold saline applied to the brain surface by the surgeon and a small bolus of propofol (20 mg) intravenously." - Barash 9e
9. Patient Positioning Considerations
- All padding and positioning must be completed before any sedation is given - the patient cannot reposition themselves once the head is fixed and sedation has started
- Common positions: lateral decubitus or supine with head turned
- Pressure areas, eye protection, arm padding
- Urinary catheter placement (procedures are typically 3-6 hours)
- Temperature management (warm blankets, forced air warming to prevent hypothermia and shivering during the awake phase)
- The anesthesiologist must be able to see the patient's face at all times from their position at the head of the bed
10. Monitoring
| Monitor | Purpose |
|---|---|
| Arterial line | Beat-to-beat BP, blood gas sampling |
| SpO2 | Continuous oxygenation |
| Capnography (ETCO2) | Essential - airway patency and ventilation confirmation |
| EEG / ECoG | Seizure localization (by neurophysiology team) |
| Standard ECG, NIBP | Routine |
| Temperature | Prevent hypothermia |
| Neuropsychological testing | Real-time cortical mapping |
| BIS (optional) | Sedation depth titration |
11. Postoperative Considerations
- Patients may be observed in PACU or ICU (similar to any craniotomy)
- Most patients tolerate sedation for surgical closure after the awake phase
- Analgesia: multimodal approach - scalp block provides good postoperative pain relief, supplemented with paracetamol/NSAIDs, opioids as needed
- Monitor for new neurological deficit (compare to intraoperative baseline)
- Seizure precautions continue postoperatively
- For patients who tolerated the procedure poorly or are poor awake candidates, surrogate testing under general anesthesia is an alternative for motor/sensory mapping - but language testing cannot be performed under GA
12. Special Considerations
Epilepsy Surgery vs. Tumor Surgery
- Epilepsy cases require discontinuation of anticonvulsants and avoidance of propofol before EEG recording
- Tumor cases primarily need language and motor mapping; ECoG is less central
Pregnant Patients
- Case reports exist; dexmedetomidine and mannitol have been used (PMID: referenced in Miller's - Handlogten et al., 2015)
Pediatric Patients
- Awake craniotomy in children is rare but feasible from age ~10-12 years; requires highly experienced teams and careful psychological preparation
- Meta-analysis (PMID: 37839565, 2024) shows comparable outcomes to adults in selected pediatric patients
Failed Awake Craniotomy
- If the patient becomes uncooperative or experiences an emergency, conversion to general anesthesia in the middle of the procedure with a head in a pin holder is technically very challenging and must be planned for
Summary: The Anesthesiologist's Core Priorities
- Patient selection and preparation - Ensure a motivated, well-informed, cooperative patient
- Perfect local anesthesia - Scalp nerve blocks are the cornerstone; sedation cannot substitute
- Meticulous sedation titration - Match depth to the phase of the procedure
- Airway vigilance - Capnography, constant visual access, pre-planned emergency rescue
- Avoid LA toxicity - Track cumulative doses
- Drug selection for ECoG - No benzodiazepines; stop propofol 15 min before EEG; dexmedetomidine preferred
- Seizure preparedness - Cold saline first, propofol rescue second
- Communication - Constant verbal contact with the patient throughout
Sources:
- Miller's Anesthesia, 2-Volume Set, 10e, Chapter 53 (Neurosurgical Anesthesia) - Awake Craniotomy and Seizure Surgery
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, Chapter on Neuroanesthesia - Awake Craniotomy
- Morgan & Mikhail's Clinical Anesthesiology, 7e
- Akavipat et al. (2024) - Dexmedetomidine for awake craniotomy: Systematic review and meta-analysis [PMID: 39079421]
- Sadhasivam et al. (2025) - Awake mapping and extent of resection in low-grade gliomas [PMID: 41398134]
- Honeyman et al. (2025) - Awake vs asleep craniotomy for eloquent glioblastoma [PMID: 40887547]
Create a quick reference PDF for awake craniotomy anesthesia team checklist
Reading File
Running Command
Writing File
Running Command
Running Command
The PDF is ready. Here's your download link:
Awake Craniotomy Checklist
PDF Document · PDF
Here's what's included in the checklist:
Structure (A4, color-coded by section):
| Section | Color |
|---|---|
| Pre-operative Assessment | Dark navy |
| Equipment & Drug Preparation | Charcoal |
| Scalp Nerve Block (6 nerves table) | Teal |
| Sedation Agent Quick-Reference | Purple |
| Phase 1 — Asleep (Induction → Dural opening) | Navy |
| Phase 2 — Awake (Brain mapping) | Teal |
| Phase 3 — Re-sleep (Resection & Closure) | Dark slate |
| Complication Response Table | Red |
| Post-op Handover Points | Green |
| Key Reminders Box | Amber |
Design features:
- ☐ Checkboxes for every actionable item
- ⚠ Red warning markers on high-risk items (e.g., NO benzos before EEG, propofol stop 15 min before recording, LAST risk, emergency airway limitation)
- Dual-column layout throughout to maximize content density
- Scalp nerve block table with landmarks and territories
- Sedation drug table with loading doses, infusion rates, and key cautions
- Complication response table with first-line and escalation steps
- Footer citing Miller's 10e, Barash 9e, Morgan & Mikhail 7e
This is a shared conversation. Sign in to Orris to start your own chat.