Being my teacher who have 20 year experience explain the topics which I provide to you make it easier and providing some clinical scenarios and provide me FMGE type questions at last for practice
I'm ready to be your teacher! With my 20 years of experience, I'll break down any topic in a clear, clinically relevant way - with real-world scenarios and FMGE-style MCQs at the end.
Please go ahead and share the topic(s) you want to learn today!
For example, you can give me:
- A single topic (e.g., "Rheumatic fever")
- A system (e.g., "Renal physiology")
- A disease group (e.g., "Bleeding disorders")
- A drug class (e.g., "Beta blockers")
What would you like to study? 📚
Primary hyperthyroidism and subclincal hyperthyroidism
Reading File
Finding Sources
Finding Sources
Searching PubMed
hyperthyroidism diagnosis treatment guidelines
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything I need from the textbooks to deliver a thorough, teacher-style lesson. Let me compose the complete answer.
🎓 Primary Hyperthyroidism & Subclinical Hyperthyroidism
Your 20-Year Experienced Teacher's Complete Guide
PART 1: UNDERSTANDING THE BASICS FIRST
Think of the thyroid as a furnace and TSH as the thermostat. Normally, when the furnace overheats (too much T4/T3), the thermostat turns off (TSH drops). In hyperthyroidism, the furnace is running too hot - and we classify severity by how much the thermostat has responded.
| Parameter | Overt (Primary) Hyperthyroidism | Subclinical Hyperthyroidism |
|---|---|---|
| TSH | Suppressed (<0.1 mIU/L) | Low/subnormal |
| Free T4 | HIGH | NORMAL |
| Free T3 | HIGH | NORMAL |
| Symptoms | Present (hypermetabolic) | Absent or minimal |
Memory trick: "Sub" = below the surface. Subclinical = labs are only partially abnormal, patient looks okay on the surface.
PART 2: PRIMARY HYPERTHYROIDISM - THE FULL PICTURE
2.1 Causes (Must Know for FMGE)
| Cause | Key Feature |
|---|---|
| Graves disease | Most common in iodine-replete areas; autoimmune (TSH-RS antibodies); goiter + ophthalmopathy |
| Toxic Multinodular Goiter (TMNG / Plummer disease) | Most common in iodine-deficient areas (up to 60% of thyrotoxicosis) |
| Toxic Adenoma | Single autonomously functioning nodule; hot on radio-isotope scan |
| TSH-secreting pituitary adenoma | Rare; TSH is elevated/normal with high T4 - central hyperthyroidism |
| Factitious / Iatrogenic | Exogenous T4; low RAIU; FT4:FT3 ratio altered |
| Acute thyroiditis | Transient; pain + fever |
(Source: Textbook of Family Medicine 9e, p. 1019)
2.2 Graves Disease - In Depth (Most FMGE Questions Come From Here)
Mechanism: TSH-receptor stimulating antibodies (TSH-RS Abs / TRAb) attach to TSH receptors on thyroid cells and mimic TSH, causing uncontrolled T4/T3 synthesis. The pituitary sees excess T4 and shuts off TSH - often to <0.01 mIU/L (essentially undetectable).
Classic Triad:
- Diffuse goiter (present in >90% of cases)
- Ophthalmopathy (proptosis, lid lag - due to orbital fibroblast inflammation)
- Pretibial myxedema (non-pitting, waxy skin over shins)
Exam pearl: If a patient has hyperthyroidism WITHOUT goiter and WITHOUT eye signs, question the diagnosis of Graves disease!
Signs & Symptoms (hypermetabolic state):
- Tachycardia, wide pulse pressure, systolic hypertension
- Warm, moist skin; heat intolerance; excessive sweating
- Weight loss despite good appetite
- Tremor, anxiety, hyperactivity, insomnia
- Diarrhea
- In women: oligomenorrhea
- In elderly: "apathetic thyrotoxicosis" - atrial fibrillation is the main feature, NOT classic symptoms
2.3 Diagnosis Workup
Step 1 - Biochemistry:
- TSH (most sensitive; suppressed <0.1 mIU/L)
- Free T4 and Free T3 (elevated in overt disease)
- TSH-RS Abs (positive in Graves disease)
Step 2 - Imaging:
- Radioiodine Uptake (RAIU) scan with I-123:
- Diffuse increased uptake = Graves disease
- Focal hot nodule = Toxic adenoma
- Multiple hot areas = TMNG
- Low/no uptake = thyroiditis or factitious hyperthyroidism
PART 3: CLINICAL SCENARIOS
🏥 Scenario 1 - Classic Graves Disease
A 28-year-old woman comes to your clinic with a 3-month history of weight loss (5 kg), palpitations, excessive sweating, and difficulty sleeping. On examination: pulse 112/min, diffuse smooth goiter, and you notice her eyes look prominent. Labs: TSH = 0.005 mIU/L (undetectable), FT4 = 3.8 ng/dL (high), TSH-RS Abs = strongly positive.
What is happening? This is textbook Graves disease. The TRAb is hijacking the TSH receptor, running the thyroid on overdrive. Her pituitary has completely shut off TSH.
Management:
- Step 1: Propranolol (beta-blocker) immediately for symptom control (palpitations, tremor, anxiety) - this is a temporizing measure only
- Step 2: Methimazole (MMI) as first-line antithyroid drug - blocks thyroid peroxidase, inhibiting T4/T3 synthesis
- Step 3: Long-term plan: ATDs for 12-18 months OR Radioactive Iodine (RAI) I-131 OR surgery
Why MMI over PTU? PTU has serious hepatotoxicity risk. MMI is preferred in all patients EXCEPT first-trimester pregnancy (PTU preferred in T1 because MMI causes embryopathy).
🏥 Scenario 2 - Apathetic Thyrotoxicosis (The Trap!)
A 72-year-old man is referred for new-onset atrial fibrillation. He denies any weight change or anxiety. Examination: no goiter, no eye signs. TSH = 0.004 mIU/L, FT4 = 2.9 ng/dL (high).
The trap: Classic symptoms (anxiety, tremor, sweating) are ABSENT in the elderly. They instead present with:
- Atrial fibrillation (most common presentation)
- Heart failure
- Unexplained weight loss
- Depression or apathy (NOT hyperactivity)
FMGE pearl: Elderly + new-onset AF + suppressed TSH = think apathetic thyrotoxicosis until proven otherwise!
🏥 Scenario 3 - Toxic Multinodular Goiter
A 55-year-old woman from a mountain village presents with a large multinodular goiter for years. She now has palpitations. TSH = 0.03 mIU/L, FT4 high. TRAb NEGATIVE. RAIU scan shows multiple hot nodules.
Diagnosis: TMNG (Plummer disease). No autoimmune antibodies. Preferred treatment = RAI or surgery (not long-term ATDs, as these don't cure autonomous nodules).
PART 4: SUBCLINICAL HYPERTHYROIDISM - DETAILED
4.1 Definition & Classification
Definition: Subnormal TSH with normal FT4 and FT3, in an asymptomatic patient. (Tietz Textbook of Laboratory Medicine, 7th Ed)
Two grades - this distinction is HIGH-YIELD:
| Grade | TSH Level | Clinical Significance |
|---|---|---|
| Grade 1 | 0.1 - 0.4 mIU/L (low detectable) | Milder; may spontaneously normalize |
| Grade 2 | <0.1 mIU/L (undetectable) | Higher risk of progression to overt disease and cardiac complications |
25% of subclinical hyperthyroidism patients have Grade 2 disease. Grade 2 carries significantly more cardiovascular risk.
(Source: Braunwald's Heart Disease, p. 1147)
4.2 Causes
Endogenous (primary):
- Graves disease (early/mild)
- TMNG
- Solitary autonomous nodule
- In iodine-deficient areas: nodular disease more likely to persist/progress
Exogenous (most common cause overall):
- Overtreatment with levothyroxine - most common cause overall, reversible by dose reduction
- Intentional TSH suppression in thyroid cancer patients (only indicated in HIGH-RISK thyroid cancer)
Transient:
- Post-RAI or antithyroid drug treatment
- Thyroiditis phase
Key exam point: In Graves disease, subclinical hyperthyroidism tends to revert to normal. In TMNG/autonomous nodule, it tends to persist or progress.
4.3 Why Does It Matter? - Complications
Even with normal hormone levels, the suppressed TSH itself signals the body that thyroid hormone action is excessive. Long-term consequences:
| System | Complication |
|---|---|
| Heart | Atrial fibrillation (2-3x higher incidence vs normal TSH!) |
| Heart | Heart failure, increased LV mass, diastolic dysfunction |
| Bone | Osteoporosis and fractures (especially postmenopausal women) |
| Vascular | Carotid artery plaques, increased stroke risk |
| Cardiac rhythm | Increased ectopic beats |
(Source: Tietz Textbook of Laboratory Medicine 7th Ed, Family Medicine 9e)
Framingham study showed: Individuals with subclinical hyperthyroidism are at increased risk for paroxysmal atrial fibrillation. This is the landmark data you must know for FMGE.
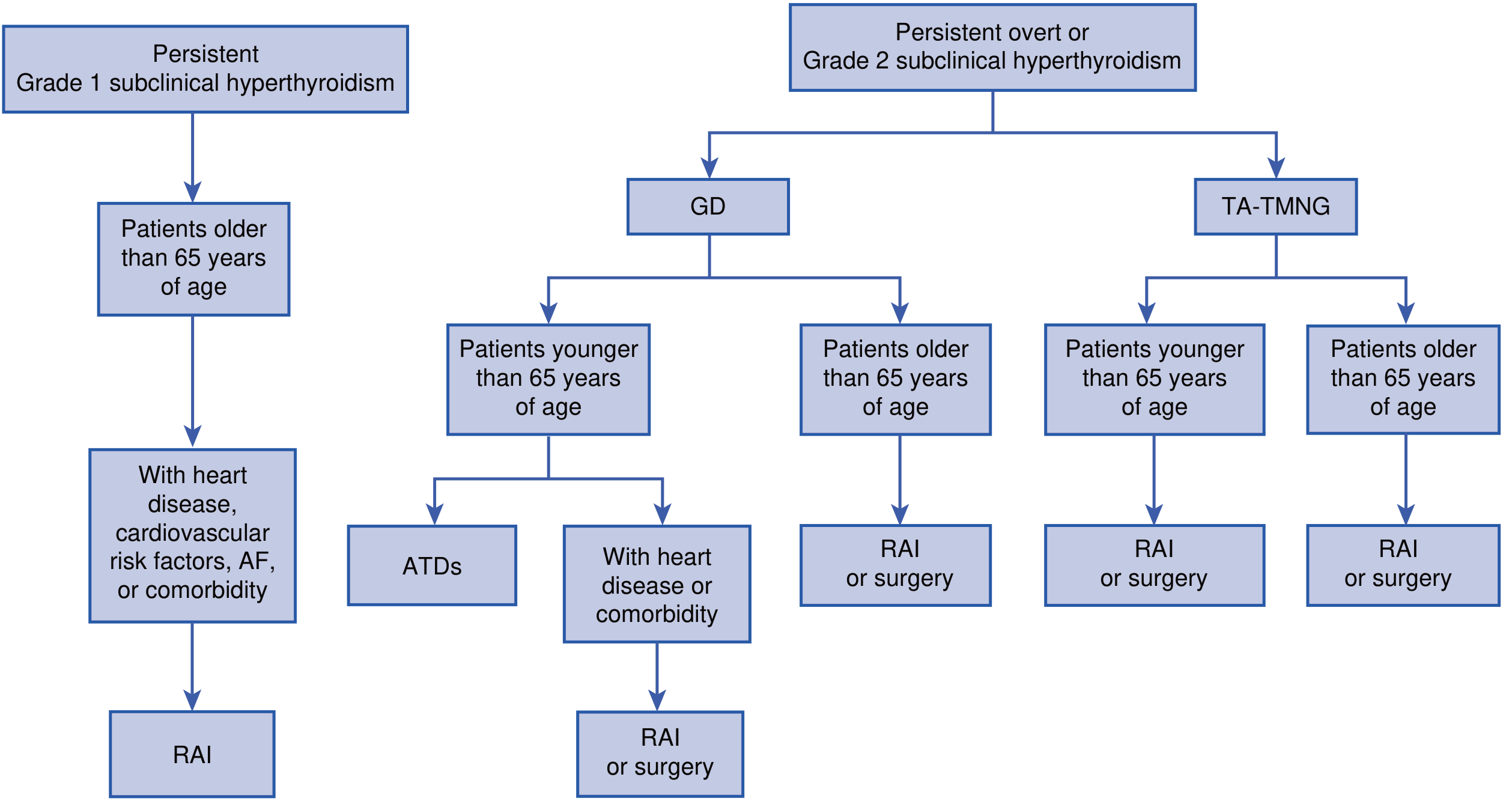
4.4 Treatment of Subclinical Hyperthyroidism
The controversy: Treat or watch? This depends on Grade + patient risk.
ATA/AACE Guidelines say - TREAT when TSH persistently <0.1 mIU/L (Grade 2) AND any of:
- Age > 65 years
- Postmenopausal women NOT on estrogens or bisphosphonates
- Osteoporosis
- Cardiac risk factors or established AF
- Symptomatic patients
Do NOT treat in:
- Asymptomatic young patients with Grade 1 (TSH 0.1-0.4 mIU/L)
- Premenopausal women with Grade 1
- No evidence of harm found
Treatment modality by cause:
- TMNG/autonomous nodule: RAI is preferred (definitive)
- Graves disease (young): ATDs (may spontaneously remit)
- Graves disease (elderly with comorbidities): RAI or surgery
- Exogenous (levothyroxine overtreatment): Reduce LT4 dose
Treatment Flowchart (from Braunwald's Heart Disease):
PART 5: THYROID STORM (Bonus - High Yield!)
Thyroid storm is the most severe, life-threatening form of hyperthyroidism.
Features:
- Fever (cardinal sign)
- Altered mental status
- Severe tachycardia / new AF
- GI symptoms (nausea, vomiting, diarrhea, rarely jaundice)
- Cardiovascular collapse
Mortality can reach 50%
Treatment (the sequence matters for FMGE):
- Beta-blocker (propranolol IV) - control HR
- PTU (preferred over MMI in storm - also blocks T4→T3 conversion in periphery)
- Iodine (Lugol's solution / SSKI) - given 1 hour AFTER PTU (to block hormone release; if given first, iodine is used as substrate)
- Glucocorticoids (dexamethasone) - reduce T4→T3 conversion, treat relative adrenal insufficiency
- Treat the precipitant (infection, surgery, trauma)
Sequence memory: "B-P-I-G" - Beta-blocker, PTU, Iodine (after PTU!), Glucocorticoids
PART 6: QUICK COMPARISON TABLE
| Feature | Primary Hyperthyroidism | Subclinical Hyperthyroidism |
|---|---|---|
| TSH | Suppressed <0.1 mIU/L | Low (Grade1: 0.1-0.4; Grade2: <0.1) |
| Free T4/T3 | Elevated | Normal |
| Symptoms | Present | Absent/minimal |
| Most common cause | Graves disease | Exogenous LT4 overtreatment |
| AF risk | High | 2-3x increased vs normal |
| Treatment | Always needed | Risk-based (age, grade, comorbidities) |
PART 7: PTU vs METHIMAZOLE - FMGE Comparison
| Feature | PTU | Methimazole |
|---|---|---|
| Mechanism | Blocks TPO + peripheral T4→T3 conversion | Blocks TPO only |
| Preferred in | Thyroid storm, First trimester pregnancy | All other situations |
| Side effect | Hepatotoxicity (serious, rare) | Agranulocytosis (most dangerous) |
| Monitoring | LFTs | CBC (if fever/sore throat - stop immediately!) |
🎯 FMGE-STYLE PRACTICE MCQs
Q1. A 25-year-old woman presents with weight loss, palpitations, and proptosis. TSH is 0.004 mIU/L, FT4 is elevated. TSH-receptor antibodies are strongly positive. What is the most likely diagnosis?
- A) Toxic multinodular goiter
- B) Graves disease
- C) Hashimoto's thyroiditis
- D) Toxic adenoma
Answer: B - Graves disease. TRAb positivity + proptosis + diffuse hyperfunction = classic Graves.
Q2. A 60-year-old man is found to have TSH = 0.08 mIU/L and normal FT4 on routine labs. He is asymptomatic. This is best classified as:
- A) Overt hyperthyroidism
- B) Grade 1 subclinical hyperthyroidism
- C) Grade 2 subclinical hyperthyroidism
- D) Normal thyroid function
Answer: C - Grade 2 subclinical hyperthyroidism. TSH <0.1 mIU/L with normal FT4 = subclinical; and <0.1 = Grade 2.
Q3. In subclinical hyperthyroidism, which of the following is the MOST common cardiovascular complication?
- A) Ventricular tachycardia
- B) Atrial fibrillation
- C) Complete heart block
- D) Pulmonary hypertension
Answer: B - Atrial fibrillation. Risk is 2-3x higher. Framingham data confirms this.
Q4. Which antithyroid drug is preferred in the FIRST TRIMESTER of pregnancy?
- A) Methimazole
- B) Carbimazole
- C) Propylthiouracil (PTU)
- D) Propranolol
Answer: C - PTU. Methimazole causes aplasia cutis and choanal atresia (embryopathy) in T1. PTU is safe in first trimester; switch to MMI in T2/T3.
Q5. In thyroid storm, iodine (Lugol's solution) is given:
- A) Before PTU
- B) Simultaneously with PTU
- C) At least 1 hour AFTER PTU
- D) Instead of PTU
Answer: C - At least 1 hour after PTU. If iodine is given first, the thyroid uses it as substrate to synthesize MORE hormone. PTU must block synthesis first, then iodine blocks release.
Q6. A 70-year-old man with persistent Grade 2 subclinical hyperthyroidism (TSH = 0.05 mIU/L) and newly diagnosed atrial fibrillation. He has TMNG on ultrasound. What is the preferred treatment?
- A) Methimazole long-term
- B) Radioactive Iodine (RAI)
- C) Observation only
- D) Propranolol alone
Answer: B - RAI. Elderly + Grade 2 SCH + AF + TMNG = treat. RAI is preferred for TMNG in elderly. ATDs do not cure autonomous nodules.
Q7. The MOST common cause of subclinical hyperthyroidism overall is:
- A) Graves disease
- B) Toxic adenoma
- C) Exogenous levothyroxine overtreatment
- D) TMNG
Answer: C - Exogenous levothyroxine overtreatment. Most common cause, and the only one that is simply reversed by reducing the LT4 dose.
Q8. An elderly patient presents with new-onset heart failure and atrial fibrillation. She has no goiter, no proptosis, and no classic hyperthyroid symptoms. TSH is 0.003 mIU/L, FT4 elevated. This presentation is called:
- A) Hashitoxicosis
- B) Apathetic thyrotoxicosis
- C) Subclinical hyperthyroidism
- D) Secondary hyperthyroidism
Answer: B - Apathetic thyrotoxicosis. Classic presentation in the elderly - AF/HF without adrenergic symptoms. A common clinical trap in exams.
Q9. Which of the following features differentiates Graves disease from toxic adenoma on radionuclide scan?
- A) Diffuse homogeneous uptake vs focal hot nodule
- B) Cold nodule vs hot nodule
- C) Low uptake vs no uptake
- D) No difference - both show the same pattern
Answer: A. Graves = diffuse uniform increased uptake. Toxic adenoma = single focal hot nodule with suppression of surrounding tissue.
Q10. A 32-year-old pregnant woman (8 weeks gestation) is diagnosed with Graves disease. She requires antithyroid therapy. The most appropriate choice is:
- A) Methimazole
- B) Radioactive iodine I-131
- C) Propylthiouracil
- D) Total thyroidectomy
Answer: C - PTU. RAI is absolutely contraindicated in pregnancy (crosses placenta, destroys fetal thyroid). MMI is teratogenic in T1. PTU is the drug of choice in first trimester.
📌 SUMMARY TAKE-HOME POINTS
- TSH is the most sensitive single test for detecting both primary and subclinical hyperthyroidism
- Graves disease = TRAb positive + diffuse goiter + eye signs - most common cause of overt hyperthyroidism in iodine-replete areas
- TMNG = most common in iodine-deficient areas; no antibodies; treated with RAI (not cured by ATDs)
- Subclinical hyperthyroidism = normal FT4/T3 but suppressed TSH; Grade 2 (<0.1) is more dangerous than Grade 1 (0.1-0.4)
- AF and osteoporosis are the two major complications of subclinical hyperthyroidism to remember
- Treat subclinical only if: >65 years, postmenopausal, osteoporosis, cardiac risk, or Grade 2
- PTU in T1 pregnancy and thyroid storm; MMI everywhere else
- Thyroid storm sequence: B-P-I-G (Beta-blocker → PTU → Iodine 1hr later → Glucocorticoids)
Sources: Textbook of Family Medicine 9e | Braunwald's Heart Disease 2-Vol Set | Tietz Textbook of Laboratory Medicine 7th Ed | Sabiston Textbook of Surgery
Recent evidence (PMID 38758966): A 2024 systematic review in the European Thyroid Journal confirms there remains a "remarkable range of recommendations" for subclinical hyperthyroidism treatment across guidelines - so individualized risk-based decisions remain the standard.
This is a shared conversation. Sign in to Orris to start your own chat.