Renal osteo dystrophy etiology pathology and signs and symptoms investigation and treatment explain in detail with appropriate illustrative images and diagrams
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the content I need to write a thorough, well-illustrated response. Let me compose the complete answer.
Renal Osteodystrophy: A Comprehensive Overview
Definition
Renal osteodystrophy (ROD) describes the collective skeletal changes that occur in chronic kidney disease (CKD), encompassing all bone disorders arising from disturbances of mineral metabolism, altered hormonal signaling, and uremic toxicity. Per KDIGO (2006), the term should be used exclusively to define alterations in bone morphology associated with CKD. The broader systemic syndrome - including all clinical, biochemical, and imaging abnormalities - is now termed CKD-Mineral and Bone Disorder (CKD-MBD).
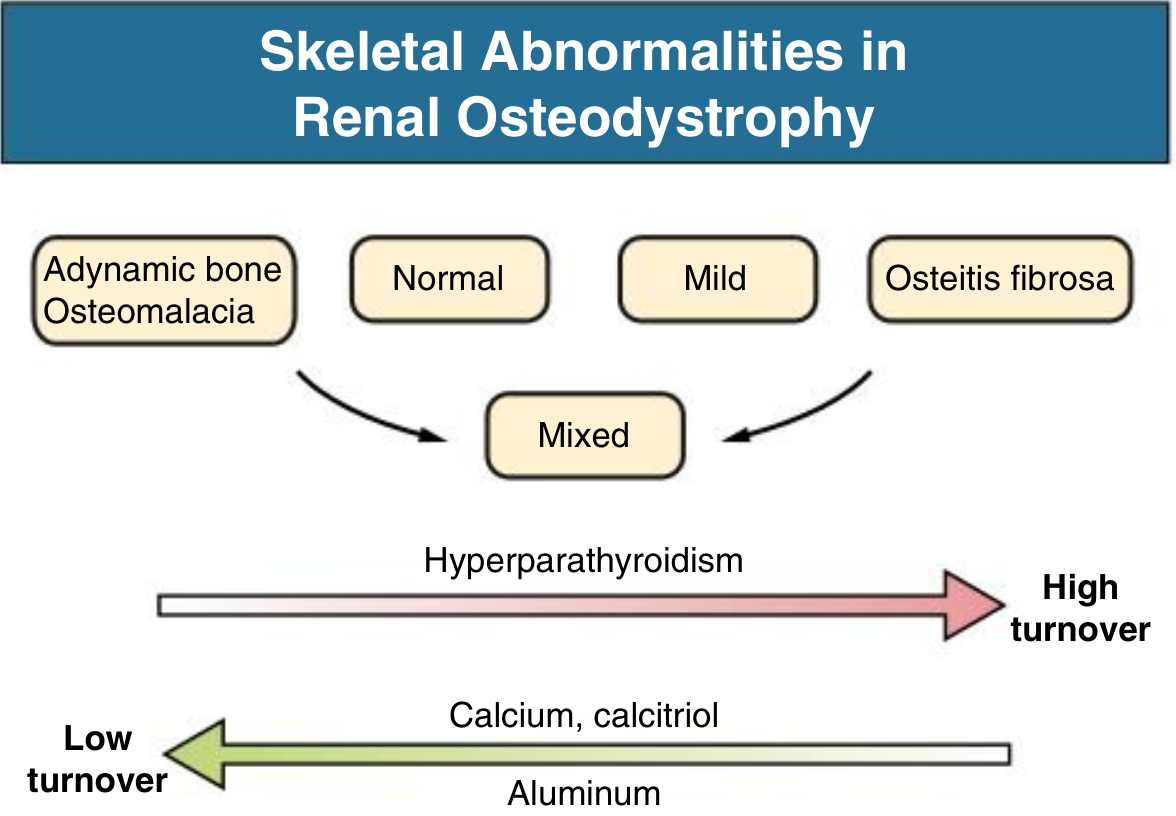
The spectrum of skeletal abnormalities includes:
- Osteitis fibrosa - high-turnover disease from hyperparathyroidism
- Osteomalacia - defective mineralization, often aluminum-related
- Adynamic bone disease (ABD) - abnormally low bone turnover
- Mixed renal osteodystrophy - combinations of the above
- Osteopenia/Osteoporosis
Comprehensive Clinical Nephrology, 7th Ed., p. 1179
The Spectrum of Skeletal Abnormalities
KDIGO TMV Classification
The KDIGO-recommended Turnover, Mineralization, Volume (TMV) classification provides a clinically relevant histomorphometric description:
| Parameter | Options |
|---|---|
| Turnover | Low / Normal / High |
| Mineralization | Normal / Abnormal |
| Volume | Low / Normal / High |
Any combination is possible in a given biopsy specimen. This replaced the older simple high/low turnover binary scheme.
Brenner and Rector's The Kidney, p. 2411
Etiology and Pathogenesis
The pathogenesis is multi-factorial. Several interconnected mechanisms converge as CKD progresses.
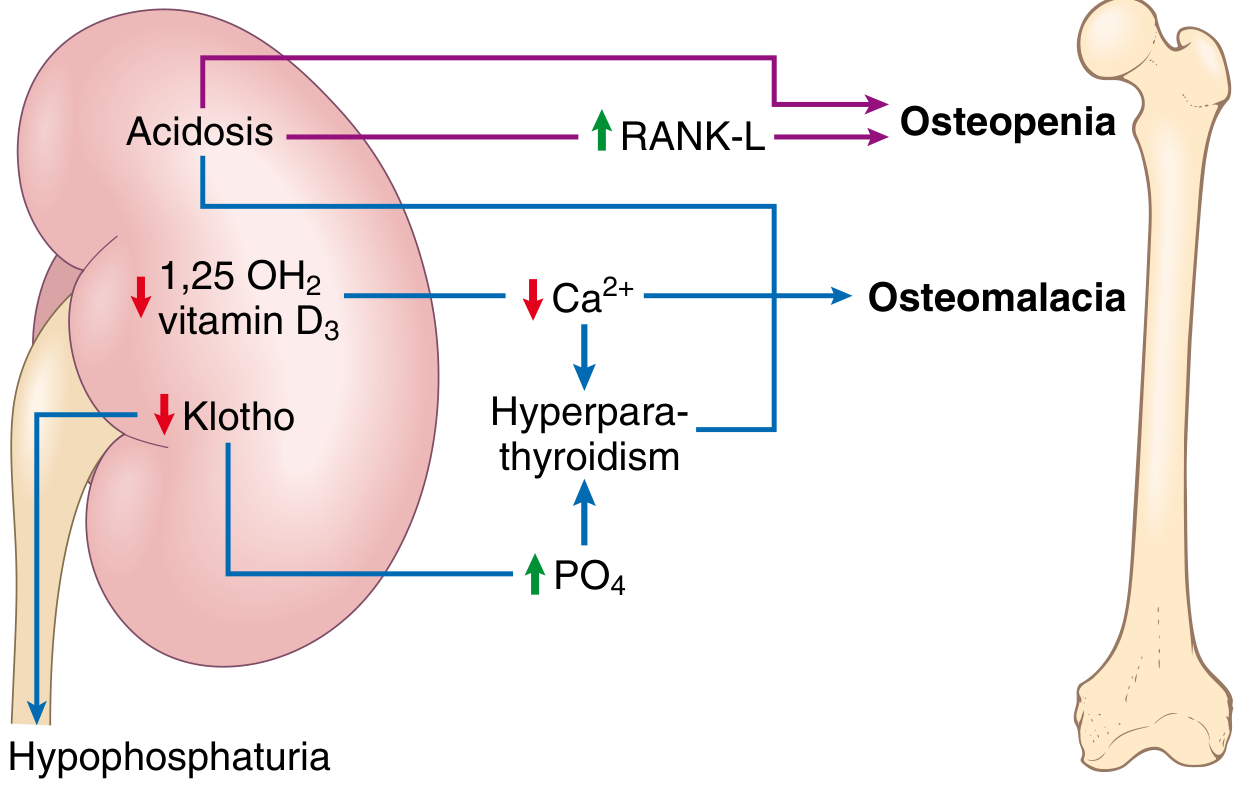
1. Calcium Metabolism Disturbances
- Total serum calcium falls as GFR decreases due to phosphate retention, decreased renal 1,25-(OH)2D3 synthesis, reduced intestinal calcium absorption, and skeletal resistance to PTH
- Free calcium levels stay normal initially due to compensatory hyperparathyroidism
- Persistent hypocalcemia is a powerful continuous stimulus for PTH hypersecretion and parathyroid gland hyperplasia
2. Phosphate Retention and FGF-23
- With progressive CKD, the kidney retains phosphate (hyperphosphatemia becomes overt at stage 4 CKD)
- Early compensation involves increased FGF-23 (secreted by osteocytes), which promotes phosphaturia - but this comes at the cost of suppressing 1α-hydroxylase, further reducing calcitriol synthesis
- Decreased renal expression of Klotho (the FGF-23 co-receptor) impairs phosphate handling, creates FGF-23 resistance, and directly suppresses calcitriol
3. Vitamin D Deficiency
- The kidney performs the crucial second hydroxylation step (25-OH-D → 1,25-(OH)2D3, calcitriol)
- Impaired calcitriol synthesis → reduced intestinal Ca2+ absorption → hypocalcemia → elevated PTH
- Calcitriol also directly suppresses PTH gene transcription and is needed for osteoblast/osteoclast maturation
4. Secondary Hyperparathyroidism (High-Turnover Disease)
- The combined effects of hypocalcemia, hyperphosphatemia, calcitriol deficiency, and Klotho reduction drive parathyroid hyperplasia
- Parathyroid glands show decreased expression of Vitamin D receptors, calcium-sensing receptors, and α-Klotho
- An elevated "set-point" for calcium-regulated PTH secretion develops
- PTH drives increased osteoclast and osteoblast activity → osteitis fibrosa
5. Tubular Dysfunction and Acidosis
- Tubular and systemic acidosis increases RANKL expression on osteoblasts → increased osteoclast recruitment and bone matrix resorption → osteopenia
- Acidosis also impairs mineralization
6. Aluminum Toxicity (Low-Turnover Disease)
- Historically, aluminum-containing phosphate binders and aluminum-contaminated dialysate were major causes
- Aluminum deposits at the mineralization front, blocking further hydroxyapatite crystal growth → osteomalacia
- Aluminum also directly suppresses osteoblast activity → adynamic bone disease
7. Adynamic Bone Disease - Low-Turnover
- Increasingly prevalent, especially in diabetic and elderly dialysis patients, and those on peritoneal dialysis
- Caused by over-suppression of PTH (excess calcium/vitamin D supplementation), aluminum toxicity, diabetes mellitus, and aging
- Characterized by absent or minimal osteoblast/osteoclast activity - the bone cannot respond to microfractures
8. β2-Microglobulin Amyloidosis (Aβ2M)
- In long-term dialysis patients (>10 years), β2-microglobulin accumulates and deposits as amyloid in synovial membranes, joints, and bone, causing destructive arthropathy and cyst formation
Pathology
Histological Types
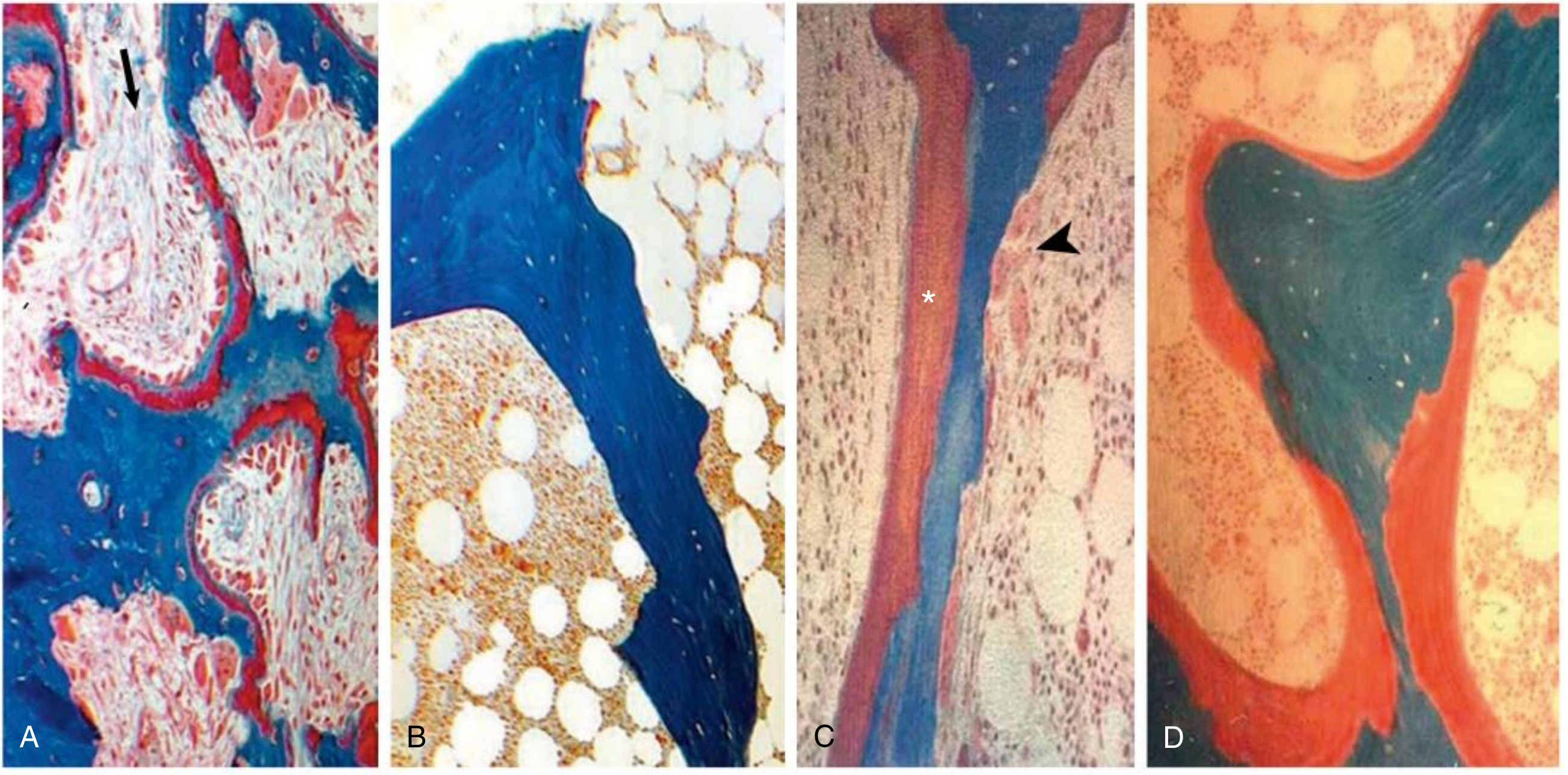
Osteitis Fibrosa (High-Turnover)
- Increased osteoclast AND osteoblast numbers and activity
- Peritrabecular fibrosis (replacement of marrow by fibrous tissue)
- Woven (disorganized) osteoid rather than lamellar
- In severe cases: brown tumors (collections of osteoclasts, fibroblasts, and hemosiderin-laden macrophages in lytic cavities)
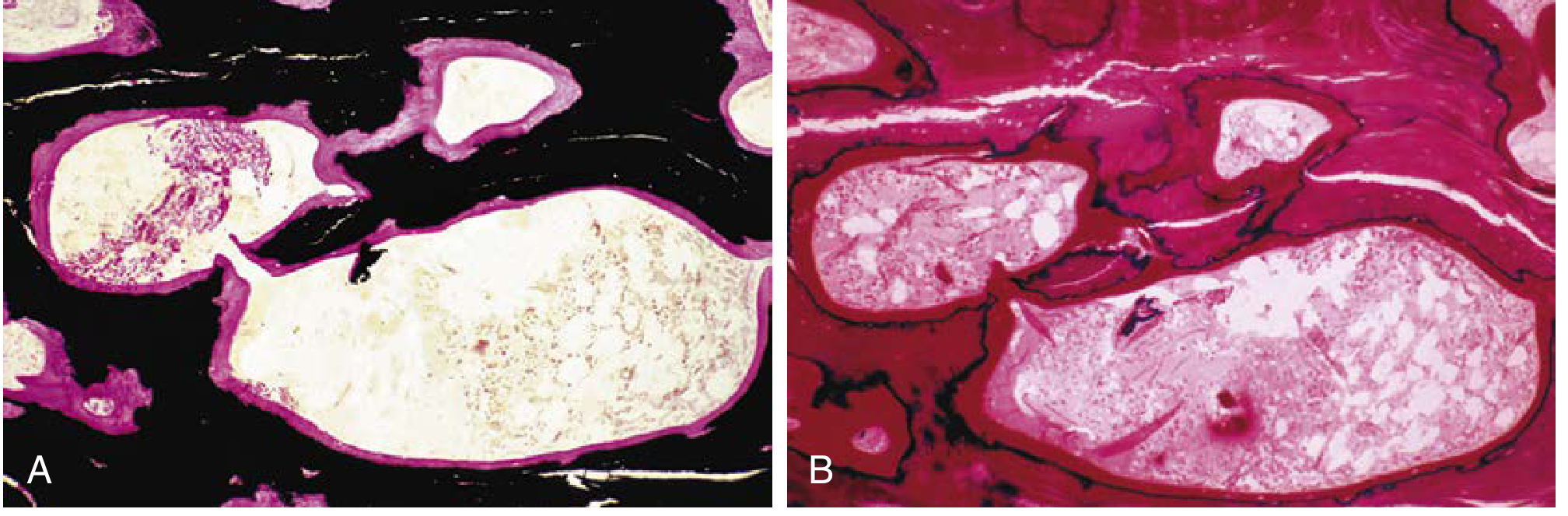
Osteomalacia (Low-Turnover)
- Increased osteoid seam width (unmineralized bone matrix accumulates)
- Increased trabecular surface covered by osteoid
- Decreased bone mineralization (assessed by tetracycline double-labeling)
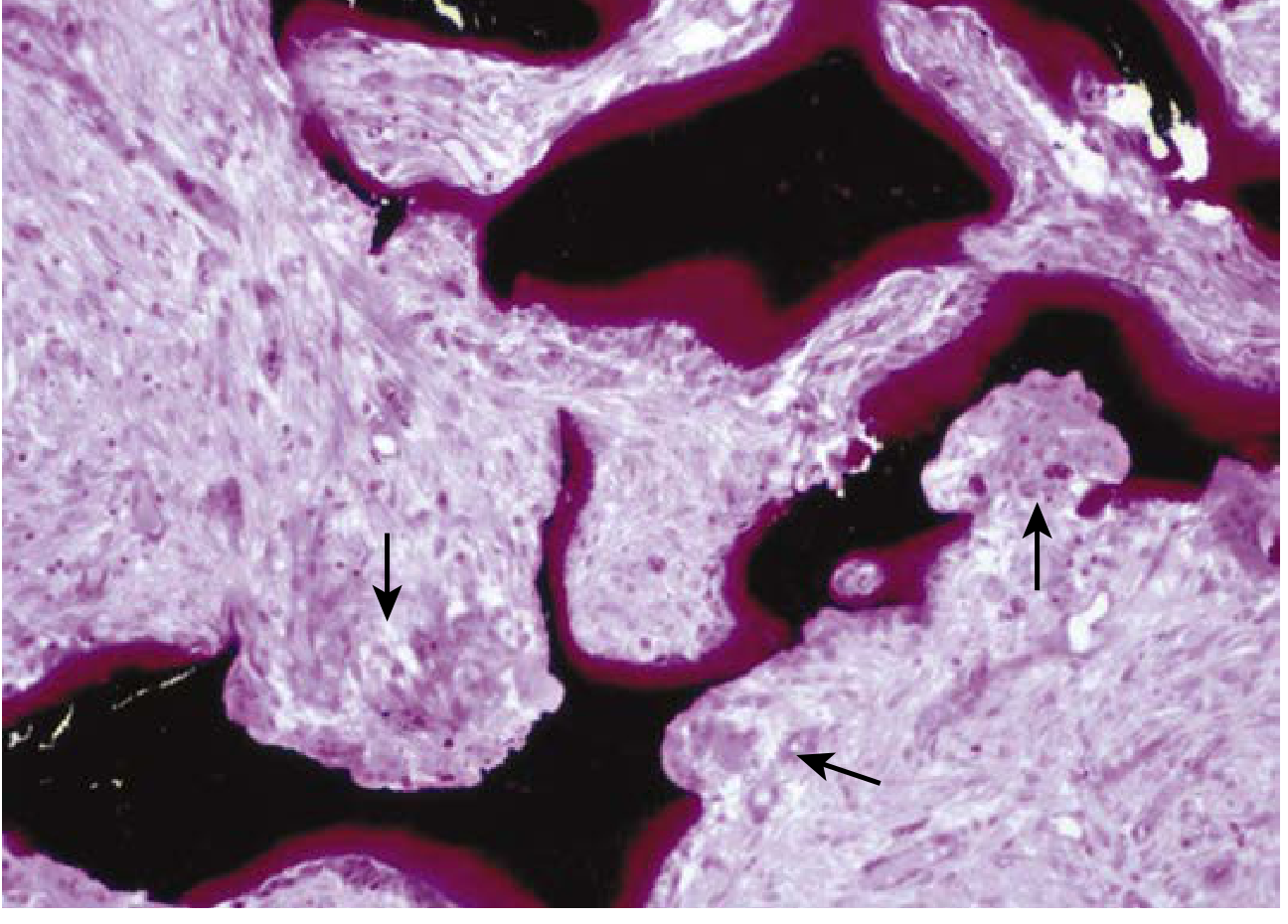
- Von Kossa stain: mineralized bone = black; osteoid = magenta/red
Aluminum-related bone disease is defined histologically as:
- Aluminum staining >15% of the trabecular surface
- Bone formation rate <220 mm²/day
Adynamic Bone Disease (Low-Turnover)
- No osteoclastic or osteoblastic cellular activity
- No osteoid visible on biopsy
- Bone cannot respond to microdamage → fragility fractures
Von Kossa stain and tunneling resorption in osteitis fibrosa with osteomalacia:
Epidemiology
- Skeletal abnormalities can begin at eGFR ~50 mL/min/1.73 m2 (CKD stage 3)
- In hemodialysis patients: osteitis fibrosa is declining, ABD is increasing (especially in White patients)
- In Black dialysis patients: osteitis fibrosa remains dominant
- In peritoneal dialysis patients, diabetics, and elderly: ABD has been dominant for decades
- Osteomalacia represents a small fraction but is more common in South Asians Comprehensive Clinical Nephrology, 7th Ed., p. 1180
Signs and Symptoms
Skeletal Manifestations
- Bone pain - non-specific aches and pains in the lower back, hips, and legs; aggravated by weight-bearing; can be debilitating
- Acute localized bone pain - may mimic acute arthritis
- Pathological fractures - especially of long bones; vertebral fractures cause kyphoscoliosis or chest deformities
- Subperiosteal erosions - on radiographs, particularly at radial aspect of middle phalanges (classic site)
- Resorption of terminal digits (acro-osteolysis)
- Brown tumors - lytic lesions, can be confused with bone metastases
- Slipped epiphyses - particularly in children
- Growth retardation - in children with CKD
- Deformities - resulting from fractures and bone softening
Muscle and Joint Manifestations
- Proximal muscle weakness - gradual onset; multifactorial (PTH excess, vitamin D deficiency, uremic myopathy)
- Periarthritis - peri-articular calcium phosphate crystal deposition, especially with hyperphosphatemia; mimics gout or pseudogout; responds to NSAIDs
- Carpal tunnel syndrome and destructive arthropathy - in β2-microglobulin amyloidosis (long-term dialysis)
Extraskeletal Calcifications
- Vascular calcification - arterial wall calcification; major contributor to cardiovascular mortality
- Pulmonary calcification - can cause restrictive lung disease
- Myocardial calcification
- Periarticular calcification - "tumoral calcinosis" pattern
- Calciphylaxis (calcific uremic arteriolopathy) - rare but life-threatening; painful skin necrosis from calcification of small dermal vessels
Skin Manifestations
- Pruritus - related to hyperparathyroidism and calcium-phosphate deposition in skin
- Calciphylaxis causes painful, necrotic skin lesions with a livedo pattern
Investigations
1. Serum Biochemistry
| Test | Finding | Significance |
|---|---|---|
| Serum calcium | Normal (early) → Low (stage 4+) | Hypocalcemia drives PTH |
| Serum phosphate | Normal → Elevated (stage 4+) | Drives FGF-23, suppresses calcitriol |
| Intact PTH (iPTH) | Elevated | Surrogate for high-turnover disease; >600 pg/mL = osteitis fibrosa in dialysis |
| Alkaline phosphatase (ALP) | Elevated | Reflects osteoblastic activity |
| Bone-specific ALP (BAP) | Elevated | More specific marker of bone formation |
| 25-hydroxyvitamin D | Low | Assess vitamin D status; <30 ng/mL requires correction |
| 1,25-(OH)2D3 (calcitriol) | Low | Not useful for differentiating ROD subtypes |
| FGF-23 | Elevated early | Rises before phosphate becomes elevated |
| Serum aluminum | Elevated if exposure | Confirms aluminum-related bone disease |
| Bicarbonate | Low | Metabolic acidosis contributes |
Key notes on PTH assays:
- Two-site immunometric ("intact" PTH) assays also measure large N-terminally truncated fragments
- "Biointact" PTH (1-84) assays are more specific but not clearly superior clinically
- KDIGO target for dialysis patients: iPTH approximately 2-9x the upper limit of normal for the assay used
- Serial PTH measurements are essential - trends are as important as absolute values
- In CKD stages 3-5, progressive rises above normal should be addressed
2. Radiological Investigations
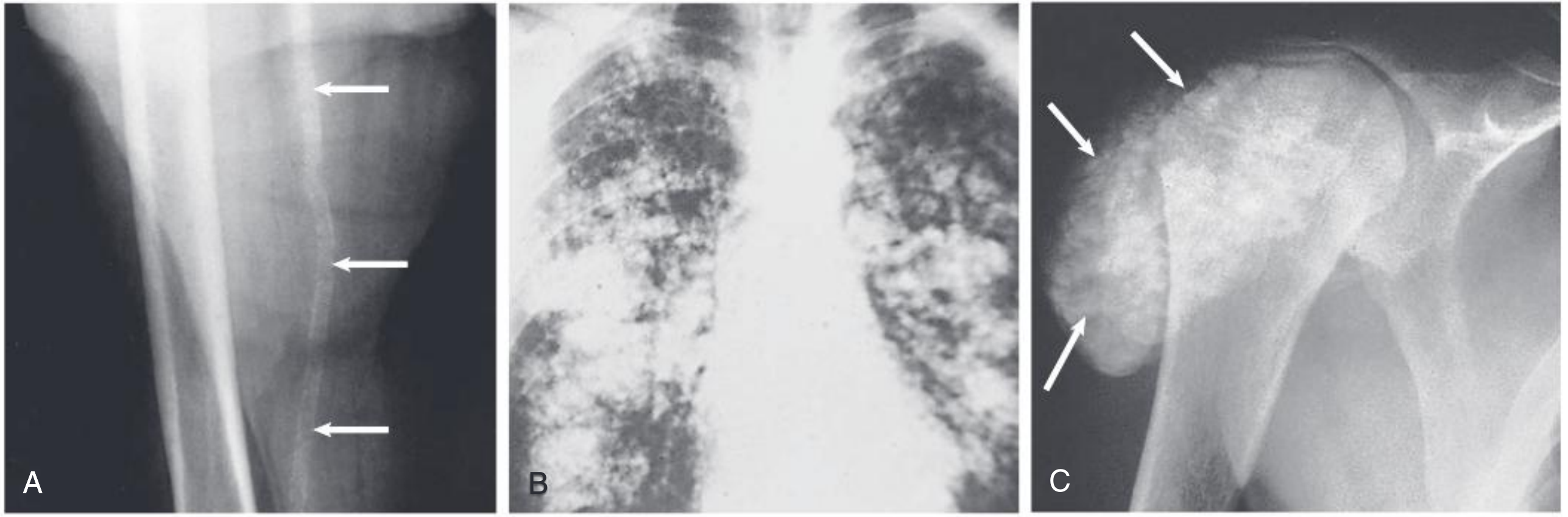
Plain X-rays (hands, spine, skull)
- Subperiosteal bone resorption at radial aspect of middle phalanges (pathognomonic of hyperparathyroidism)
- Salt and pepper skull - granular mottling from patchy resorption
- Rugger jersey spine - alternating bands of sclerosis and lucency
- Brown tumors - well-defined lytic lesions
- Looser's zones / pseudofractures - linear lucencies perpendicular to the cortex in osteomalacia
- Acro-osteolysis - resorption of terminal phalanges
- Periosteal reaction (in children)
- Vascular and soft tissue calcifications
Radiologically, the features of secondary hyperparathyroidism include osteosclerosis, acro-osteolysis, and subperiosteal bone resorption (Grainger & Allison's Diagnostic Radiology).
DEXA (Dual-energy X-ray absorptiometry)
- Measures bone mineral density (BMD)
- Does not distinguish between types of ROD
- Useful for monitoring osteopenia/osteoporosis
Bone Scintigraphy (Tc-99m)
- Increased uptake in areas of high turnover or calcification
- Can identify brown tumors and soft tissue calcification sites
3. Bone Biopsy (Gold Standard)
Bone biopsy remains the definitive investigation for diagnosing the specific type of renal osteodystrophy and is the most reliable guide for treatment decisions. It is performed on the iliac crest after double tetracycline labeling (two courses of tetracycline 14 days apart, with biopsy 3-5 days after the second course).
Histomorphometry assesses:
- Bone turnover - via dynamic tetracycline-based measurements (bone formation rate, activation frequency)
- Mineralization - osteoid volume, osteoid thickness, mineralization lag time
- Bone volume - trabecular bone volume per tissue volume
- Aluminum - stained with solochrome azurine or Perl's stain; >15% trabecular surface = aluminum-related disease
Biopsy is indicated when:
- PTH in the recommended range but bone-specific ALP is elevated
- Hypercalcemia with only modestly elevated PTH
- Significant bone pain without clear biochemical cause
- Before parathyroidectomy when etiology is uncertain
4. Other Tests
- Serum β2-microglobulin - elevated in amyloidosis
- MRI of joints - for β2-microglobulin amyloid deposits (destructive spondyloarthropathy)
- Parathyroid ultrasound / Sestamibi scan - for tertiary hyperparathyroidism, pre-surgical localization
- Serum aluminum level and deferoxamine stimulation test - if aluminum toxicity suspected
Treatment
Prevention is the primary goal. Ideally therapy should begin at CKD stage 3, before significant parathyroid hyperplasia develops.
1. Dietary Modification
- Phosphate restriction: Limit dairy products, processed foods with added phosphate, and protein-rich foods (but avoid <0.8 g/kg/day protein to prevent malnutrition)
- Calcium supplementation: Calcium carbonate taken between meals as the initial approach to hypocalcemia in mild-moderate CKD
2. Control of Phosphate (Cornerstone of Management)
Phosphate Binders (taken with meals to bind dietary phosphate):
| Type | Examples | Notes |
|---|---|---|
| Calcium-based | Calcium carbonate, calcium acetate | Effective; risk of hypercalcemia with high doses |
| Non-calcium, non-aluminum | Sevelamer carbonate, lanthanum carbonate | Preferred in hypercalcemia, vascular calcification |
| Aluminum-based | Aluminum hydroxide | Highly effective but causes aluminum bone disease; avoid long-term |
| Iron-based | Ferric citrate, sucroferric oxyhydroxide | Added benefit of iron supplementation |
3. Vitamin D Therapy
- 25-hydroxyvitamin D deficiency (<30 ng/mL): Correct with ergocalciferol or cholecalciferol
- Active vitamin D sterols (calcitriol, alfacalcidol, paricalcitol, doxercalciferol): Used in CKD 3-5D when PTH remains elevated despite correction of hypocalcemia and vitamin D deficiency
- These directly suppress PTH gene transcription and reduce parathyroid hyperplasia
- Selective vitamin D receptor activators (paricalcitol): Have less hypercalcemia and hyperphosphatemia than calcitriol; may have additional cardiovascular benefits
- Goal in dialysis patients: Achieve iPTH ~2-9x the upper limit of normal (to avoid over-suppression and ABD)
4. Calcimimetics
- Cinacalcet (oral), etelcalcetide (IV, administered with dialysis), evocalcet (Japan): Target the calcium-sensing receptor, increasing its sensitivity to calcium → reduces PTH secretion
- Especially useful when PTH is elevated with concurrent hypercalcemia or hyperphosphatemia (since calcimimetics lower Ca and P as well as PTH)
- Can be combined with low-dose active vitamin D for synergistic effect
- Side effects: Hypocalcemia, nausea/vomiting (less with etelcalcetide on nausea profile)
- Cinacalcet significantly reduces rates of parathyroidectomy and calciphylaxis
- Not recommended in pre-dialysis CKD due to phosphate retention risk
5. Treatment of Adynamic Bone Disease
- Reduce or stop calcium supplements
- Reduce active vitamin D doses
- Allow PTH to rise slightly to stimulate bone formation
- Avoid oversuppression of PTH below target ranges
6. Treatment of Aluminum-Related Bone Disease
- Eliminate aluminum exposure (switch phosphate binders)
- Deferoxamine (DFO) chelation therapy: Binds aluminum and promotes its dialytic removal; indicated when serum aluminum is markedly elevated or aluminum staining on biopsy is significant. Risk of serious infections (mucormycosis) limits its use.
7. Treatment of β2-Microglobulin Amyloidosis
- High-flux dialysis membranes and hemodiafiltration enhance β2-microglobulin clearance
- Renal transplantation - restores normal kidney function and halts amyloid deposition
8. Parathyroidectomy
Indications:
- Severe, refractory hyperparathyroidism failing medical therapy (iPTH often >1000 pg/mL)
- Persistent hypercalcemia from autonomous parathyroid function (tertiary hyperparathyroidism)
- Calciphylaxis with elevated PTH (urgent indication)
- Severe metastatic calcification
- Before kidney transplantation with significant osteopenia or frank hypercalcemia
Surgical options:
- Subtotal parathyroidectomy (3.5 glands removed)
- Total parathyroidectomy with autotransplantation (forearm muscle)
Post-operative "hungry bone syndrome" - severe hypocalcemia due to avid bone recalcification - must be anticipated and treated with IV calcium and vitamin D.
9. Renal Transplantation
- The most effective long-term treatment for all forms of renal osteodystrophy
- Restores calcitriol production, phosphate regulation, and suppresses PTH
- Post-transplant bone loss in the first year is common due to corticosteroid immunosuppression
- Persistent hyperparathyroidism for up to 12 months post-transplant is expected; mild hypercalcemia may resolve spontaneously
Summary Table: Key Features by ROD Type
| Feature | Osteitis Fibrosa | Osteomalacia | Adynamic Bone Disease |
|---|---|---|---|
| Turnover | High | Low | Very Low (absent) |
| PTH | Very high (>600 pg/mL) | Normal/Low | Low/Normal (suppressed) |
| ALP | Elevated | Elevated | Normal/Low |
| Osteoid | Woven, increased | Markedly increased (thick seams) | Absent |
| Osteoclasts | Numerous | Few (osteoid blocks entry) | Absent |
| Fibrosis | Peritrabecular | Absent | Absent |
| Aluminum | Absent | Present (at mineralization front) | May be present |
| Treatment | Vitamin D + cinacalcet ± parathyroidectomy | Remove aluminum; DFO | Reduce Ca/VitD suppression |
Sources:
- Comprehensive Clinical Nephrology, 7th Ed., Chapter 88 (CKD-MBD and Renal Osteodystrophy)
- Robbins, Cotran & Kumar Pathologic Basis of Disease (Metabolic Diseases of Bone)
- Henry's Clinical Diagnosis and Management by Laboratory Methods (Metabolic Bone Disease)
- Brenner and Rector's The Kidney (CKD-MBD, TMV Classification)
- Grainger & Allison's Diagnostic Radiology (Radiological features of ROD)
This is a shared conversation. Sign in to Orris to start your own chat.