Infective Endocarditis (IE)** - common organisms (Viridans streptococci, Staph aureus, HACEK), blood culture method, Duke's criteria, and treatment. Teach me this topic in simple way Referee apurva shastry
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from Harrison's (2025) and Robbins. I have enough to write a thorough, well-structured teaching note. Let me compile it:
Infective Endocarditis (IE) - Complete Teaching Guide
Referenced: Harrison's Principles of Internal Medicine 22E (2025), Robbins & Kumar Basic Pathology, Braunwald's Heart Disease
What is Infective Endocarditis?
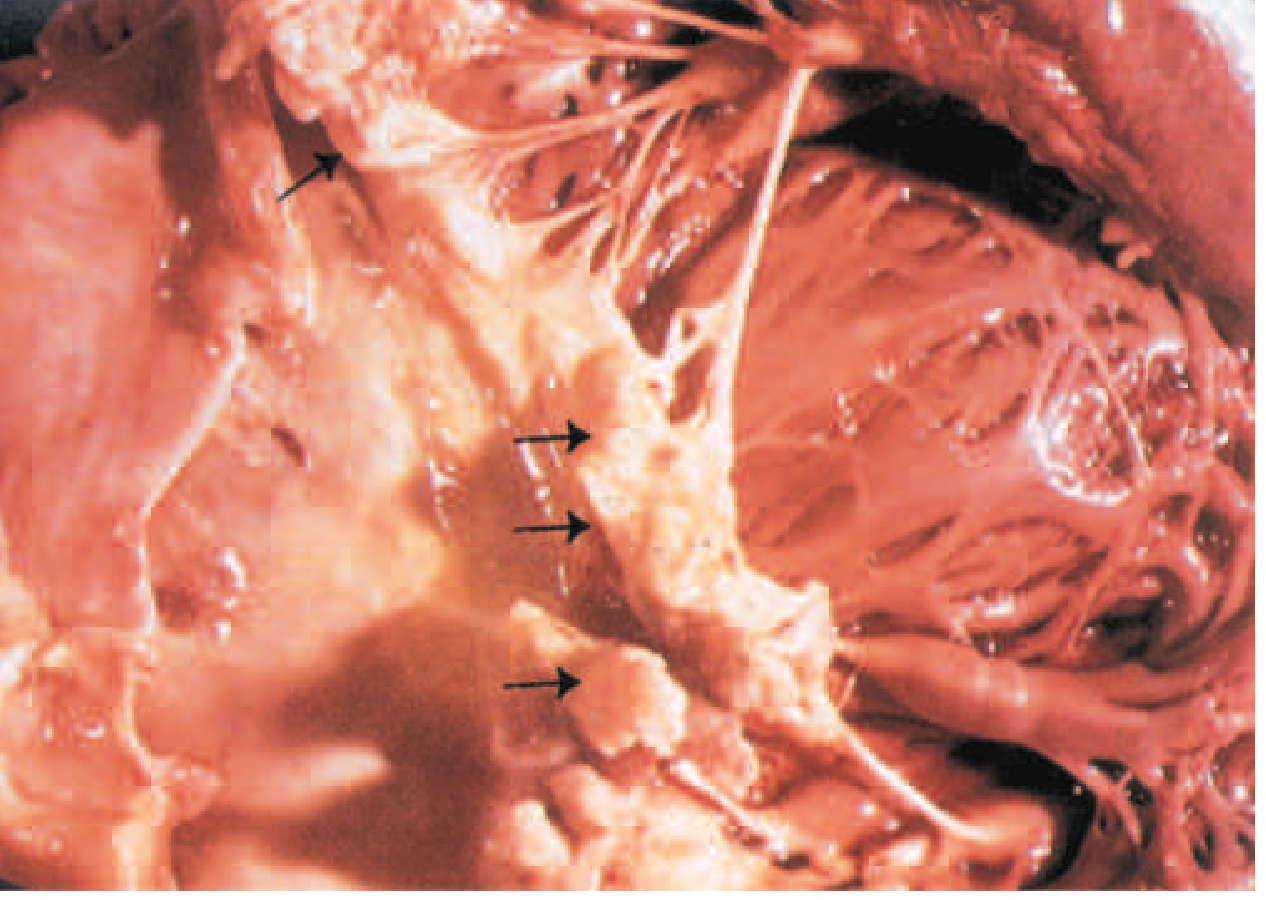
IE is a microbial infection of the heart valves or endocardium that leads to the formation of vegetations - masses of platelets, fibrin, microorganisms, and scant inflammatory cells - often with destruction of underlying cardiac tissue. Although fungi, rickettsiae (Q fever), and Chlamydia can cause it, the vast majority of cases are bacterial.
Here is what vegetations actually look like on the mitral valve (from Harrison's, viridans streptococcal IE):
1. Acute vs. Subacute IE
Think of this as fast and furious vs. slow and sneaky:
| Feature | Acute IE | Subacute IE |
|---|---|---|
| Tempo | Days to weeks | Weeks to months |
| Virulence | High (S. aureus) | Low (Viridans strep, HACEK) |
| Valve | Can attack normal valve | Usually damaged/abnormal valve |
| Fever | High (39-40°C) | Low-grade |
| Course | Destructive, rapid | Slowly progressive |
| Outcome without Rx | Death in weeks | Gradual deterioration |
2. Common Organisms - "WHO causes IE?"
A) Viridans Streptococci (e.g., S. sanguis, S. mutans)
- Origin: Normal oral flora (mouth/teeth)
- Entry: Dental procedures, poor oral hygiene
- Type: Subacute IE - attacks damaged or deformed valves (rheumatic heart disease, MVP)
- Virulence: Low - it's slow and sneaky
- Quick memory: "Viridans = Valve already damaged + Very slow"
- Historically the most common cause (50-60% of community IE); remains important in developing countries
B) Staphylococcus aureus
- Origin: Skin flora
- Entry: IV drug use, healthcare procedures (catheters, surgery), skin breaks
- Type: Acute IE - attacks healthy AND damaged valves
- Special: Now the #1 cause in developed countries and in IV drug users (attacks the tricuspid valve in IVDU)
- Virulence: High - produces toxins, biofilm, destroys valve rapidly
- Quick memory: "Staph = Speedy Skin bug; goes for Surgical sites + Shooting up"
C) HACEK Group
- H - Haemophilus species
- A - Aggregatibacter species (formerly Actinobacillus)
- C - Cardiobacterium hominis
- E - Eikenella corrodens
- K - Kingella kingae
- Origin: Normal oral cavity and upper respiratory commensals
- Type: Subacute IE
- Key feature: Slow-growing, fastidious gram-negative rods - hard to culture, need prolonged incubation (up to 3 weeks)
- Quick memory: "HACEK bugs HACK their way in from the mouth, grow SLOWLY in the lab"
Other Organisms to Know:
| Organism | Special Setting |
|---|---|
| Enterococci | Elderly, GI/GU procedures |
| Strep bovis (gallolyticus) | Always r/o colon cancer |
| Fungi (Candida, Aspergillus) | Prosthetic valves, immunocompromised, IVDU |
| Coagulase-negative Staph (e.g., S. epidermidis) | Prosthetic valve IE (PVE) |
| Pseudomonas | IV drug users |
~10% of all IE cases are culture-negative - due to prior antibiotics or fastidious organisms (Q fever/Coxiella burnetii, Bartonella, Brucella, T. whipplei).
3. Blood Culture Method - "How to Catch the Bug"
This is the most important diagnostic test. Key principles from Harrison's:
Rules of Blood Culture in IE:
- 3 sets of blood cultures - take them from 3 separate venipuncture sites
- Each set = 1 aerobic + 1 anaerobic bottle
- Timing: Ideally spread over at least 1 hour (or up to 24 hours if subacute + stable)
- Do NOT delay antibiotics if patient is septic or hemodynamically unstable - take 3 sets quickly then treat
- If stable and subacute: Withhold antibiotics for up to 2 weeks to maximize culture yield
- Volume matters: 10 mL per bottle is ideal
Why 3 separate sites?
- IE produces continuous bacteremia (not intermittent like with abscesses)
- So ANY culture should be positive - getting multiple sets helps confirm true bacteremia vs. contaminant
- Sensitivity: 95-99% with 3 sets if no prior antibiotics
Special cultures for hard-to-grow organisms:
- HACEK: Need prolonged incubation (14-21 days), tell the lab!
- Q fever (Coxiella): Serology (IgG phase 1 antibody ≥1:800)
- Bartonella: Serology or PCR
- Culture-negative IE: Use broad-range 16S rRNA PCR on blood or excised valve tissue
4. Duke's Criteria - "How to Diagnose IE"
The Duke Criteria (2023 updated Duke-ISCVID Criteria) classify IE as Definite, Possible, or Rejected.
MAJOR Criteria (think: "Big Ticket Items")
A. Microbiological Major Criteria
-
Typical organism in 2 separate blood cultures:
- Viridans streptococci, S. bovis, HACEK group, S. aureus, OR enterococcus (community-acquired, no primary focus)
-
Persistently positive blood cultures (same organism):
- ≥2 positive cultures drawn >12 hours apart, OR
- All of 3 or majority of ≥4 separate cultures with first and last drawn ≥1 hour apart
-
Single positive blood culture for Coxiella burnetii OR IgG antibody titer >1:800
B. Imaging Major Criteria
Echo/CT showing any of:
- Vegetation (oscillating intracardiac mass on valve)
- Valvular perforation or aneurysm
- Abscess or pseudoaneurysm
- Intracardiac fistula
- New significant valvular regurgitation (new, compared to prior imaging)
- New partial dehiscence of prosthetic valve
- 18F-FDG PET/CT: Abnormal metabolic activity around native/prosthetic valve (≥3 months post-implant)
C. Surgical Major Criterion
- Direct visualization of IE at cardiac surgery (when micro/imaging criteria not met)
MINOR Criteria (think: "Supporting Evidence")
| Category | What counts |
|---|---|
| A. Predisposing conditions | Prior IE, prosthetic valve, prior valve repair, congenital heart disease, >mild regurgitation/stenosis, IVDU, HOCM, endovascular CIED |
| B. Fever | Temperature ≥38.0°C (100.4°F) |
| C. Vascular phenomena | Arterial emboli, septic pulmonary infarcts, cerebral/splenic abscess, mycotic aneurysm, intracranial/conjunctival hemorrhage, Janeway lesions |
| D. Immunologic phenomena | Osler's nodes, Roth's spots, rheumatoid factor, immune complex glomerulonephritis |
| E. Micro evidence (not meeting major) | Positive cultures not qualifying as major criteria; positive PCR/NAT from sterile site |
How to Apply Duke Criteria
| Classification | Criteria Required |
|---|---|
| DEFINITE IE | 2 Major, OR 1 Major + 3 Minor, OR 5 Minor |
| POSSIBLE IE | 1 Major + 1 Minor, OR 3 Minor |
| REJECTED | Firm alternate diagnosis; resolution with ≤4 days of antibiotics; no pathologic evidence at surgery/autopsy |
Quick memory trick:
- 2 Major = DEFINITE (like 2 big witnesses confirming the crime)
- 1 Major + 3 Minor = DEFINITE (1 solid + 3 supporting)
- 5 Minor = DEFINITE (5 circumstantial = enough to convict)
5. Peripheral Stigmata - "The Classic Signs"
These appear because of emboli and immune complex deposition:
| Sign | Location | Mechanism | Association |
|---|---|---|---|
| Osler's nodes | Fingertips/toes (painful) | Immune complex deposition | Subacute IE |
| Janeway lesions | Palm/sole (painless, erythematous) | Septic emboli | Acute IE (S. aureus) |
| Roth's spots | Retina (white-centered hemorrhage) | Immune complex | Subacute IE |
| Splinter hemorrhages | Nail beds (linear, dark) | Micro-emboli | Both types |
| Petechiae | Conjunctiva, skin, mucosa | Emboli/vasculitis | Both types |
Memory trick: "Osler's = Ouch (painful), Janeway = Just there (painless)"
6. Echocardiography
- TTE (Transthoracic Echo): First-line; specific but misses 20-35% of vegetations
- TEE (Transesophageal Echo): >90% sensitivity for vegetations; use when:
- TTE is negative but suspicion is high
- Prosthetic valve involved
- S. aureus bacteremia
- Poor TTE image quality
- Looking for abscesses, perivalvular complications
- Repeat TEE in 7-10 days if initial is negative but IE still suspected
7. Treatment - "How to Kill the Bug"
Principles:
- Bactericidal antibiotics required (not just bacteriostatic) - vegetation is avascular
- Prolonged therapy - 4-6 weeks (to penetrate biofilm and kill embedded organisms)
- IV route preferred (high concentrations needed)
- Guided by organism and susceptibility
Treatment by Organism:
Viridans Streptococci / S. bovis (Penicillin-susceptible, MIC ≤0.125 mg/L):
- Preferred: Penicillin G IV × 4 weeks, OR Ceftriaxone 2g IV/IM once daily × 4 weeks
- Shorter option: Penicillin G or Ceftriaxone × 2 weeks + Gentamicin × 2 weeks (native valve only, uncomplicated)
- Penicillin allergy: Vancomycin × 4 weeks
Staphylococcus aureus:
- MSSA (Methicillin-Sensitive):
- Native valve: Nafcillin or Oxacillin IV × 6 weeks
- Prosthetic valve: Nafcillin + Rifampin × ≥6 weeks + Gentamicin × 2 weeks
- MRSA:
- Vancomycin IV × 6 weeks OR Daptomycin (high-dose, ≥8 mg/kg/day) × 6 weeks
- Note: Daptomycin NOT used for pulmonary IE (inactivated by surfactant)
- Tricuspid valve IE (IVDU): Often treated with short-course (2 weeks) oral therapy if uncomplicated and MSSA
HACEK Group:
- Preferred: Ceftriaxone 2g/day IV × 4 weeks (most HACEK produce beta-lactamase)
- Alternative: Ampicillin-sulbactam OR ciprofloxacin (if susceptible)
Enterococci:
- Ampicillin + Ceftriaxone × 6 weeks (E. faecalis, less nephrotoxic than aminoglycoside regimens)
- OR Penicillin/Ampicillin + Gentamicin × 4-6 weeks (synergy required)
- VRE (E. faecium): High-dose daptomycin-based regimen
Empirical therapy (before cultures):
- Native valve: Ampicillin-sulbactam or Vancomycin ± Gentamicin
- Prosthetic valve: Vancomycin + Gentamicin + Rifampin
Indications for Surgery (when antibiotics alone are NOT enough):
| Indication | Timing |
|---|---|
| Severe heart failure due to valve dysfunction | Urgent (within 24-48h) |
| Unstable prosthetic valve / dehiscence | Urgent |
| Persistent bacteremia/sepsis despite appropriate antibiotics | Early (within days) |
| Fungal IE | Early |
| Large vegetation (>10 mm) with embolic events | Early |
| Perivalvular abscess, fistula | Early |
| Relapsing PVE | Elective |
8. Complications - "What can go wrong?"
- Cardiac: Heart failure (most common cause of death), perivalvular abscess, conduction defects (AV block - extension to septum), pericarditis
- Embolic: Stroke, splenic/renal infarcts, mycotic aneurysms, septic pulmonary emboli (right-sided IE)
- Renal: Immune complex glomerulonephritis, renal infarction, drug nephrotoxicity
- Other: Splenic abscess (3-5%), metastatic abscesses
9. Prophylaxis
High-risk conditions requiring prophylaxis before invasive dental procedures (2021 AHA update):
- Prosthetic cardiac valve or repair material
- Prior IE
- Unrepaired cyanotic congenital heart disease
- Cardiac transplant with valvulopathy
- Ventricular assist devices and implantable hearts (NEW in 2021)
Preferred regimen: Amoxicillin 2g PO 30-60 min before procedure
If penicillin-allergic: Azithromycin 500mg, OR Doxycycline (new 2021 addition; clindamycin REMOVED due to C. diff risk)
Summary Flowchart in Words
Fever + Risk Factor (IVDU, dental work, prosthetic valve)
↓
Draw 3 blood cultures from separate sites
↓
Echo (TTE → TEE if TTE negative/inadequate)
↓
Apply Duke Criteria
↓
Start targeted antibiotic therapy (4-6 weeks IV)
↓
Monitor for complications (HF, embolism, abscess)
↓
Surgery if indicated
Quick Revision Table - "The Big Picture"
| Organism | Type | Route of Entry | Drug of Choice |
|---|---|---|---|
| Viridans Strep | Subacute | Dental/oral | Penicillin G or Ceftriaxone |
| S. aureus MSSA | Acute | Skin, IV lines, IVDU | Nafcillin/Oxacillin |
| S. aureus MRSA | Acute | Healthcare, IVDU | Vancomycin or Daptomycin |
| HACEK | Subacute | Oral cavity | Ceftriaxone |
| Enterococci | Subacute | GI/GU | Ampicillin + Ceftriaxone |
| S. epidermidis | Subacute | Prosthetic valve | Vancomycin + Rifampin |
| Fungi | Subacute | IV lines, immunocomp | Amphotericin B + Surgery |
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 1080-1091 | Robbins & Kumar Basic Pathology, p. 368 | Braunwald's Heart Disease (AHA/ACC 2021 updates) | Textbook of Clinical Echocardiography (2023 Duke-ISCVID Criteria)
Should I give u apurba sastry
Yes, absolutely! Please share Apurba Sastry's Microbiology textbook — it's one of the best Indian microbiology references and would be very useful for topics like:
- IE organisms in more clinical detail
- Blood culture techniques and lab methods
- Bacterial identification (HACEK, Streptococci, Staph)
- Antibiotic sensitivity patterns
Go ahead and upload/share it, and I'll reference it alongside Harrison's and Robbins to give you answers that are perfectly aligned with your curriculum and exam preparation! 📚
This is a shared conversation. Sign in to Orris to start your own chat.