Glocoma reason, treatment and complications
Reading File
Finding Sources
Searching PubMed
glaucoma treatment management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Glaucoma: Causes, Treatment, and Complications
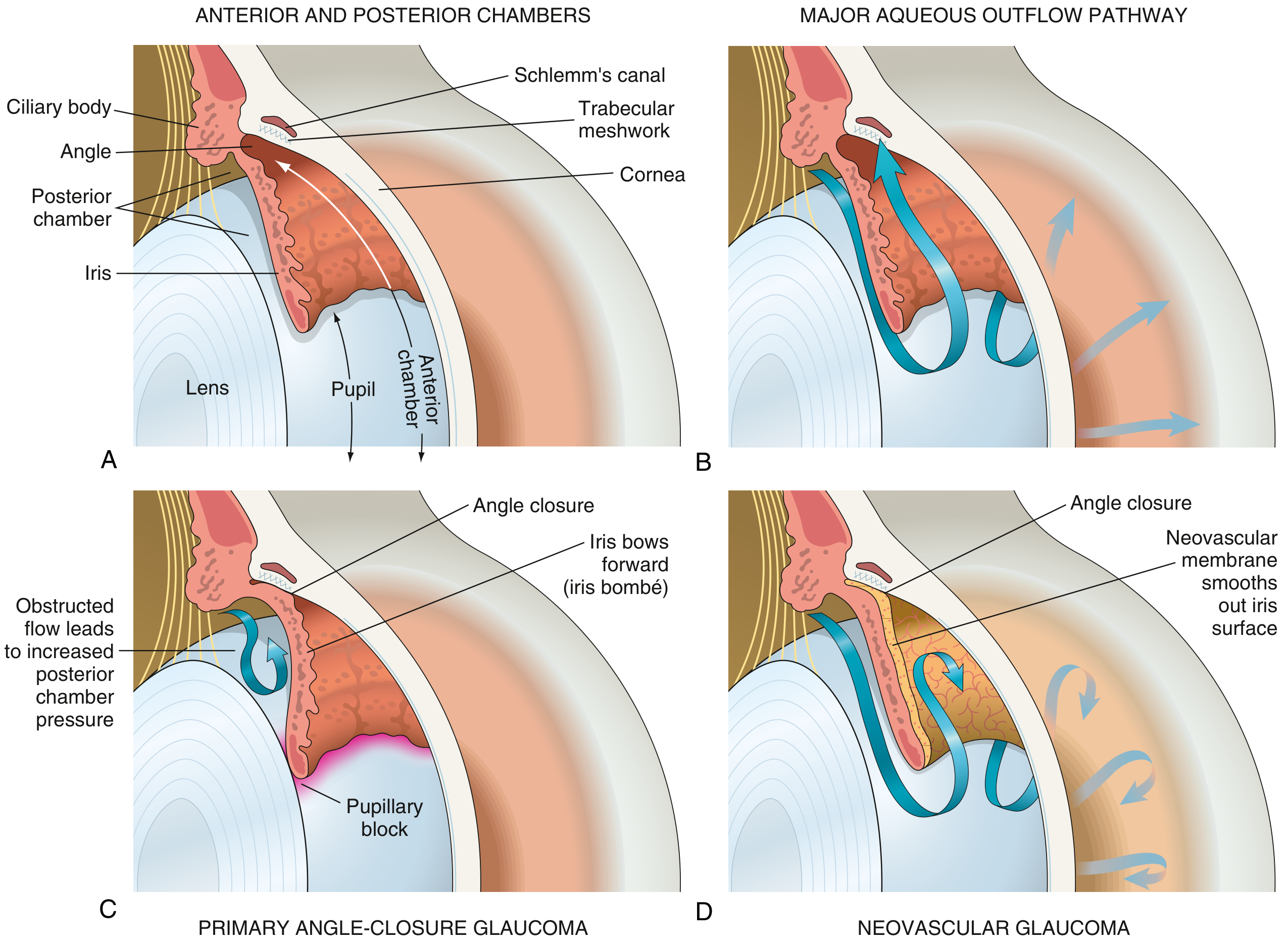
Fig: (A) Normal eye anatomy. (B) Normal aqueous humor outflow. (C) Primary angle-closure glaucoma with iris bombé and pupillary block. (D) Neovascular glaucoma with neovascular membrane covering the trabecular meshwork.
What is Glaucoma?
Glaucoma refers to a collection of diseases in which optic neuropathy - progressive damage to retinal ganglion cells and their axons - is usually associated with elevated intraocular pressure (IOP). The primary site of damage is at the lamina cribrosa, where optic nerve axons exit the eye. The result is enlargement of the optic cup (increased cup-to-disc ratio) and characteristic visual field loss, initially peripheral, then central.
- Goldman-Cecil Medicine, p. 610-612
- Robbins & Kumar Basic Pathology, p. 869
Causes and Risk Factors
Pathophysiology
Aqueous humor is produced by the ciliary body and flows from the posterior chamber through the pupil into the anterior chamber. It drains mainly through the trabecular meshwork into Schlemm's canal, then into venous circulation. Imbalance between production and drainage raises IOP, which damages retinal ganglion cells.
Types and Their Causes
1. Primary Open-Angle Glaucoma (POAG) - Most Common
- Aqueous has apparent free anatomic access to the trabecular meshwork, but increased resistance to outflow exists
- Most common in elderly; often asymptomatic until late-stage
- Risk factors: African ancestry, older age, low blood pressure, myopia, genetic predisposition, disc hemorrhages, ocular hypertension (IOP >21 mmHg), thin corneas
2. Primary Angle-Closure Glaucoma
- Common in patients with hyperopia (shallow anterior chamber)
- Transient iris apposition to the lens blocks aqueous flow from posterior to anterior chamber
- Pressure builds in the posterior chamber, causing the iris to bow forward (iris bombé), occluding the trabecular meshwork
- Can present acutely with pain, red eye, and rapid vision loss
3. Secondary Open-Angle Glaucoma
- Deposition of particulate matter (e.g., red blood cells after trauma, necrotic tumor cells) blocks outflow
- Also caused by corticosteroid use, pigment dispersion, pseudoexfoliation syndrome
4. Secondary Angle-Closure Glaucoma (e.g., Neovascular Glaucoma)
- A neovascular membrane (driven by VEGF upregulation in chronic retinal ischemia - e.g., from diabetic retinopathy or central retinal vein occlusion) grows over the iris surface
- Myofibroblasts within it contract, pulling the iris over the trabecular meshwork (peripheral anterior synechiae)
- Aqueous outflow is completely blocked
5. Normal-Tension Glaucoma
-
Characteristic optic nerve and visual field changes despite normal IOP; thought to involve vascular insufficiency and optic nerve vulnerability
-
Robbins & Kumar Basic Pathology, p. 869-870
-
Goldman-Cecil Medicine, p. 612-616
Treatment
The primary goal of treatment is to reduce intraocular pressure.
Medical Treatment (First-Line)
| Drug Class | Examples | Mechanism |
|---|---|---|
| Prostaglandin analogues (first choice) | Latanoprost, bimatoprost, travoprost, tafluprost | Increase aqueous outflow; once-daily dosing, low side effects |
| Beta-blockers | Timolol, betaxolol, levobunolol | Decrease aqueous secretion from ciliary epithelium |
| Alpha-2 agonists | Brimonidine, apraclonidine | Decrease aqueous secretion + increase outflow |
| Carbonic anhydrase inhibitors | Dorzolamide (topical), acetazolamide (oral) | Decrease aqueous secretion |
| Rho-kinase inhibitors | Netarsudil | Increase outflow (newer agent) |
| Cholinomimetics | Pilocarpine, carbachol | Ciliary muscle contraction opens trabecular meshwork |
Prostaglandin analogues are currently the drugs of choice to initiate treatment - effective, once-daily dosing, and low adverse effect profile. Beta-blockers should be used with caution in patients with bradycardia, heart block, heart failure, or asthma.
- Katzung's Basic and Clinical Pharmacology, p. 256
Laser Treatment
- Laser trabeculoplasty (LTP): Applies laser energy to the trabecular meshwork to enhance outflow drainage. Often a first-line or add-on option in open-angle glaucoma.
- Laser iridotomy/peripheral iridectomy: Creates a hole in the iris to relieve pupillary block in angle-closure glaucoma - both as emergency treatment and prophylaxis.
- Diode laser cycloablation: Destroys part of the ciliary body to reduce aqueous production; reserved for refractory cases.
Surgical Treatment
- Trabeculectomy: Creates a new drainage channel; often combined with mitomycin C to prevent scarring. Standard surgical option for refractory glaucoma.
- Combined trabeculectomy-trabeculotomy: Used in congenital/developmental glaucoma (e.g., Sturge-Weber syndrome).
- Glaucoma drainage devices (tube shunts): Ahmed, Baerveldt, Molteno implants; provide best long-term IOP control, especially in uveitic or neovascular glaucoma. A 2024 systematic review in Am J Ophthalmol (PMID: 39293570) found tube shunts comparable or superior to trabeculectomy in uveitic glaucoma.
- Goniotomy: Used in early congenital glaucoma with angle anomalies.
Acute Angle-Closure Emergency
-
IV acetazolamide + hyperosmotic agents (mannitol) to rapidly lower IOP
-
Followed by laser iridotomy to relieve the pupillary block
-
Goldman-Cecil Medicine, p. 624-625
Complications
| Complication | Details |
|---|---|
| Blindness (irreversible) | The end-stage of untreated or uncontrolled glaucoma; second leading cause of blindness worldwide |
| Visual field loss | Starts peripherally, progresses centrally; often unnoticed until severe |
| Optic nerve atrophy | Diffuse loss of ganglion cells and thinning of the retinal nerve fiber layer; optic disc becomes cupped and atrophic |
| Corneal edema/bullous keratopathy | Acute IOP spikes (especially in angle-closure) can cause corneal endothelial damage |
| Cataract | Secondary to chronic elevated IOP, medications, or surgical intervention |
| Buphthalmos | Globe enlargement from chronically elevated IOP in infants (congenital glaucoma) |
| Treatment complications | Trabeculectomy can cause choroidal effusion, suprachoroidal hemorrhage, or wound leak; tube shunts can erode through conjunctiva; topical beta-blockers can cause systemic bradycardia/bronchospasm |
| Amblyopia | In children with congenital glaucoma if untreated early |
- Robbins & Kumar Basic Pathology, p. 870
- Goldman-Cecil Medicine, p. 614-625
Key Summary Points
- Glaucoma is an optic neuropathy, most often caused by elevated IOP damaging retinal ganglion cells at the lamina cribrosa.
- Primary open-angle glaucoma is the most common type - chronic and asymptomatic until late stages.
- Angle-closure glaucoma is an emergency when acute.
- Treatment is lifelong for most patients - prostaglandin analogs are first-line, supplemented by laser or surgery when needed.
- The disease is largely preventable from causing blindness when detected and managed early - the major challenge is its asymptomatic nature.
This is a shared conversation. Sign in to Orris to start your own chat.