Lucid interval in extra dural hemorrhage
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough explanation of the lucid interval in extradural hemorrhage (EDH), drawn directly from authoritative surgical and anatomy textbooks.
Lucid Interval in Extradural Hemorrhage
Definition
The lucid interval is the period of apparent normal consciousness that occurs between an initial loss of consciousness (due to cerebral concussion at the time of impact) and the subsequent deterioration into coma caused by the expanding extradural hematoma.
Mechanism
The classic sequence of events:
-
Initial impact - A lateral blow to the head (most commonly the temporal region) fractures the thin squamous temporal bone, tearing the middle meningeal artery (most often its anterior branch). This causes an immediate, brief loss of consciousness from the concussive force.
-
Lucid interval begins - As the arterial blood begins to collect between the periosteal layer of the dura and the calvaria (skull), the dura is slowly stripped away. During this phase, intracranial pressure (ICP) remains near normal because cerebrospinal fluid (CSF) is displaced into the spinal canal - a compensatory mechanism described by the Monro-Kellie doctrine. The patient regains consciousness and may appear entirely normal, perhaps complaining only of headache with no neurological deficit. This phase lasts hours (classically a few hours for arterial EDH).
-
Compensation fails - As the hematoma continues to expand under arterial pressure, CSF displacement can no longer compensate. ICP rises sharply.
-
Herniation and deterioration - The medial aspect of the temporal lobe herniates through the tentorial hiatus (uncal herniation), compressing:
- The reticular activating system in the midbrain - causing progressive drowsiness, confusion, then coma
- The ipsilateral oculomotor nerve (CN III) - causing initial pupillary constriction then rapid dilation (ipsilateral "blown" pupil)
- The contralateral crus of the midbrain against the opposite tentorial edge (Kernohan's notch) - causing hemiplegia on the same side as the lesion (a false localizing sign), occurring late
-
Terminal signs - Fixed dilated pupils bilaterally, decerebrate rigidity, Cushing's triad (hypertension, bradycardia, irregular respiration)
Sequence of Motor Involvement
When the anterior branch of the middle meningeal artery bleeds, the hematoma presses on the motor cortex from below upward, producing a progressive contralateral hemiplegia starting with:
- Face first
- Then arm
- Then trunk
- Then leg
Duration of the Lucid Interval
The duration varies depending on the type and calibre of the vessel injured:
- Arterial bleeding (middle meningeal artery) - lucid interval of a few hours; rapid deterioration
- Venous bleeding (diploic veins, venous sinuses) - slower accumulation, longer or more indistinct lucid interval
Why EDH Has a More Classic Lucid Interval than SDH
| Feature | Extradural Hemorrhage | Subdural Hemorrhage |
|---|---|---|
| Source | Middle meningeal artery (arterial) | Superior cerebral veins (venous) |
| Incidence | Less common | ~6x more common |
| Speed of accumulation | Slower initially (dura stripped gradually) | Accumulates quickly |
| Lucid interval | Present and classic (hours) | Much shorter or absent |
| Signs of compression | Appear later | Appear earlier |
| Compensation | CSF displacement allows period of normalcy | Little time for compensation |
"In extradural haemorrhage after a period of initial unconsciousness (stage of cerebral concussion), there will be a stage of consciousness in which the patient behaves normally (lucid interval). During this lucid interval the duramater is slowly stripped off the skull by the accumulating blood, but the intracranial pressure continues to be normal by displacement of the cerebrospinal fluid into the spinal canal. When this compensation fails, intracranial pressure increases..." - S Das, A Manual on Clinical Surgery
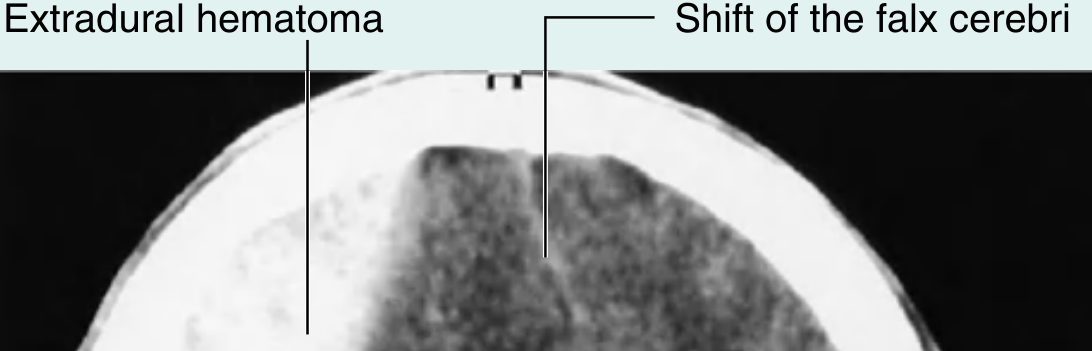
CT Appearance
On CT scan, an EDH appears as a biconvex (lens-shaped/lenticular) hyperdense lesion between the skull and the brain, constrained by the firm dural attachments at the suture lines. Midline shift (shift of the falx cerebri) may be evident.
Clinical Significance - "Talk and Die"
This pattern is classically called the "talk and die" syndrome. Although it occurs in only about one-third of EDH cases, it is critically important because:
- The patient appears neurologically intact during the lucid interval
- Rapid, avoidable secondary brain injury follows if not recognized
- Prompt evacuation of the hematoma (before herniation is established) carries an excellent prognosis
Side Localisation
The side of hemorrhage is identified by:
- Side of the skull fracture on X-ray (fracture line crossing the middle meningeal groove in the temporal bone)
- Side of boggy swelling under the temporal muscle
- Side of initial pupillary dilation (ipsilateral CN III compression)
Sources:
- S Das: A Manual on Clinical Surgery, 13th Edition, pp. 272-274
- Bailey and Love's Short Practice of Surgery, 28th Edition, p. 387
- Gray's Anatomy for Students, p. 1029
This is a shared conversation. Sign in to Orris to start your own chat.